Pathological Coronary Lesions
1. Common atherosclerotic plaques were present on the three main coronary trunks in 60% of cases, with two different patterns: either young plaques consisting in macrophages, foamy cells, and a small amount of extracellular lipid deposit (Fig.
1), or adult eccentric plaque with a lipid core surrounded by a fibrous wall consisting in macrophages, fibroblasts, smooth muscle cells, a few lymphocytes, elastic fibers, and collagenous fibers. Stenosis occluded 75% or more of the lumen (Figs. 2-4). In one case, the right coronary artery was completely occluded by a massive thrombosis (Fig. 5).2. Uncommon intimal thickening which was diffuse, circular, and concentric throughout the whole length of every coronary trunk affected all patients, occluding over 40% of the vascular lumen. Collagenous and microelastic fibers were admixed with smooth muscle cells, macrophages, rare foam cells, and fibroblasts, without lymphocytes (Figs. 6-9).
3. Unusual and original lesions consisting in proliferation of smooth muscle cells mixed with numerous packed elastic fibers, which formed mamillated
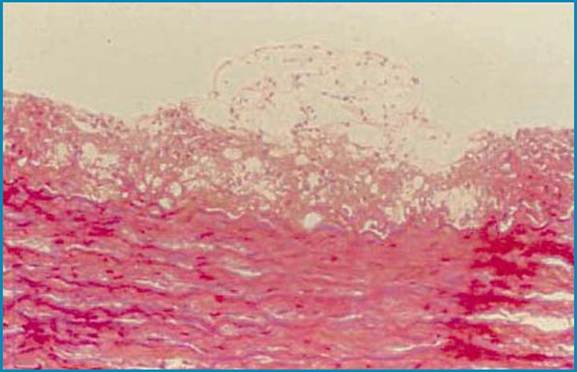
Fig. 1 Common atherosclerotic young plaque. Col HPS ?100
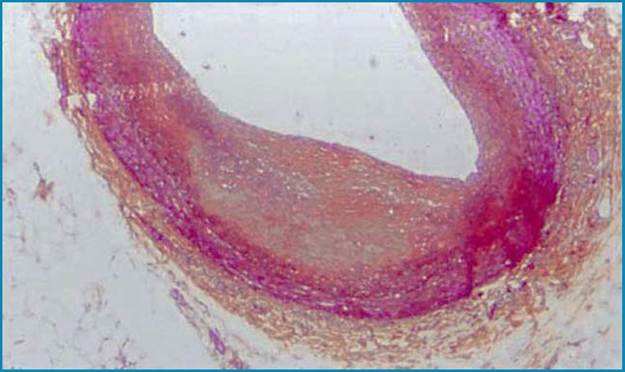
Fig. 2 Adult eccentric plaque.
Col HPS, ?25
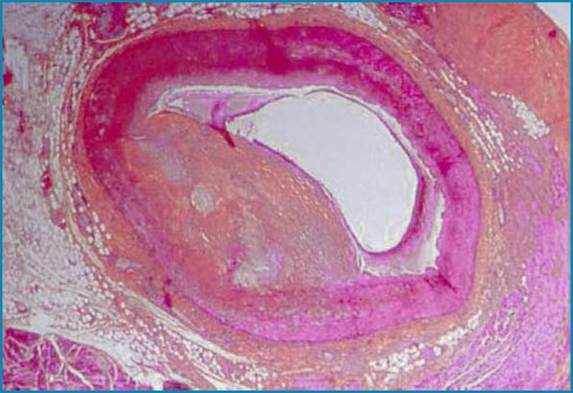
Fig. 3 Adult eccentric plaque. Col HPS, ?25
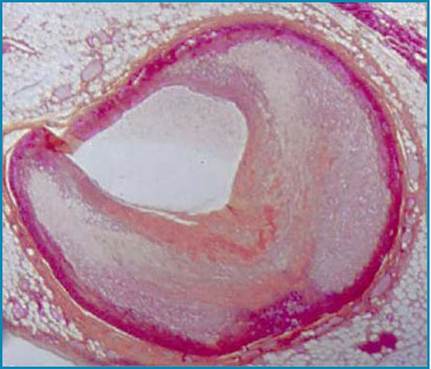
Fig. 4 Adult eccentric plaque. Col HPS, ?25
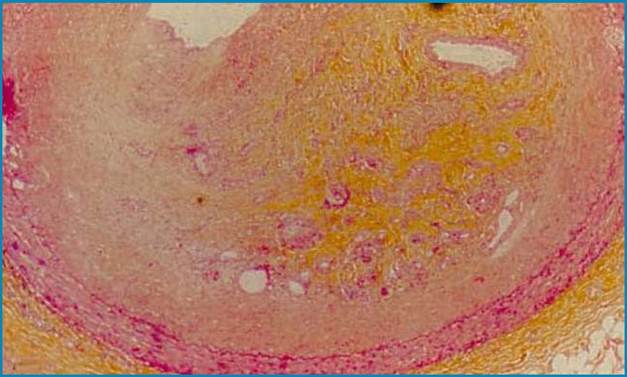
Fig. 5 Complete occlusion by fibrous organized plaque. Col HPS, ?25

Fig.6 Intimal diffuse and circular thickness
