Ischemic Cerebrovascular Events
Clinicopathological Aspects
There is no peculiar clinical presentation of HIV-1-related strokes [9, 27], although they are usually asymptomatic, and not diagnosed prior time to death [13, 31].
Hemiparesis, hemiplegia, and hemianesthesia are the most common presenting signs. Encephalopathy seems more common in cerebral infarction [27], whereas headache, language disturbance, and abnormal vision are more common in TND [27, 43]. A transient chorea has exceptionally been reported as a TND [48]. TNDs can be isolated [43, 46, 49] but are more frequently recurrent [42, 44]. Their association with PIs is controversial [50]. Although rarely reported as the presenting manifestation of HIV infection [14, 51], stroke was the first manifestation of HIV-1 in up to 40 and 50% of South African patients described by Tipping et al. [15] and Mochan et al. [52], respectively. Infarcts are usually lacunar rather than infarcts in large-vessel territories [9,13, 31]. In a retrospective study, 19% of patients had a small vessel occlusion and 12% had large artery atherosclerosis [14]. Yet, in a prospective clinical study of black heterosexual nonintravenous drug users, 61% of ischemic strokes were large-vessel infarcts with cortical involvement and only 39% were small-vessel infarcts with subcortical involvement [52]. These findings have also been observed in another black population cohort [19]. Autopsy series confirm, however, that infarcts are usually small, located in the basal ganglia or the thalamus and the deep white matter, more rarely in the brain stem or the cerebellum, and frequently multiple [31]. Occlusion of large vessels seems to be less frequent [14, 19, 47, 52].Mechanisms of Ischemic Stroke
The exact distribution of the different causes of strokes in HIV-1 infection cannot be determined because a thorough exploration has not always been performed in published series.
For example, in the recent series of Ortiz et al. [14], brain MRI was performed in only 57% of patients and 39% underwent lumbar puncture. Even recent clinical series are not entirely comparable. In some, previous HIV infection is documented in 91% of patients, the mean CD4 count is In others, stroke results in the first diagnosis of HIV infection in 42% of patients, CD4 counts are > 200 in 54% of patients, and opportunistic infections defining AIDS occurred in 28% of them [15]. This is partly explained by discrepancies in demographic data and availability of antiretroviral therapies. Traditional risk factors for vascular disease have relatively low prevalence, and conversely, mechanisms unusual in the general population such as infection, vasculitis and hypercoagulability, play a greater role in HIV- infected patients [14, 15]. However, two causes emerge: cardioembolism and vasculi- tis/vasculopathy [9] (see Table 1).Table 1 Causes of ischemic stroke in HIV-infected patients
Cardioembolism
Infectious and noninfectious endocarditis
Cardiomyopathy
HIV myocarditis
Myxoid valvular degeneration
Arrhythmias
Mural thrombi
Intra-atrial septal defect
Patent Foramen ovale
Hematological
Protein S deficiency
Antiphospholipid antibodies
Disseminated intravascular coagulation
Neoplasm
Hyperviscosity syndrome
Vasculitis
Opportunistic infections
Aspergillosis
Candidiasis
Cytomegalovirus
Cryptococcosis
Herpes simplex virus
Mucormycosis
Syphilis
Toxoplasmosis
Trypanosomiasis
Tuberculosis
Varicella-zoster virus
Neoplasm
Non-Hodgkin’s lymphoma
HIV-related vasculitis
HIV itself
Immune reconstitution
Premature atherosclerosis with protease inhibitors
Dyslipidemia
Insulin resistance
Endothelial dysfunction
Hyperhomocysteinemia
Drugs (especially cocaine and heroin)
Cryptogenic
Cardioembolism
Cardiac disease may be found in as many as 50% of AIDS patients [53], and is regarded as the main cause of embolic stroke (Fig.
1) in HIV-1-infected individuals [33]. It includes viral myocarditis, bacterial and nonbacterial (marantic) endocarditis (both with and without history of intravenous drug abuse), dilated cardiomyopathy, mural thrombi, myxoid degeneration of the valves, and HIV myocarditis [8, 9, 17, 27, 33, 53]. Dilated cardiomyopathy was deemed the responsible mechanism for stroke in almost 20% of patients in the series of Ortiz et al.[14]. Conversely, in another recent study
[15], cardioembolism was a cause of cerebral infarction in only 10% of patients, and appeared less common in this population than in the HIV negative patients. Aortic root dilatation associated with left ventricular dilatation, increased viral load, and lower CD4 cell count, documented in HIV-1- infected children [54], has not been described in adults.
