Antenatal testing and mother-to-child transmission
Most observational studies estimate the risk of MTCT without interventions to be around 15—20% in Europe and the USA and over 30% in African populations. Postnatal breastfeeding doubles the overall risk of transmission and accounts for most of the difference.
In non-breastfeeding women, approximately 75% of perinatal transmission occurs around the time of delivery. Other factors independently affecting the rate of transmission include the HIV viral load and CD4 cell count of the mother at the time of delivery, duration of rupture of membranes, prematurity and mode of delivery. In the last five years, the MTCT rate has been reduced to less than 2% in the USA and most European countries by the introduction of antenatal testing, highly active antiretroviral therapy (HAART) for mother's requiring therapy, use of antiretroviral therapy perinatally even if not indicated on the grounds of the mother's disease status, delivery by elective caesarean section, and refraining from breastfeeding. A recommendation that HIV testing should be offered to all women in pregnancy has been successfully implemented in many European countries, notably France, Italy and Spain where the prevalence of HIV in pregnant women was highest.In the UK, universal offer of HIV testing during the antenatal period has been recommended in London because of the high prevalence since 1992. However, until 1999, it was recommended that antenatal HIV testing should only be offered to women considered at high risk (selective testing) outside London. An economic analysis was published in 1999 showing that a universal offer policy was cost-effective throughout the UK provided that a high uptake of testing was achieved. Department of Health guidelines endorsing this approach were published in August 1999. In low prevalence areas, up to 50 pooled samples can be tested in batches to reduce costs.
During most of the 1990s, detection of previously undiagnosed HIV in pregnancy has been low everywhere in the UK. However, during 1999, and more dramatically, during the first half of 2000, there has been a marked improvement in antenatal detection rates, with about 75% of all HIV infected women being aware of their diagnosis before their baby is born in inner London and Scotland, 66% in outer London and about 50% elsewhere in the UK. In most European countries and in the USA, a marked decrease in AIDS cases reported in infancy reflects the high proportion of pregnant women receiving appropriate care to reduce MTCT.Among UK women who either knew their HIV status before pregnancy or are diagnosed during pregnancy, MTCT rates of 2% or less are being reported among those taking up
Box 12.2 Interventions to reduce transmission from mother-to-child
• Not breastfeeding
• Antiretroviral therapy
• Elective caesarean section delivery (ie before the onset of labour or membrane rupture)
• IMPLEMENTING ALL 3 CAN REDUCE TRANSMISSION RATES TO 2% OR LESS
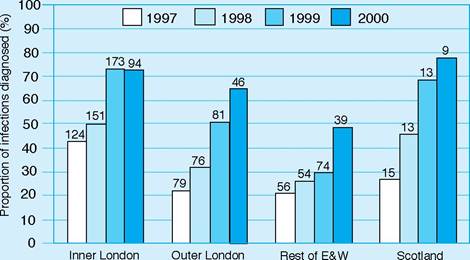
Figure 12.3 Proportion of HIV infections diagnosed prior to birth among pregnant women
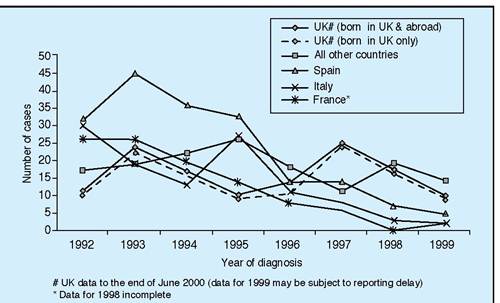
Figure 12.4 Mother-to-child HIV transmission in European countries: AIDS cases in children aged less than 1 year at diagnosis. Source: European Nonaggregate AIDS data set. June 1999. European Centre for the Epidemiological Monitoring of AIDS, Saint Maurice, France
interventions. Women taking HAART for their own disease who have undetectable HIV viral load at delivery have a very low risk of transmitting HIV to their baby. For those women not needing therapy for themselves, most guidelines recommend zidovudine and elective caesarean section (CS) delivery, which limits exposure of mother and baby to antiretroviral drugs and is associated with a transmission rate of CS delivery remains unclear.
There is probably no place for dual ART with ZDV and 3TC in pregnancy, as this is rarely able to fully inhibit viral replication, adds little to reducing transmission with ZDV and elective CS, increases the potential for toxicity in the infant and has been associated with rapid selection of 3TC-associated mutants.In the developing world, a number of major studies have evaluated the efficacy of cheaper and less complicated perinatal ART regimens. These include short-course ZDV and most notably the use of a single dose of the non-nucleoside reverse transcriptase inhibitor (NNRTI) drug nevirapine to the mother during labour and to the infant within the first three days of birth. This extremely cheap regimen has been shown to reduce transmission by nearly 40% compared with a regimen of intrapartum and neonatal ZDV for a week, even in breastfeeding women over a period of 12 months. It is now being implemented alongside antenatal HIV testing programmes in many parts of the developing world. A concern that resistance to nevirapine, which occurred in about 15% of women, might compromise its use in subsequent pregnancies is probably unfounded as virus returns to wild type in the months following delivery. However, there are concerns that giving a single dose of nevirapine during labour in addition to other ART to women in Europe and the USA who fail to achieve undetectable viral load, could compromise the woman's future ART options to any NNRTI drug because of the rapid selection of HIV strains resistant to nevirapine even after a single dose. Resistance testing to guide therapy choice is routinely recommended for all HIV-infected pregnant women in many developed countries because of de novo acquisition of drugresistant strains of HIV-1.
More on the topic Antenatal testing and mother-to-child transmission:
- ESSENTIAL ANTENATAL CARE
- CHILD ABUSE AND NEGLECT (CHILD MALTREATMENT)
- UNICEF has called child sexual assault ‘a fundamental violation of children's rights',1 while the World Health Organization (WHO) has named it a ‘serious infringement on a child's right to health and protection'.[234] [235]
- The Mother Goddess of the Tribes
- Voluntary counselling and HIV testing
- The physiatric history and examination of a child require a blend of medical diagnostic skills to establish or confirm the diagnosis as well as a knowledge of child development and behavior to evaluate functional assets and difficulties for the intervention phase of rehabilitation.
- KANGAROO MOTHER CARE
- E. Cybele, the Great Mother
- B. Mary, the Mother of God
- BACTERIAL AND VIRAL TRANSMISSION PATTERNS
- Genetic Testing
- A. Mary as Virgin Mother
- Testing of patients and blood donors
- CHAPTER IV THE GREAT MOTHER AND MONTANISM
- CASE 224: A Worried Mother
- Transmission
- B. Montanism, the Great Mother and the Virgin Mary
- TRANSMISSION OF TERRESTRIAL AND BAT RABIES
- The Spirit as Mother in Early Syriac-Speaking Christianity
- Possible Forms of the Cultural Transmission Term