Medical problems of HIV-infected drug users
The extent of IDU-related conditions requires consideration of not only the clinical features of IDU but also the associated medical conditions such as HIV since confusion may arise as to the aetiology of specific symptoms.
(See Box 11.9)Pre-AIDS deaths
The phenomenon of pre-AIDS death amongst HIV-infected drug users was described soon after the onset of the AIDS epidemic in the USA. The IDU non-AIDS death rate was 2.5/100 person-years in Edinburgh (compared to 0.9/100 person-years in other risk groups), 3.8/100 person-years in Amsterdam and 2.6/100 person-years in New York. In Edinburgh 20% of pre-AIDS deaths were expected and related to conditions not ostensibly related to HIV. Liver disease was the single commonest cause of these deaths, accounting for 75% of expected pre-AIDS deaths or 25% of all pre-AIDS deaths, and is presumably related to the heavy co-infection with hepatitis B and C.
Respiratory infections
A review of pneumonia in all HIV positive patients suggested an increased annual incidence of bacterial pneumonia; 97—290 per 1000 compared to 21 per 1000 for HIV negative individuals. IDU-related HIV patients also have an overall higher incidence of bacterial infections; 12% (mortality of 2.2%) compared to 3% (mortality of 0%) in HIV negative drug users. The overall rate of bacterial sepsis in Edinburgh drug users was 7.0 per 100 person-years whilst in the Bronx cohort of drug users the rate was 8.0 per 100 person-years. In Spain 60% of the pneumonias in the HIV-infected patients occurred before a diagnosis of AIDS, in 55% of patients the problem was recurrent and the mortality was increased for HIV-infected patients (19% vs. 4%). Streptococcus pneumonia and Haemophilus influenzae were the commonest organisms involved in the pneumonias. Additional susceptibility factors for drug users may be the use of opiates themselves because they are known to depress the cough reflex as well as the immune system.
Latterly it has been suggested that the inhalation of drugs as well as the injection of drugs may increase the risks of bacterial pneumonias. The odds of developing pneumonia were twice as great for those reporting smoking cocaine, crack cocaine and marihuana and over 20-fold increased for those also having prior PCP and a low CD4. The effects of tobacco were not examined since all patients utilised this drug. The incidence of tuberculosis is much higher in HIV-infected drug users than in other risk groups outside the tropics, or in HIV negative drug users. In the USA, most patients with AIDS and tuberculosis have been drug users. One study showed a prevalence of 15% in drug users with AIDS but only 4% in other risk groups within a New York hospital. In New York the rate of tuberculosis was 4% among HIV positive drug users compared to 0% in HIV negative drug users. The 36% increase in reported cases of tuberculosis between 1984 and 1986 has been largely ascribed to infection amongst HIV positive drug users.Hepatitis
Drug users with a history of IDU are highly likely to be coinfected with hepatitis B and C viruses (anywhere from 40% to 100% depending on location).
Anti-HIV drugs have long been associated with hepatitis and it is uncertain at present whether modern combination therapy for HIV will have a deleterious effect on those
Table 11.1 continued
Box 11.9 Associated medical problems of IDU
• Lymphadenopathy is associated with both HIV and the injection of foreign materials.
• Fatigue, lethargy and excessive sweating are features of HIV as well as mild withdrawal from opiates.
• Diarrhoea, a common presentation of early symptomatic HIV (CDC stage IVA), is also a common symptom of opiate withdrawal.
• Weight loss and fever are both key symptoms of the constitutional symptoms associated with HIV (CDC stage IVA), infection with mycobacteria as well as heavy opiate or stimulant (amphetamines or cocaine) use.
• Epileptic seizures require consideration of cerebral toxoplasmosis in HIV, the intermittent use of benzodiazepines or even hepatic encephalopathy.
• The excessive use of cannabis and benzodiazepines interferes with memory and other cognitive functions in a similar manner to HIV as does frequent head injuries. Thus early dementia is difficult to detect in current drug users especially since reducing drugs will also help the dementing patient to improve function in relation to activities of daily living.
