Pericardial Effusion and Tamponade
Before the introduction of HAART, the prevalence of pericardial effusion in asymptomatic AIDS patients was estimated at 11% [9], and was particularly high in those with end-stage disease.
HAART has significantly reduced the overall incidence of pericardial effusion in HIV patients. Pericardial effusion in HIV disease may be related to opportunistic infections (tuberculosis and nontuberculosis mycobacteria [10], Nocardia [11], Cryptococcus [12], and cytomegalovirus), malignancy (Kaposi’s sarcoma [13], non-Hodgkin’s lymphoma [14]), and valve endocarditis or bacterial pericarditis [15] (Streptococcus pneumoniae), but most often a clear etiology is not found. Hypoalbuminemia, which is associated with ascites and pleural effusions, is a potential cause of pericardial effusion in end-stage HIV infection. Pericardial effusion may be part of capillary leak syndrome. A pericardial effusion is a marker of shortened survival.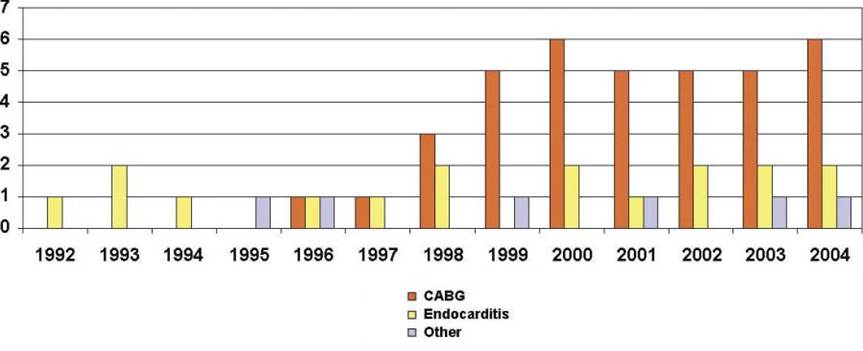
Fig. 1 Evolution of cardiac surgery in La Pitie Institute, Paris. CABG, coronary artery bypass grafting
The majority of pericardial effusions are small and asymptomatic, but sometimes there is a cardiac tamponade which requires urgent pericardial drainage (only 1 case among 231 patients over a 5-year period for Heidenreich) [9]. An HIV test is required for each patient with pericardial effusion. In young patients with cardiac tamponade, the coexistence of fever and pulmonary infiltrates is suggestive of underlying HIV infection [16]. The indications of pericardiocentesis or pericardial window are not different between HIV-infected and other patients in cases of cardiac tamponade. Because the effusions are frequently small and rarely progressive, an exhaustive search for a diagnosis with pericardiocentesis is not indicated. The surgical techniques are the same as those used on non-HIV patients, with a preference for percutaneous or videoscopic techniques limiting the risk of viral transmission to the surgical team.