Opportunistic/Tumoral VasculitisZVasculopathy
Vasculitic changes in intracerebral vessels associated with ischemic strokes can be due to opportunistic infections as diverse as tuberculosis, cytomegalovirus, varicellazoster virus (Fig. 2), herpes simplex virus, syphilis, cryptococcosis, candidiasis, aspergillosis, mucormycosis, coccidioidomycosis, and trypanosomiasis (reviewed in [9, 34]). Several cases of lymphomatoid granulomatosis and malignant lymphoma have also been associated with infarcts [9, 34, 55]. Although the frequency of nervous system opportunistic infections and neoplasms has dramatically decreased with the current use of combined multitherapies in Western countries [2], infectious vasculitis remains relatively common in HIV-infected patients with stroke and advanced immunodepression and is generally predictive of poor outcome [14]. This argues for performing lumbar puncture in these cases [14].
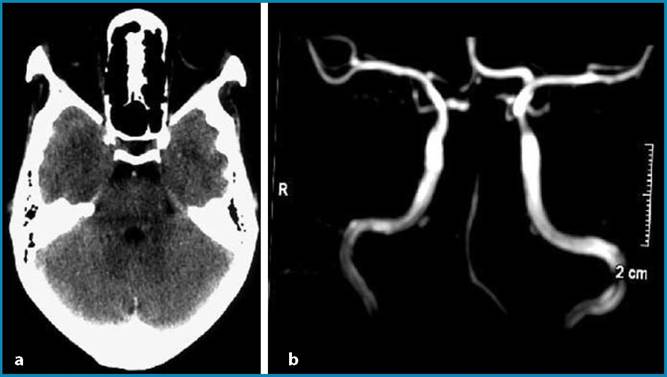
Fig. 1a, b Cardioembolic acute basilar artery occlusion. a Noncontrast CT scan shows a spontaneous hyperdensity of the basilar artery. b MR angiogram shows the acute basilar artery occlusion
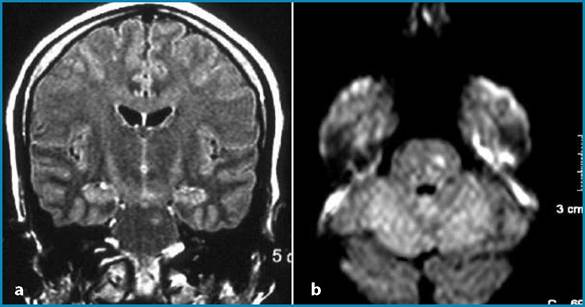
Fig.
2a,b Varicella-zoster virus- related lacunar infarct in the pons. a Fluid-attenuated inversion recovery MR image obtained in the coronal plane shows a left infarct in the pons. b Diffusion- weighted MR image shows a recent ischemic stroke in the ponsHIV-Related Vasculitis/Vasculopathy
The frequent formation of cotton-wool spots in HIV-1-infected patients’ eyes is ascribed to vasculitis-induced ischemic injury [56]. Indeed, in some cases, HIV-1 itself appears to be the cause of vasculitis [18, 36, 57-59]. As part of the immunodepression caused by the virus, a granulomatous inflammation involving small arteries and veins of the brain surface and leptomeninges, termed primary angiitis of the central nervous system (CNS), is a rare vasculitis (less than 25 cases reported, principally reviewed in [59]) usually associated with high mortality [59], although a benign course has been described [49]. Moreover, two patients in the series of Evers et al. [18] had fluctuating intracranial stenosis which resolved within months, suggesting an inflammatory origin. It has been reported once that HIV-1 vasculitis could principally concern the cerebral posterior circulation [60]. The pathogenesis of primary angiitis of the CNS is speculative and mechanisms such as infection of endothelial cells by HIV-1, increased deposition of circulating immune complexes, and impaired regulation of cytokines and adhesion molecules have been proposed [61]. For others, cerebral vasculitis in the absence of infections or tumors is controversial [35]. Immune reconstitution promoted by HAART may exceptionally induce cerebral vasculitis (Fig. 3) in HIV-infected patients [62, 63].