• Syncopal attacks in HIV may be associated with an autonomic neuropathy or a failing adrenal cortex but it is also associated with the use of antidepressant tricyclic drugs such as amitriptylene.
• Jaundice may be a result of acute or chronic hepatitis B or C infection, excessive alcohol ingestion or a side effect of the treatment of mycobacterial infections in HIV.
• Lastly shortness of breath and a persistent cough are common early symptoms of Pneumocystis carinii pneumonia (PCP) but can occur with endocarditis, bacterial pneumonia, excessive smoking, recurrent bronchitis and obstructive airways disease.
Greater detail can be obtained from the web site of the Regional Infectious Diseases Unit, Western Infirmary, Edinburgh (www.med.ed.ac.uk/ridu/History.htm).
Box 11.10 Co-infection of HIV and hepatitis viruses Hepatitis B
• 10% of drug users will be carriers of hepatitis B
• Re-emergence of carriers (HbsAg) with CD4 counts of < 200 cells/pl may occur
Hepatitis C — data contradictory and may vary with risk groups because of length of HCV infection which is often unknown
• HCV RNA levels rise with falling CD4 counts
• Increased progression of both HIV and HCV disease reported in haemophiliacs
• Studies on drug users have reported no change of HIV progression
• Increased rate of HCV progression also reported in drug users
co-infected with HCV or not. There are reports in the literature of therapy improving, worsening or having no effect on concomitant HCV.
Thus despite a greater risk of hepatotoxicity in HIV/HCV co-infected patients on highly activated retroviral therapy (HAART), this is not a reason to withold therapy from HCV HIV co-infected patients but rather such patients require more carefully monitoring. There is also the problem of additional hepatotoxicity associated with the use of antituberculous drugs in HIV/HCV co-infected individuals.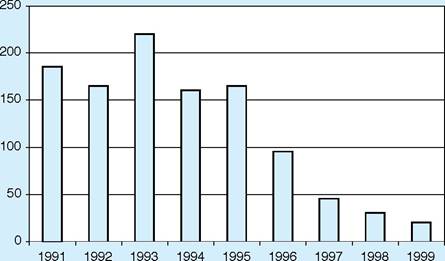
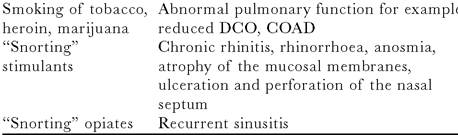
Figure 11.1 Opportunistic events/100 patient-years: Regional Infectious Diseases Unit, Edinburgh
Although treatment for HCV is now available in the form of interferon and ribavirin, tolerance and interactions with HIV therapy are likely to be problematical since ribavirin has been reported to interfere with the phosphorylation of nucleosides such as zidovudine.
HIV dementia and encephalitis
HIV/AIDS is unusual in that it combines both immunological, neurological and psychiatric disorders and as a consequence patients may develop a variety of disabilites ranging from wasting disorders, severe pain, neurological dysfunction such as paralysis or cognitive impairment and psychological symptoms. These combinations of problems may result in considerable problems for both patients and carers. Autopsy studies in Edinburgh (prior to modern antiretroviral therapy (ART)) have shown that as many as 60% of IDU-related HIV patients have evidence of HIV encephalitis although only 6—7% have frank dementia.
AIDS
As for AIDS itself, little variation between the risk activities with regard to presentation has been reported. In the USA, figures available to the Centers for Disease Control show that conditions such as Kaposi's sarcoma are unusual in the absence of homo/bisexuality. In drug users, Kaposi's sarcoma, cytomegalovirus and chronic cryptosporidiosis are all significantly less common than for all other risk groups notified with AIDS, while PCP, tuberculosis, oesophageal candidiasis and extrapulmonary cryptococcosis are more common.
