Natural history and clinical manifestations
As in adults, HIV-infected children present with a spectrum of signs and symptoms reflected in the revised Centre for Disease Control classification system (Box 12.3). The differences between adults and children with HIV disease are summarised (Box 12.4).
In the absence of HAART, disease progression is generally faster than in adults, with 15—20% of childrenBox 12.3 Centers for Disease Control 1994 revised classification system for HIV infection in children less than 13 years old
Category N: no symptoms
Category A: mildly symptomatic
• Lymphadenopathy
• Hepatomegaly
• Splenomegaly
• Dermatitis
• Parotitis
• Recurrent upper respiratory tract infections, sinusitis or otitis media
Category B: moderately symptomatic
Examples of conditions in clinical category B include:
• Anaemia, neutropenia or thrombocytopenia
• Bacterial infections: pneumonia, bacteraemia (single episode)
• Candidiasis, oropharyngeal
• Cardiomyopathy
• Diarrhoea, recurrent or chronic
• Hepatatis
• Herpes stomatitis, recurrent
• Lymphoid inter stitial pneumonia
• Nephropathy
• Persistent fever > 1 month
• Varicella (persistent or complicated primary chickenpox or shingles)
Category C: severely symptomatic
Any condition listed in the 1987 surveilllance case definition for AIDS, with the exception of LIP. For example:
• Serious bacterial infections, multiple or recurrent
• Candidiasis (oesophageal, pulmonar y)
• Cytomegalovirus disease with onset of symptoms at age >1 month
• Cryptosporidiosis or Isosporiasis with diarrhoea persisting 1 month
• Encephalopathy
• Lymphoma
• Mycobacterium tuberculosis disseminated or extrapulmonary
• Mycobacterium avium complex or M. kansasii, disseminated
• Pneumocystis carinii pneumonia
• Progressive multifocal leucoencephalopathy
• Toxoplasmosis of the brain with onset at age > 1 month
• Wasting syndrome developing AIDS-defιning illnesses by 12 months.
This subset of perinatally infected children typically present with PCP at around three to four months of age (Figure 12.8). Progression rates to AIDS in infancy have been shown to be reduced by the use of primary PCP prophylaxis with Septrin from 4 to 6 weeks of age onwards.Approximately 70% of perinatally infected children will have some signs or symptoms by 12 months (Figure 12.14). In the absence of antiretroviral therapy, the median age at which children progress to AIDS is about six years, and 25—30% have died by this age. The median age of death is around nine years. In many cases, the child is the first family member to be diagnosed as HIV infected. Some children, however, do not present until the second decade of life. Disease progression in children in developing countries is more rapid (Figure 12.15). Survival following an AIDS diagnosis has greatly improved over the past 10 years, but even where antiretroviral therapy is available the mortality amongst children with PCP and CMV is appreciable (Figure 12.13). This is yet another reason for antenatal HIV testing which can render PCP in infancy wholly preventable.
Children with HIV infection frequently present with signs and symptoms that are common in general paediatrics and are non-specific. The most usual clinical features associated with HIV infection include persistent generalised lymphadenopathy, hepatosplenomegaly, chronic or recurrent diarrhoea, fever, and recurrent otitis or sinusitis.
Persistent oral candidiasis, bilateral parotitis or neurological signs are more specific of HIV infection. Herpes zoster (shingles) in childhood is uncommon and suggests a defect in cellular immunity justifying an HIV test in the absence of other explanations. Similarly, thrombocytopenia can be a presenting feature, and HIV should be considered in the differential diagnosis of idiopathic thrombocytopenic purpura.
Recurrent and often severe bacterial infections are frequent and include pneumonia, cellulitis, local abscesses, osteomyelitis, septic arthritis and occult bacteraemia.
