STATE-OF-THE-ART HAART TREATMENT
Standard of care anti-HIV treatment dictates the combined use of three or more of the 21 approved antiretroviral agents. These derive from four different classes of drugs: nucleoside reverse transcriptase inhibitors (NRTIs), nonnucleoside reverse transcriptase inhibitors (NNRTIs), protease inhibitors (PIs), and entry inhibitors (Figure 28.1).
Treatment goals are durable viral suppression, restoration of immunologic function, reduction in HIV pathogenesis, and improvement in the quality of life, with minimal drug-related toxicities. For the most part, clinicians rate the success of these combinations by looking at viral suppression and recovery of CD4 T cells in the absence of toxicity and viral escape. However, if patients stop all therapy, viral load rebounds and the incomplete state of immune reconstitution recovered during HAART quickly erodes.17 Furthermore, it is generally accepted that although the advent of HAART greatly reduced HIV morbidity and mortality, these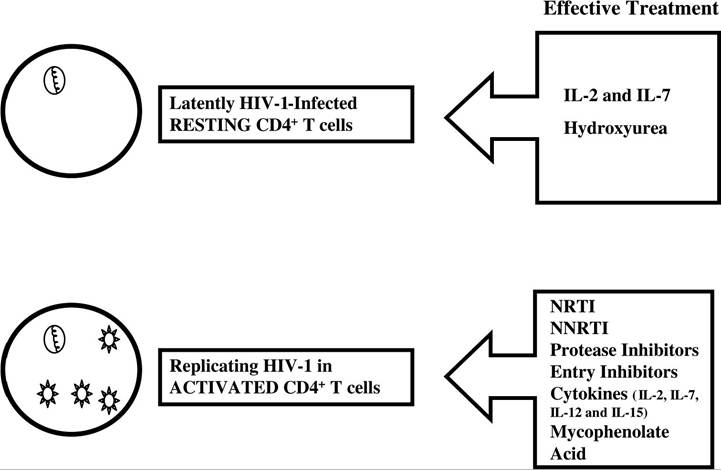
FIGURE 28.1 HIV-1 treatment. Targeting replicating HIV-1 in activated lymphocytes may be accomplished by the combination of the four approved classes of antivirals (NRTI, NNRTI, PI, and entry inhibitors) and likely by the addition of cytokines and virostatics. The ultimate challenge is to eliminate reservoir virus in latently infected resting cells (CD4 and macrophage). Some cytokines may “tickle out” the virus, and hydroxyurea may have indirect or direct antiviral effects in resting lymphocytes.
drug combinations are not free of serious drawbacks (i.e., drug-related toxicities, emergence of drug-resistant strains, difficulty of adhering to regimens, and extremely high costs, that make them inaccessible in developing nations). Thus, we need to devise maintenance therapies that are easier to tolerate, contain viral expansion (to what minimal level may need to be revised), and fully restore the immune system. Moreover, we need to investigate and address what is happening in virally suppressed patients: why is immune reconstitution incomplete, and how can we remedy this situation?
Many studies confirm the observations mentioned in the introduction and pose additional relationships that correlate HIV infection with induced apoptosis and immune dysfunction, including the following: T cell population subsets and T cell receptor repertoire are skewed during HIV-1 infection, and HAART does not always restore preinfection homeostasis; it is probable that different mechanisms induce apoptosis in CD4 and CD8; HAART reduces apoptosis, but the mechanisms responsible remain elusive; and immune dysfunction may be indirectly linked to apoptosis.