The Tests
There are two general tests that detect HIV infection. Both tests are done with blood, although tests using saliva and urine are also available. One blood test detects the antibody to the virus; the other detects evidence of the virus itself.
Tests for Antibodies to HIV
The standard test to detect HIV actually detects the antibody to HIV. Antibodies are proteins the body makes to kill any microbe that invades human tissues. If antibodies are present, the microbe also is, or has been, present. Testing has been done to identify antibodies to many microbes for several decades; it is a common method for finding the microbes that cause a multitude of infectious diseases.
Virtually everyone with HIV has a positive test. The only exception is that the time between infection with the virus and formation of the antibodies can be 3 to 6 weeks, or even (rarely) up to 24 weeks. The result is that some people with recent infection will not show antibodies to HIV, and will not have positive results, despite having HIV. When we suspect this might be the case, we usually repeat the test in 2 to 3 months; or if it’s important to know the results immediately, we test for the virus itself.
People with a positive antibody test nearly always have HIV infection. The usual exception is human error—such as a mix-up in the report of the results or in the tubes of blood. If someone tests positive and the positive results don’t make sense, we repeat the antibody test.
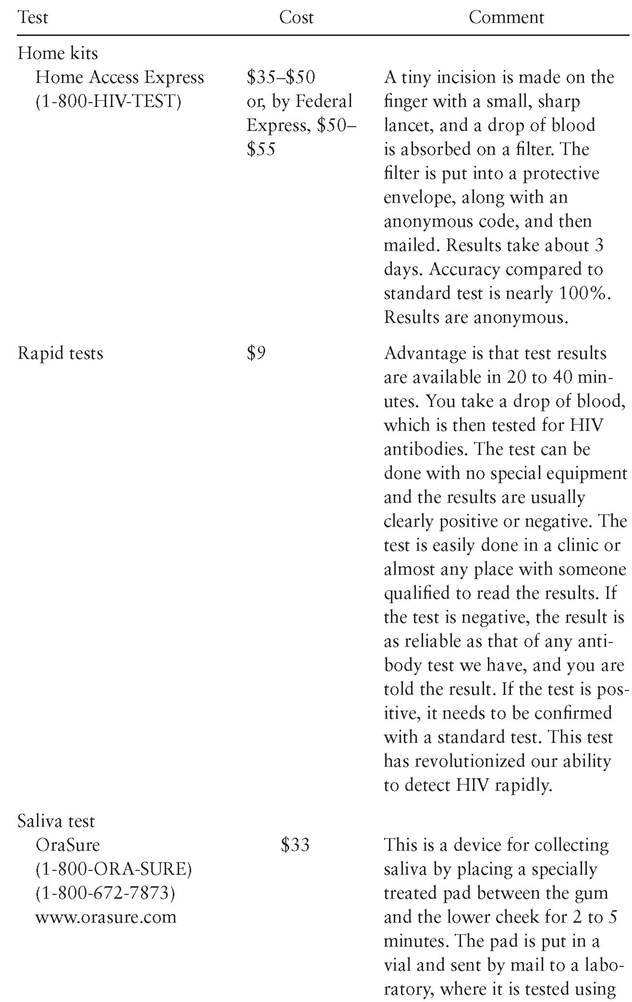
Some test methods offer special advantages (see table 10); some avoid a needlestick by using not blood but urine or saliva; rapid tests give results not in one to two weeks but in less than an hour; and selftests allow complete anonymity. These tests are all approved by the FDA, but they vary somewhat in accuracy. They all use standard scientific methods to detect antibodies to HIV—just as the standard blood test used since 1985 does.
Tests for HIV
Tests that measure “quantitative HIV” or “viral load” detect not antibodies to the virus, but the virus itself and its concentration in the blood.
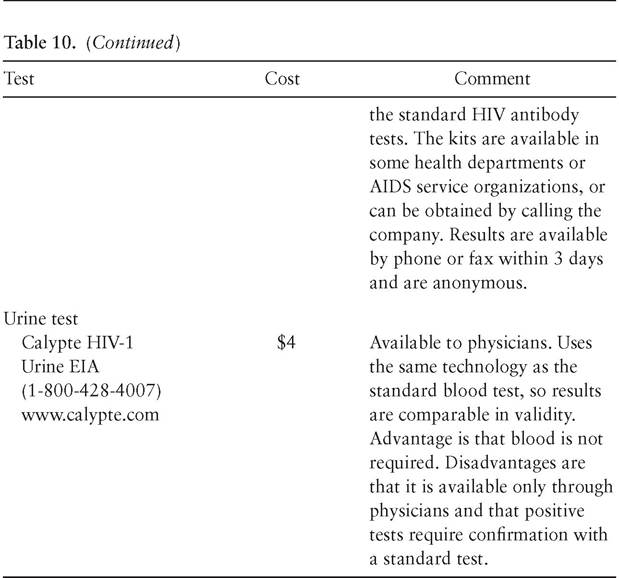
Table 10. Tests for HIV Antibody
(continued)
Although the test is done on blood, most of the HIV is in other places in the body, mostly in the lymph nodes. Nevertheless, the test on blood does accurately represent the amount of HIV in the body.
The viral load tests commonly used give results in “copies per milliliter of blood,” or “copies/ml.” One “copy” is one virus. The test will measure between about 500 copies/ml and 750,000 copies/ml. So-called ultra-sensitive tests will detect as few as 50 copies/ml. People with untreated HIV infection have a wide range of viral loads, but the average is about 30,000 copies/ml.
The highest viral loads occur in the first three to four weeks of infection, before the person’s antibodies have had time to kick in. After that, the viral load drops to a “set point” where, if the person doesn’t get treatment, it stays for years. If the set point is high, the infection progresses rapidly—that is, the CD4 count declines quickly and the time before HIV complications set in is short. People in this situation are called “rapid progressors.” If the set point is low, the infection progresses slowly; these people are called “chronic non-progressors.”
The difference between rapid progressors and chronic non-progres- sors may lie either in the virulence of the virus or in the quality of the person’s immune system—the latter probably being more important. Don’t confuse the quality of the immune system’s response to HIV with its response to other infections. The immune system’s ability to control HIV has nothing to do with its ability to control other infections. A person who seems to catch every circulating flu bug is as likely to be a chronic non-progressor as someone who never seems to get sick.
The goal of HAART is to kill the virus, that is, to get the viral load as low as possible for as long as possible. Our target is usually a viral load of less than 50 copies/ml, or “undetectable,” within six months of starting the therapy. This target is virtually always possible, but it has three caveats. (1) The virus must be susceptible to three drugs in the HAART regimen. (2) The person taking the drugs must stick closely to the regimen. (3) The HAART drug must have no side effects or interactions with other drugs that keep them from getting to where the virus is.
A medical rule is, the viral load dictates the probability of transmission. In other words, the more virus, the more likely the transmission to others. This is true of all infections, not just HIV: the larger the number of microbes, the more likely the infection is to be transmitted. The implication is that reducing the viral load with HIV treatment may reduce the probability of transmission. A further implication is that the amount of the reduction in transmission may depend directly on the amount of reduction in viral load. The bottom line is, “no detectable virus” is good and markedly reduces the probability of transmission but never completely eliminates it.