Evidence supports the occurrence of a vasculopathy involving the CNS small vessels in HIV-1-infected patients free of risk factors for these vascular changes [31]. The autopsy series of the Edinburgh HIV Cohort revealed the presence of an asymptomatic vasculopathy characterized by small-vessel wall thickening, perivascular space dilatation, rarefaction and pigment deposition with vessel wall mineralization, and occasional perivascular inflammatory cell infiltrates without evidence of vasculitis [9, 35].
These patients were young (range 22-47 years) and free of vascular risk factors, although 48% of them were intravenous drug users. Features of this microvasculopathy are similar to those observed in the brains of non-HIV aging patients with high blood pressure or diabetes mellitus [35]. Cranial nerve mononeuritis (left trochlear nerve palsy) and HIV-1 microangiopathy have been described [64]. Calcification of the vessel wall and calcium deposits occurred less often in adults than in children [31].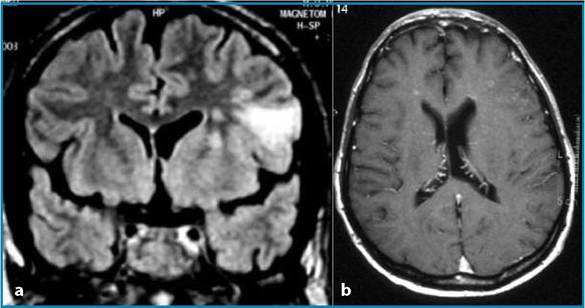
Fig. 3a, b Immune reconstitution vasculitis confirmed by brain biopsy. a Fluid-attenuated inversion recovery MR image obtained in the coronal plane shows an infarct in the left middle cerebral artery territory. b Gadolinium- enhanced T1-weighted MR image obtained in the axial plane shows punctiform bilateral enhancement
The alteration of the cerebral microvascularization in HIV-1-infected patients induces disturbed vasoreactivity, as demonstrated by reduced baseline cerebral flow and decreased cerebrovascular reserve capacity in response to acetazolamide challenge [65]. Abnormalities of cerebral perfusion have also been documented in the early stages of the infection and in asymptomatic HIV-1-infected patients [66]. Transcranial Doppler imaging has been used to monitor the progression of a reversible form of symptomatic cerebral vasospasm observed in two HIV-1-infected patients with presumed underlying HIV-related vasculopathy [49]. Vasoreactivity was confined to small cerebral arterioles, the same vessels showing pathologic changes in the autopsy series of Connor et al. [35]. These disturbances may represent a predisposing factor for the development of cerebral microinfarcts. Frequent in children, stroke caused by intracranial large-vessel aneurysmal HIV-associated vasculopathy has exceptionally been reported in adults [67].
Atherosclerosis and Antiretroviral Therapies
Increasingly, severe treatment-associated metabolic side effects have been observed with combined antiretroviral therapy, among them dyslipidemia, insulin resistance, and overt diabetes mellitus, which are well-known risk factors for cardiovascular disease.