The common causative organisms are similar to those seen in children with hypogammaglobulinaemia and include pneumococci, salmonellae, staphylococci, streptococci and Haemophilus influenzae. This reflects the B-cell defect that accompanies the destruction of the CD4+ helper T cells. Children with HIV infection frequently have hypergammaglobulinaemia due to dysregulated polyclonal B-cell activation. The antibodies are generally non-functional.Pulmonary disease is an important cause of morbidity and mortality and may be one of the first manifestations. Lymphoid interstitial pneumonitis (LIP), characterised by multiple foci of proliferating lymphocytes in the lung interstitium, occurs in 20—30% of vertically infected children, but is rare in adults. It presents with persistent bilateral reticulonodular shadowing on chest X-ray (Figure 12.9) and clinical features ranging from asymptomatic to chronic hypoxia. It may be an abnormal response to primary Epstein-Barr virus (EBV) infection. Coinfection with Mycobacterium tuberculosis is an increasing problem in children, and can be difficult to distinguish radiologically from LIP. Clinically a child with bilateral infiltrates due to TB would be highly symptomatic, as opposed to LIP which may be clinically silent.
Opportunistic infections, apart from PCP and primary disseminated CMV disease in the subset of children with very rapid disease progression, are usually a late complication of HIV infection and result from severe immunosuppression. The most common are oesophageal candidiasis, multidermatomal varicella zoster, disseminated mycobacterium avium complex (MAC) or CMV infections, cryptosporidiosis, and more rarely,
Box 12.4 Differences between children and adults with HIV disease
• More rapid disease progression:
20% of children develop AIDS by 12 months Child may be the first family member to present
• Higher viral loads at presentation
• Physiologically higher absolute CD4 counts
• Growth faltering common (affects height and weight)
• Encephalopathy presents with developmental delay and hypertonic diplegia
• Opportunistic pathogens encountered for the first time
primary illnesses often more severe than OIs in adults
• Poor primary responses to childhood infections/immunisations
• Lymphoid interstitial pneumonitis common
• Malignancy uncommon (accounts for less than 2% of AIDS- defining presentations in children)
• More rapid clearance of antiretroviral drugs, requiring higher than adult equivalent doses particularly in very young children
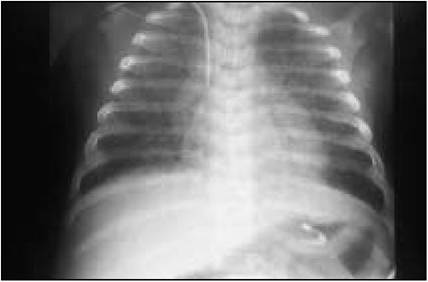
Figure 12.8 Pneumocystis carinii pneumonia (PCP) in a three month old.
Diffuse bilateral ground-glass opacification, tending to confluence in right upper and both lower lobes. Air bronchograms are seen, which imply air space disease which is a late feature of disease. The earliest infiltrates are usually perihilar. The absence of pleural effusion or hilar adenopathy is typical. Less typical presentations include miliary, coin and nodular lesions, lobar consolidation and cavitations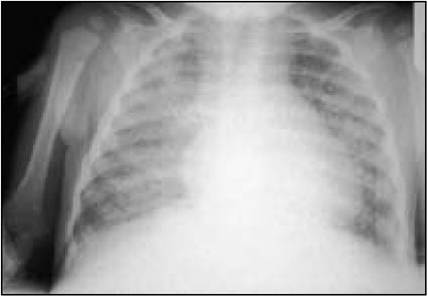
Figure 12.9 Lymphoid interstitial pneumonitis (LIP) in a child aged 12 months. Diffuse, well-circumscribed nodules distributed uniformly throughout both lung fields. May be associated with hilar adenopathy. A radiological spectrum is seen in LIP, ranging from fine linear interstitial infiltrates to large nodules that tend to confluence in the right middle and lingular lobes
toxoplasmosis. MAC should be considered in any child with advanced disease and unexplained fevers, weight loss and abdominal discomfort.
Encephalopathy due to effects of HIV infection on the central nervous system is seen most frequently in the subgroup of children with rapid disease progression. The most common neurological manifestations are hypertonic diplegia, developmental delay (particularly affecting motor skills and expressive language) or acquired microcephaly. Cranial imaging studies may show basal ganglia calcification and cerebral atrophy and MRI scans may show evidence of white matter damage. Seizures are not usually a feature of HIV encephalopathy which does not tend to affect the grey matter. The majority of school age children are attending normal school without requiring additional support in the classroom.
Malignancy, such as Kaposi's sarcoma or lymphoma, is a relatively uncommon feature of paediatric HIV disease, accounting for only 1—2% of AIDS-defining illness in children.