Diagnosis
IgG antibodies to HIV are passively transferred to virtually all babies born to infected mothers, unless they are born extremely preterm or the mother has profound hypogammaglobulinaemia.
Standard IgG antibody assays are so sensitive that traces ofEstimated vertical transmission rate (95% CI) in UK over time in non-breast-feeding women
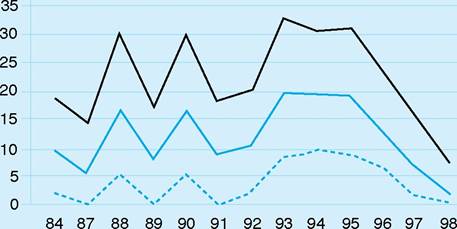
Figure 12.5 Estimated vertical transmission rate (95% CI) in UK over time in non-breastfeeding women (from Doung, BMJ 1999)
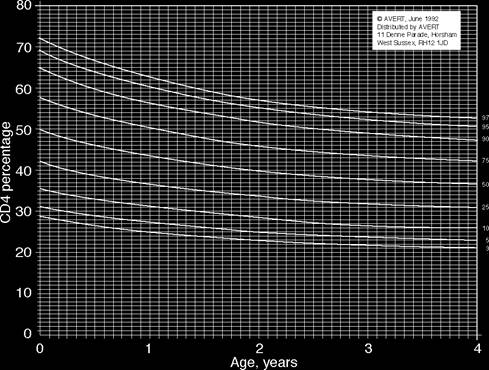
Figure 12.6 Normal ranges for CD4+ lymphocyte percentages in HIV- uninfected children born to HIV-infected mothers.
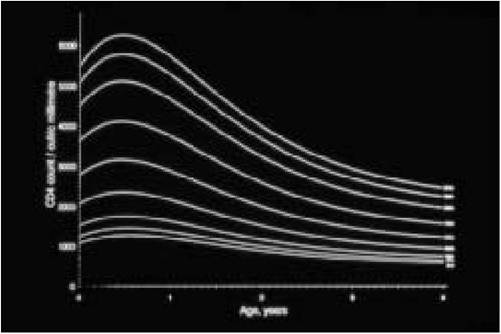
Figure 12.7 Normal ranges for absolute CD4+ lymphocyte counts in HIV- uninfected children born to HIV-infected mothers. Source: European Collaborative Study
Table 12.2 Suggested follow-up of infants born to HIV-infected mothers
| Age | Action Comment |
| Birth to 4—6 weeks 24-48 hours | Give antiretroviral prophylaxis to baby Usually zidovudine monotherapy, but modified in light of maternal therapy Proviral DNA PCR* If positive, suggests intrauterine transmission or high intrapartum innoculum: may be associated with more rapid disease progression. Not helpful if negative, as less than 50% of infected babies can be detected within 48 hours of birth |
| 3-6 weeks | Proviral DNA PCR Should detect 95% of infected infants. A positive result must be confirmed on two separate blood samples |
| 4-6 weeks | Stop antiretroviral prophylaxis. Start See text for PCP prophylaxis recommendations PCP prophylaxis** |
| 3-4 months | Proviral DNA PCR If all assays are negative and there are no clinical concerns, child is almost certainly uninfected. PCP prophylaxis can be stopped |
| 18 months | HIV antibody test Perfor med until serorever sion documented |
*Initial infant sample should be tested in parallel with maternal sample obtained around the time of delivery, to ensure maternal strain of HIV can be detected.
**For very low risk infants paediatric specialists increasingly are not recommending PCP prophylaxis.
maternal antibody are frequently detectable in the baby up to 18 months of age. Waiting for antibodies to become undetectable (“seroreversion”) is therefore a slow way to establish the child's infection status. Using techniques that detect proviral HIV DNA, by polymerase chain reaction (PCR) or other amplification techniques, 93% of infected infants can be diagnosed by one month of age, and virtually all by three months. Quantitative RNA assays are now widely available but are not licensed for diagnostic purposes because of problems with false positive results and variable performance with non-B clade viral isolates. Whichever test is used, it is essential to ensure that it efficiently detects the maternal strain of HIV.
Virus culture is a highly specialised assay that is available only in research laboratories and has been largely superseded by amplification assays. Immune complex dissociated p24 antigen assays (ICD p24 ag) detect the nuclear capsid antigen of the virus by a commercial ELISA kit. This is a cheap but less sensitive method of diagnosis. Similarly IgA assays are highly specific but lack sensitivity, particularly during the first three months of life.
If PCR assays which reliably detect the mother's strain of HIV are negative on the infant's blood at three different time points, with at least one set performed at or after three months of age, and there are no clinical concerns, the parents/guardians can be informed that their baby is almost certainly not infected (Table 12.2).
T-cell subsets and measurement of immunoglobulins (Ig) are non-specific tests. Reversal of the CD4 : 8 ratio and high Ig (>2 ? upper limit of normal) are suggestive of infection but, for diagnostic purposes, should be supported by at least one other test that detects the virus directly. It is important to realise that absolute CD4 counts are physiologically much higher in infants and young children than in adults (Figures 12.7 and 12.8).
All children presumed to be uninfected should be followed until seroreversion is confirmed, and longer term follow-up to ensure normal development until four to five years is advised in children exposed to ART perinatally.
More on the topic Diagnosis:
- Adhikari S.. Diagnosketch: A Visual Guide to Medical Diagnosis for the Non-Medical Audience Oxford: Oxford University Press,2022. — 665 p., 2022
- Diagnosis of Bovine Tuberculosis in Zambia
- Voluntary counselling and HIV testing
- Bovine Tuberculosis in Uganda
- Prevalence and Epidemiology of BTB in Rwanda
- Bovine Tuberculosis in Zambian Wildlife
- Tetanus