Endothelial dysfunction, impaired fibrinolysis, and excess inflammation may also contribute to the increased cardiovascular risk in HIV-infected individuals. Surrogate markers such as C-reactive protein (CRP), homocysteine, tissue plasminogen activator, and plasminogen activator inhibitor-1 are higher in HIV-positive than in HIV-negative subjects, are increased in patients treated with HAART in association with metabolic abnormalities and altered fat distribution [10]. The pathogenesis of atherosclerosis now includes chronic systemic inflammatory activity, and CRP is a predictor of cardiovascular mortality in HIV-infected women [68]. The results of the DAD study support the hypothesis that early atherosclerosis is a side effect of combined antiretroviral therapies [20]. The mechanism for PI-induced dyslipidemia is not yet established; direct effect of drugs themselves, interactions between antiretroviral treatment, HIV, host response to infection or genetic predisposition are hypothesized [10, 11]. The full clinical implications of vascular imaging findings are still being debated. In a recent review [69], 88% of studies measuring carotid intima thickness or atherosclerotic lesions reported worsening of these conditions in association with PIs. Several groups have examined the relationship between antiretroviral therapy, HIV, and carotid intima-media thickness in cross-sectional and longitudinal studies, with conflicting results. Some cross-sectional studies have concluded a positive correlation between PIs exposure and carotid intima-media thickness [70-72], using both presence of plaque and carotid intimamedia thickness as an endpoint, while others have found that, after control for traditional cardiovascular risk factors, PIs were no longer a statistically significant predictor of plaque or carotid intima-media thickness [73, 74]. Jerico et al. [75] identified the use of combination antiretroviral therapy as a predictor of subclinical atherosclerosis independent of the Framingham risk score. Longitudinal studies of changes in carotid intima-media thickness have also produced conflicting issues. Hsue et al [76] reported rapid progression of carotid intima-media thickness. Median carotid intima-media thickness increased in the first 12 months and then decreased by month 36 for Thiebaut et al. [77]. Carotid intimamedia thickness increases with age, body mass index, waist circumference, and tended to be lower in female and in subjects with higher HDL cholesterol [78]. Currier et al. [78] showed that traditional risk factors for cerebrovascular diseases can overshadow the impact of PI exposure in the development of carotid intima-media thickness. In this study, the use of PIs was not correlated with an increase of intima-media thickness [78]. The relative increase in cardiovascular disease is still small in an absolute sense, and the overwhelming effect of antiretroviral therapies is positive in terms of improvement in immune function and related morbi-mortality [10]. Yet carotid intima-media thickness appears to be a strong predictor of incident stroke, and arterial intima-media thickness per se is an important determinant of vascular disease in young HIV-negative individuals [79]. As HIV-positive individuals live longer on treatment, this risk must be evaluated, because the effectiveness of medical therapy such as antiplatelet agents or anticoagulants in the setting of HIV-associated vasculopathy is unknown. Moreover, in the light of findings suggesting that atherosclerosis, predominantly carotid atherosclerosis, is associated with an increased risk for dementia [80], an evaluation of cardiovascular risk should be offered periodically to HIV-infected subjects, especially after HAART initiation [11].Hematological Disorders
Elevated levels of antiphospholipid IgG antibodies have been reported to occur in up to half of patients with HIV-1 infection and AIDS, and correlate highly with the presence of perfusion defects on SPECT scanning [81]. The clinical relevance of this remains uncertain. Indeed, the role of these antibodies in the pathogenesis of stroke in HIV-1/AIDS patients is not clearly understood [13], and their importance as a cardiovascular risk factor is controversial [82].
A frequent prothrombotic state in HIV-1- infected patients is protein S deficiency [40, 43, 52], also involved in ischemic stroke in noninfected individuals. However, its role in predisposing HIV-1-infected patients to cerebral infarction is not well established [40, 83]. A single retrospective case-control study showed a significant association of protein S deficiency in HIV-1-positive stroke patients compared with HIV-negative stroke patients [40].Yet, protein S deficiency seems to be statistically related to the HIV infection rather than the stroke occurrence [84]. A high prevalence of IgG anticardiolipin antibodies and protein S deficiency was also reported in TND [43]. Disseminated intravascular coagulation [28, 29, 33] and hyperviscosity related to polyclonal hypergammaglobulinemia [85] have also been documented in rare cases.
Drugs
Associations have been reported between over-the-counter prescription and illicit drugs with sympathomimetic properties and cerebral infarction [86, 87]. Except for a few instances of vasculitis and pharmacologically induced focal vaso-spasm, the etiology of drug-related cerebrovascular accidents is often unclear. Ortiz et al. [14] found an association between recent cocaine use and non- atherothrombotic strokes. Other mechanisms are arrhythmias and foreign embolism from impurities. However, these mechanisms are not specific to HIV infection.
Unknown Mechanism
As in noninfected young individuals, the proportion of ischemic stroke whose causes remain unidentified despite complete investigations is high and varies from 24 to 40% in HIV-1-infected patients [9, 14, 27, 41, 88]. However, a thorough exploration has not always been performed in published series. In light of the increased frequency of atypical stroke mechanisms in HIV-infected patients, comprehensive diagnostic evaluations are justified [14].