Progression from HIV to AIDS
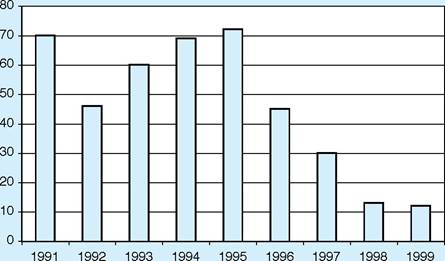
Figure 11.2 Deaths/100 patient-years: Regional Infectious Diseases Unit, Edinburgh
No evidence has been found for a role of alcohol, opiates or other psychoactive drugs in accelerating the progression of immunodeficiency in HIV-seropositive homosexual and bisexual men. The major factors identified in the progression of HIV appear to be age and HLA type. Al B8 Dr3 and Bw 35 are all associated with more rapid progression whilst B27 is associated with slower progression to AIDS and death.
Survival after the development of AIDS
Without treatment, in general, around half of patients with AIDS survive for one year but only a fifth for three years and the median survival time is around 18—20 months. In Edinburgh the one- and three-year post-AIDS survival rates were 66% and 25%. Older age at AIDS diagnosis and HLA type A1 B8 DR3 were associated with shorter survival. Whilst it had been generally assumed that the survival for injection drug users with AIDS would be shorter than for other risk groups, several studies including our own counter this presumption.
Problems of pain management in IDU-related HIV The investigation of pain in IDU-related HIV is a major problem for carers, particularly since it is a useful complaint to increase the size of opiate prescriptions. Considerable experience is required in both the investigation and management of pain in order to avoid ever larger prescriptions.
The commonest problem in the management of pain in drug users is that of insufficient doses as a consequence of existing high levels of opiate use and/or disagreement from carer s over whether pain is real or being treated adequately. Self-medication is a common problem which increases the uncertainties around prescribing. The use of inappropriate drugs such as Diconal or Temgesic should be avoided because these drugs are highly sought after as recreational drugs in the community.
Our own practice has been to utilise increasing doses of existing drugs such as methadone, oral solutions of morphine, slow-release morphine preperations such as MST (although this also has some street value since it can be injected), morphine/diamorphine solutions via subcutaneous infusions or fentanyl patches.
There is the additional problem of providing adequate sedation during procedures. Patients may require unusually large doses of medazolam as a consequence of their regular intake of benzodiazepines. If adequate doses of medazolam are not used then there is no loss of memory for the procedure which can be quite distressing for the patients. Alternatively, particularly if the patient uses illicit benzodiazepines or opiates, excessive sedation occurs with even quite small doses. As with the elderly, some HIV/AIDS patients also exhibit an unusual sensitivity to neuroleptics such as carbamazepine or antidepressants, possibly because of the concomitant presence of HIV encephalopathy. Care is therefore required in the introduction of such drugs for pain control.
Box 11.11 Common causes of pain in drug users
Dental caries
Traumatic neuropathies
Abdominal pain
• Constipation
• Cholecystitis
• Appendicitis
• Chronic hepatitis
• Lymph node enlargement
MAI
Lymphoma
Box 11.12 Problems of antiretroviral therapy in drug users
• Regular venous access required — consider external jugular rather than femoral artery
• Improved health may encourage a return to IDU — continue with harm reduction strategy
Antiretroviral therapy
It is perfectly possible to treat drug users with antiretroviral therapy although there are a number of simple difficulties such as venous access for monitoring of therapy.
When considering combination therapy for recreational drug users a number of important principles need to be understood by the drug users. Whilst these may seem obvious to ourselves this is not the case for the patients.
A number of groups have been exploring drug regimens thought to be particularly suitable for drug users, usually because they provide the possibility of a once-daily regimen, and therefore the option of employing directly observed combination therapy (DOCT) at a suitable location. Whilst DOCT may be offered to a patient as an option it should perhaps be seen as a means to an end rather than as a longterm solution.
