Intracerebral, Subarachnoid Hemorrhages and Subdural Hematoma
Intracerebral hemorrhages are less frequent than ischemic strokes in the majority of published series, but an equivalent ratio has also been reported [16]. Mainly localized in the subtentorial regions, their localizations are various, sometimes multiple.
They could be asymptomatic if of small size [31], but mortality tends to be high. The most frequent causes (Table 2) are opportunistic diseases (notably toxoplasmosis, tuberculosis, cytomegalovirus, HSV-1), mycotic aneurysms (Fig. 4), lymphoma, thrombocythemia, and metastatic Kaposi’s sarcoma [9, 13, 23, 33, 67, 89]. Risk factors like alcoholism, drug abuse (especially cocaine and crack, amphetamine, phenylpropanolamine, phencyclidine), high blood pressure, or hemophilia are sometimes found [9, 32, 41, 47, 90]. Cocaine-associated intracranial hemorrhages seem to be a consequence of the pharmacodynamic effect of cocaine and not of a cocaine-induced vasculopathy [91, 92]. Other occasional causes include disseminated intravascular coagulation, ruptured mycotic aneurysms, or disruption of congenital aneurysm [8, 9, 28, 29]. Subarachnoid hemorrhage and subdural hematoma in clinical [47] and autopsy series [13, 31] are more anecdotal. A subdural hematoma was reported in an HIV-1- infected patient with an HIV-associated encephalopathy and cerebral atrophy [93]. Recently, an increased risk of intracerebralTable 2 Causes of intracerebral hemorrhage
Thrombocythemia
Autoimmune
Drug-induced
Disseminated intravascular coagulation
Hemophilia
Aneurysmal dilatation
Mycotic aneurysm
Vasculitis
Opportunistic infections
Drug-induced
Neoplasms
Aspergillosis
Metastatic Kaposi’s sarcoma
Alcoholism
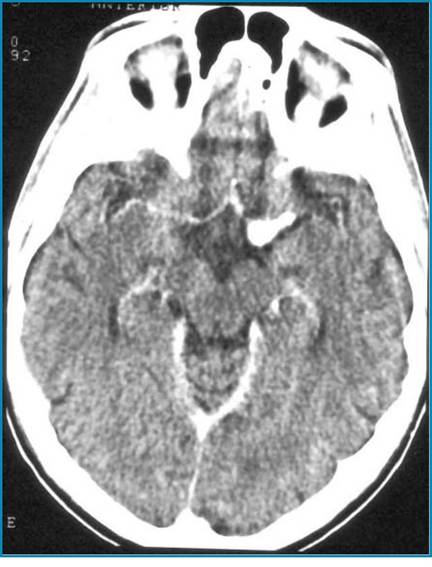
Fig. 4 Contrast-enhanced CT scan shows a mycotic aneurysm of the left middle cerebral artery
hemorrhages has been observed with tipranavir co-administrated with ritonavir. Tipranavir induces changes in coagulation parameters in rodents and may inhibit human platelet aggregation.