Management of IDU-related problems
Controlled Drug prescriptions
A working knowledge of the regulations surrounding Controlled Drug prescriptions is important when managing drug users. Attention to detail when a patient is admitted is imperative if centres are to avoid the problems of double prescribing.
The front pages of the BNF give exact guidelines on how to prescribe Controlled Drugs legally and additional information is available via the updated Guidelines on Clinical Management, Drug Misuse and Dependence published by HMSO in 1999.The medical effects of recreational drugs
Carers need to have a working knowledge of the effects of recreational drugs and equivalent doses of drugs (methadone or diazepam) if patients need to be temporarily covered for the effects of withdrawal. Tables of equivalence for opiates and benzodiazepines can be found in Guidelines on Clinical Management, Drug Misuse and Dependence (HMSO 1999). The differential diagnosis in a patient with IDU-related HIV is extensive and requires consideration of both infective and non- infective disorders. These are summarised in Table 11.1.
When patients are admitted with respiratory problems there is the dilemma of how to manage opiate prescribing.
• For those patients with mild respiratory depression a discussion over a temporary reduction in oral drugs by around 10—20% or splitting the daily dose into 3 or 4 doses may suffice.
• In those with more severe respiratory depression rapid improvement in pulmonary function is required. However if the opiate withdrawal is excessive as with intravenous bolus injections of naloxone, the patient may become disruptive with loss of venous access.
• The preferred solution is a naloxone infusion (2 mg in
500 ml perhaps starting at around l0ml per hour) to achieve an acceptable improvement in respiratory rate (and therefore oxygenation) without too great an increase in physical arousal.
The aim is to improve oxygenation rather than induce withdrawal from opiates. This improved oxygenation can be assessed by respiratory rate, oxygen desaturation or arterial blood gases. Such an infusion may be required for up to 48 hours in those on methadone because of its relatively long half-life compared to other opiates. In the event of a lack of venous access then regular small doses of intramuscular nalaoxone (0.2 mg i.m. every 1 hour initially) can also be employed to maintain oxygenation.Excessive doses of benzodiazepines also produce drowsiness and/or coma which can usually be managed by simple supportive therapy with care over respiratory rate, etc. In extreme cases it is possible to utilise the antagonist flumazenil but there is a danger of inducing fits in those on chronic longterm doses. It is therefore preferable to reverse the opiate element first (with an infusion of naloxone) before resorting to flumazenil.
Opiate withdrawals should be considered in any agitated patient known to be on opiates, particularly those who have recently commenced drugs that induce liver enzymes such as rifampicin, rifabutin, phenytoin, etc.
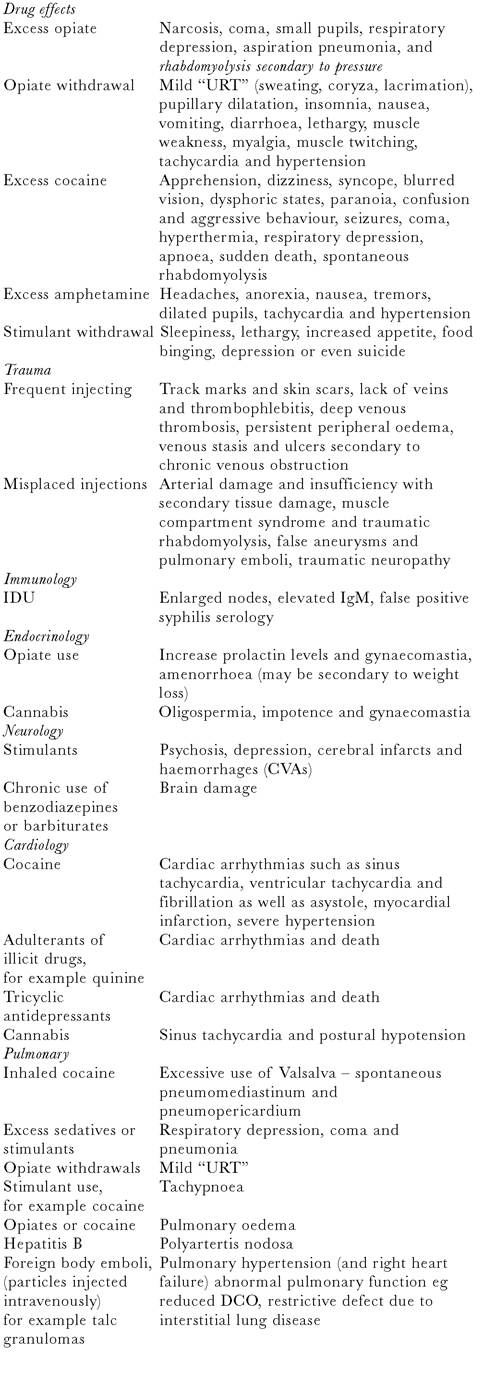
Table 11.1 Medical (non-infection) problems of drug use
Problem
Medical complications