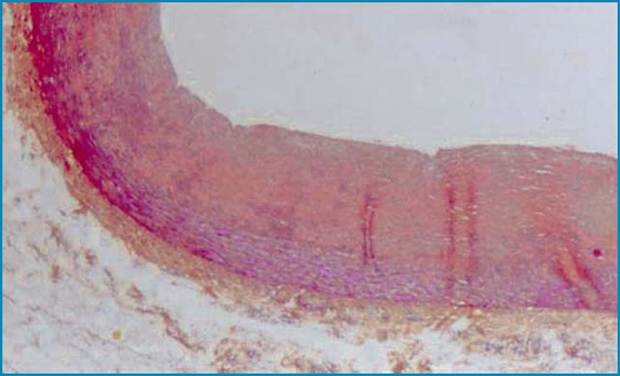
Fig.7 Intimal diffuse and circular thickness.
Col HPS, ?25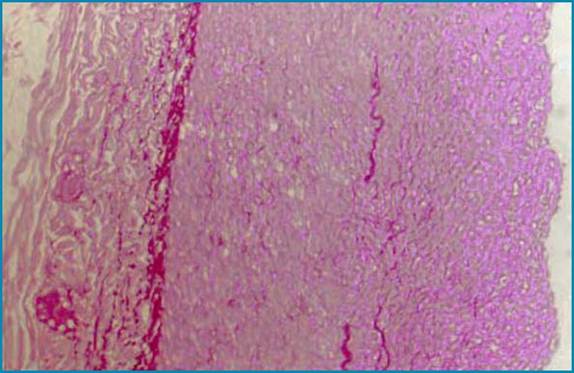
Fig. 8 Intimal diffuse and circular thickness. Col HPS, ?100
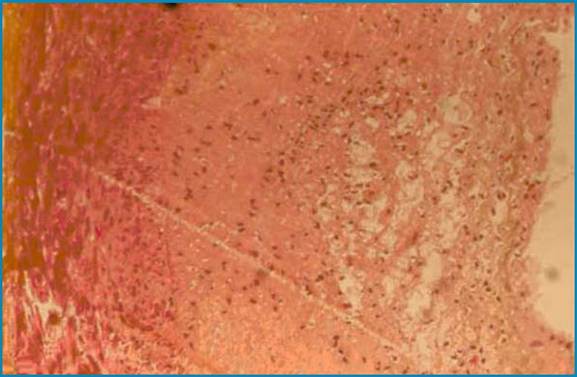
Fig. 9 Intimal diffuse and circular thickness with foamy cells. Col HPS, ?100
endoluminal protrusions resembling vegetations, were present in 40% of cases (Figs. 10-12).
The distal coronary network of intramural arterioles was also the site of a diffuse concentric intimal wall thickening occluding more than 80% of the lumen in 25% of cases (Figs. 13-15). Immunohistochemical data allowed true identification of smooth muscle cells (alpha-actin and vimentin expression) as the main elements of diffuse intimal layer thickening. The expression of tumor necrosis factor-alpha (TNF-α) and interleukin-1-alpha (IL-1α) in these cells was significantly greater than in smooth muscle cells of the underlying media. Fibro- cytes and fibroblasts were scarcely disseminated on the periphery of atherosclerotic plaques, mixed with smooth muscle cells and some lymphocytes. CD68 expression identified macrophages, proving also TNF-α and IL-1 expression and Factor VIII expression appeared on endothelial cells. Coronary lesions in AIDS patients have some of the characteristics of common atherosclerosis such as eccentric fibro-lipidic plaques; however, they also present similarities with coronary lesions following heart transplantation (so-called chronic rejection) such as diffuse concentric intimal thickening occurring in coronary trucks and in the distal network [12].