Drug interactions
Drug interactions are an ever present problem with modern antiretroviral therapy for all patients, but even more so for those taking recreational drugs where there is the ever-present possibility of serious increases in the levels of pharmaceutical or recreational drugs. Of course from the patient's point of view reduced levels of recreational drugs is also an important problem.
Box 11.13 Important principles in modern antiviral combination therapy
• Intermittent combination therapy is a major disadvantage because of the development of resistance which will impair future therapy choices
• Almost total (95%) adherence is required for the best chance of long-lasting success (undetectable viral load)
• Increasing the number of drugs used in combination therapy does not increase “wellness”, it simply increases the chance the regimen will be successful for a longer period
• However more antiviral drugs increase the chance of an adverse drug related event
• Intermittent recreational drug use is more dangerous and difficult to adjust for than regular recreational drug use (time and patience required by both patient and doctor) in terms of interactions with combination therapy
The most extensively investigated interactions are with methadone since it is commonly used long-term for heroin substitution. Little other investigational work has been undertaken possibly because of the difficulties of working with illegal drugs such as cocaine or amphetamine and some lack of interest on the part of pharmaceutical companies. One proviso when discussing interactions is our relative lack of knowledge of methadone levels and symptoms of withdrawal. Very little work seems to have been carried out in this area recently and much more is required if we are to better understand the interactions that do occur.
Other drugs used in HIV
It is important also to remember that a number of other drugs commonly used in HIV medicine such as rifampicin or phenytoin also dramatically reduce methadone levels by enzyme induction and cause problems with acute withdrawal. Increased zidovudine levels have also been reported with sodium valproate, a drug that is commonly used to control seizures.
In summary the use of recreational drugs certainly affects the choice of anti-viral drugs and possibly also the time at which therapy starts. Individual regimes to suit particular problems are important. Because of the complexity of the interactions it is important to get over to the patient how vital it is to know what drugs are actually taken rather than what drugs are prescribed. Misinformation may be fatal and they need to understand why the information needs to be accurate. This will only work of course if the patient is truly persuaded of the need for therapy. The risks of not taking therapy have to be very real and to outweigh the risks of the therapy — which after all in the case of ecstasy and ritonavir could be sudden death — not a very good outcome measure for combination therapy. For drug users the risks of disease may not outweigh therapy until the CD4 count is below 200 cells/microgram when the immediate risk of ill health is 20% or one in five for the next 12 months and 80% or four in five for the next three years. By comparison, the risk of a drug-related adverse event lies somewhere between 3% and 30%. At levels of CD4 count of 350 or 500 the risks of an adverse event are likely to outweigh the risk of serious HIV disease.
Despite all these difficulties, in Edinburgh with around 50% of our patients being drug users, we have managed to achieve the same reductions in opportunistic infections and deaths noted in other areas.
Thus recreational drug use related HIV can be managed successfully via attention to drug dependence needs, social needs and the medical care needs.
Box 11.14 Substitute recreational drug therapy and interactions with HAART
NRTI (Nucleoside Reverse Transcriptase Inhibitors)
• Zidovudine
• ZDV levels increased by opiates (AUC increased x 2)
• Stavudine and Didanosine
• Absorption decreased by co-administration with methadone
• Abacavir
• Rate but not extent of absorption of decreased by coadministration with methadone
• Increased clearance of methadone — dose adjustment may be needed
NNRTI (Non Nucleoside Reverse Transcriptase Inhibitors)
• Nevirapine and efavirenz
• AUC of methadone reduced by as much as 30% — dose adjustment may be needed
• Delavirdine
• AUC of methadone increased — to date no reports of dosage adjustment required
PI (Protease Inhibitors)
• Ritonavir
• No change in methadone dosage required
• Heroin and morphine levels reduced
• Dextropropoxyphene and pethidine levels increased
• Indinavir
• Initially need to reduce methadone doses but after a few weeks return to previous levels
• Nelfinavir
• Methadone levels reduced and dosage adjustment usually necessary
Figure 11.3 Survival of AIDS 1983-99: Regional Infectious Disease Unit, Edinburgh
12