Valvular Surgery
Valvular surgery is the most common cardiac surgery performed on HIV patients, particularly in the pre-HAART era when severe infectious endocarditis was frequent in patients with significant immunodeficiency.
In these patients, two factors which increase the incidence of infective endocarditis are frequently associated: intravenous drug abuse and immunodeficiency [17—19]; this association was found in 85% of 40 patients reported by Aris et al. in 1993 [20] and in all 11 patients for Frater et al. in 1989 [1]. The indications for cardiac surgery (replacement or valve repair) are classic (heart failure, valve destruction, emboli, annular abscess) with a higher number of interventions for persistent infection despite proper antibiotic treatment. In cases of tricuspid endocarditis, the indication for cardiac surgery is rare except for infections with yeasts.The prevalence of infective endocarditis in HIV-infected patients is similar to that of patients in other risk groups such as intravenous drug users. Estimates of endocarditis prevalence vary from 6.3 to 34% in HIV- infected patients who use intravenous drugs independently of HAART regimens. Rightsided valves are predominantly affected and the most frequent agents are Staphylococcus aureus, Streptococcus pneumoniae, Haemophilus influenzae, Candida albicans, Aspergillus fumigatus, and Cryptococcus neoformans [21, 22]. Infective organisms are common; nevertheless, yeasts (Candida albicans) and rare bacteria such as corynebacte- ria should be suspected particularly in rightsided endocarditis in intravenous drug abusers.
Good results have been achieved with the use of mechanical heart valves, bioprosthetic valves, and homografts (Fig. 2) in patients who have endocarditis [23]. Most surgeons use the following standards for heart-valve replacement: (1) a mechanical heart valve in adults, young patients, and pediatric patients when there is no contraindication to long-term anticoagulation; (2) a bioprosthet- ic valve in most patients over 65 or 70 years, patients with a proven short life expectancy, those requiring right-heart valve replacement, those in whom anticoagulation poses a high risk, and those with contraindication to long-term anticoagulation.
Because survival is longer in HIV-controlled infection, at La Pitie, similar to Abad et al. [4], the same policies are applied to all patients who are HIV-
Fig. 2 Aortic homograft
positive, whether they are drug addicts or not. Using a homograft in an aortic position is supported when the lesions are very destructive with a large annular abscess [4]. In summary, the policy for choosing a valve substitute is identical in HIV-positive and HIV-negative patients (Figs. 2-4).
Valvular endocarditis is still the most common finding in HIV-positive patients (Figs. 3, 4). However, it is possible that in the future, with the aging of this population due to longer survival as a result of HAART, valvular surgery will be performed for noninfec- tive lesions like aortic stenosis.
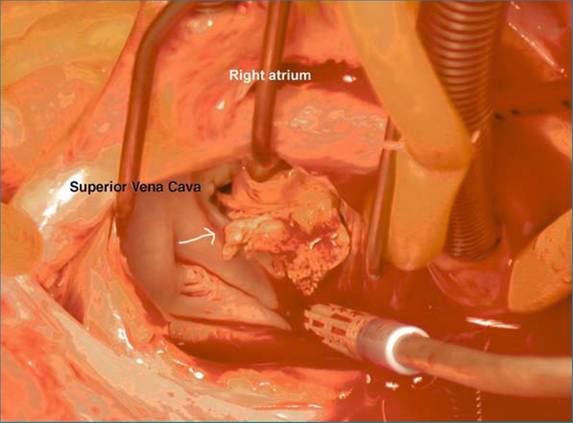
Fig. 3 Mitral vegetations
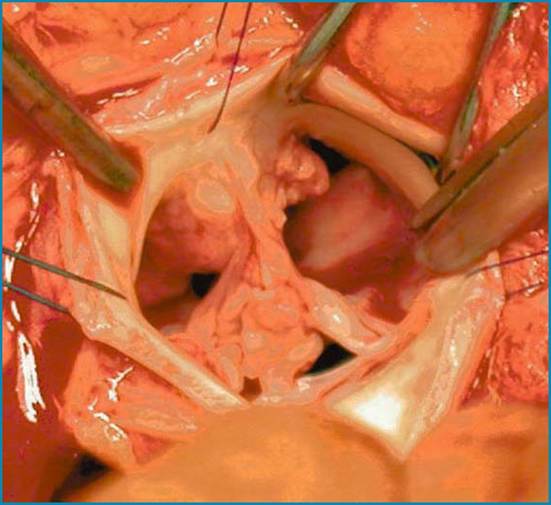
Fig. 4 Aortic vegetations