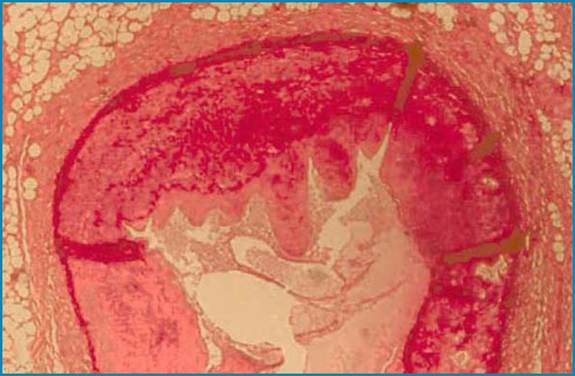
Fig. 10 Mamillated endoluminal protrusion. Col HPS, ?25
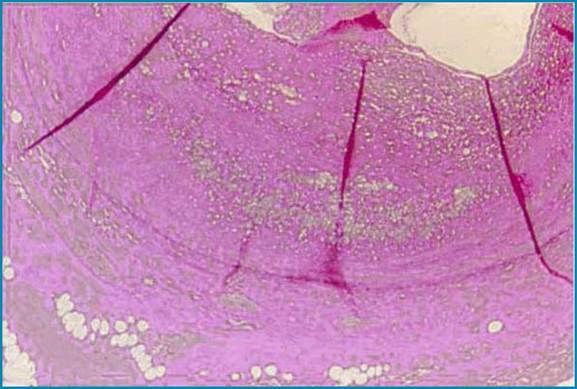
Fig. 11 Mamillated endoluminal protrusion. Col HPS, ?100
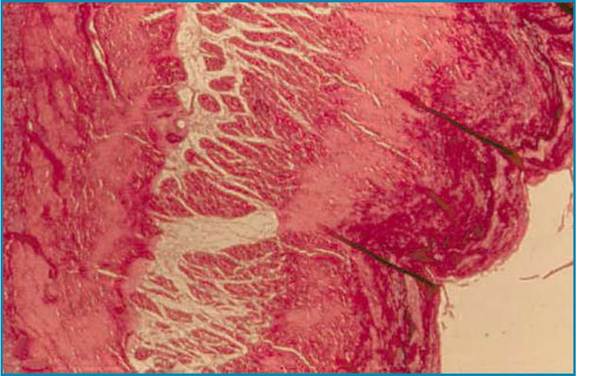
Fig.12 Mamillated endoluminal protrusion. Col Weigert, ?25
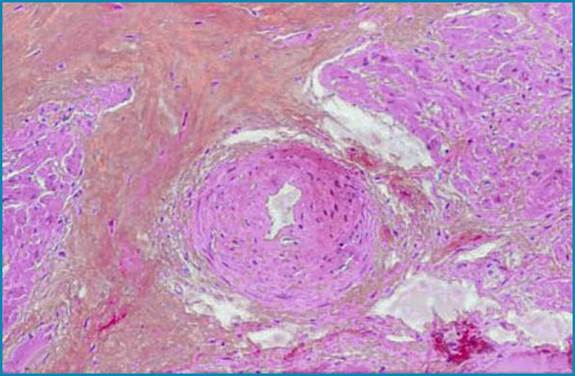
Fig. 13 Distal coronary network. Col HPS, ?25
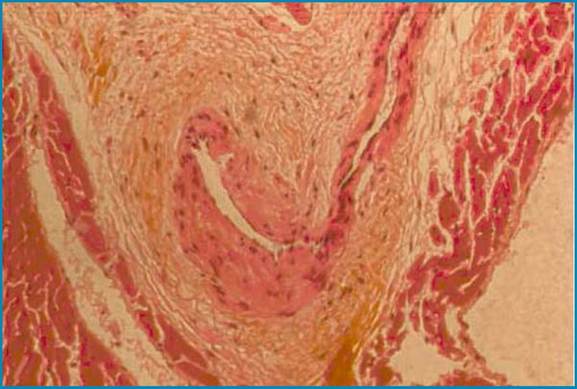
Fig. 14 Distal coronary network. Col HPS, ?100
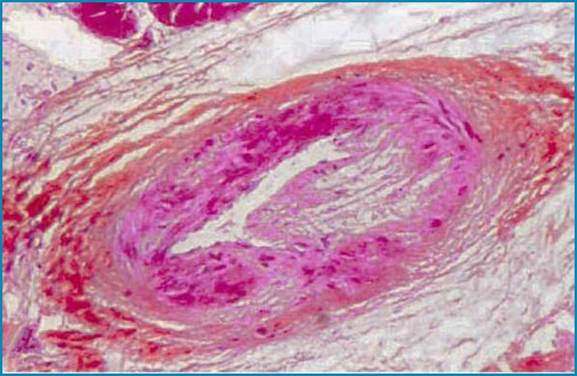
Fig. 15 Distal coronary network. Col HPS, ?100