Acute Myeloid Leukemia
Epidemiology and Etiology
AML is the most common type of acute leukemia in adults with an estimated 19,940 new cases in 2020.1 Median age at presentation is around 65 years.
Risk factors are similar to those of MDS. Antecedent MDS or myeloproliferative neoplasms, as well as certain bone-marrow failure syndromes and familial cancer syndromes increase the risk of AML.Pathology
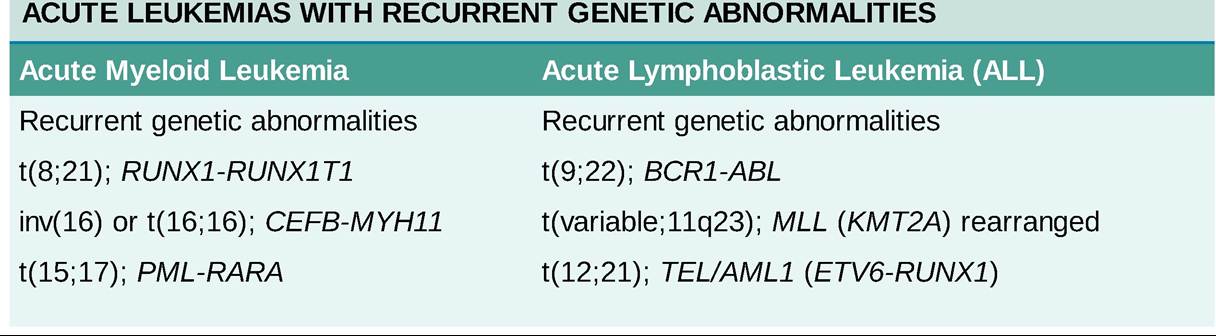
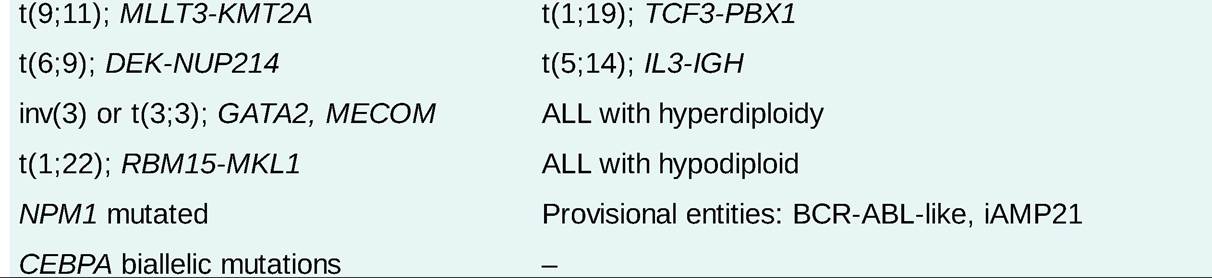
The WHO classification includes six categories for AML: AML with recurrent genetic abnormalities (Table 22-6); AML with MDS-related changes; therapy-related AML; AML, not otherwise specified (NOS); myeloid sarcoma, and myeloid proliferations related to Down syndrome. The AML NOS category includes the traditional French-American-British (FAB) subtypes M0 (AML minimally differentiated), M1 (AML without maturation), M2 (AML with maturation), M4 (acute myelomonocytic leukemia), M5 (acute monocytic leukemia), M6 (acute erythroleukemia), and M7 (acute megakaryoblastic leukemia). The FAB subtype M3 (acute promyelocytic leukemia [APL]) is classified as AML with recurrent genetic abnormalities due to the presence of t(15;17).
TABLE 22-6
Clinical Presentation
Most patients present with pancytopenia, circulating blasts, and symptoms related to cytopenias, including fatigue and dyspnea due to anemia, fever/infection due to leukopenia, and easy bruising/bleeding due to thrombocytopenia. Leukostasis is a medical emergency and may be manifested by dyspnea, chest pain, headache, confusion, or neurologic deficits. Extramedullary tissue invasion by leukemic cells (most commonly with AML-M5) can result in hepatomegaly, splenomegaly, lymphadenopathy, rashes (leukemia cutis), gingival hypertrophy, CNS dysfunction, cranial neuropathies, or infiltrative masses (granulocytic sarcomas or chloromas).
Diagnostic Testing
AML is defined by the presence of #8805;20% blasts in the bone marrow or in the peripheral blood. AML with t(8;21), inv(16) and t(15;17) can be diagnosed irrespective of the blast percentage. Bone marrow specimens should be submitted for routine pathology, IHC, flow cytometry, cytogenetics, FISH, and molecular testing/sequencing. This information is used to classify AML into prognostic groups and to guide treatment.33
TREATMENT
• Induction: standard intensive induction chemotherapy for AML typically consists of the “7 + 3” regimen which includes cytarabine over 7 days given concurrently with an anthracycline (daunorubicin or idarubicin) for 3 days. Approximately 60%-80% of AML patients achieve a remission with induction chemotherapy. However, nearly all patients achieving a remission will eventually relapse without additional consolidation therapy. The addition of targeted agents to 7 + 3 induction may include midostaurin (multikinase FLT3 inhibitor) in FLT3 mutated AML and gemtuzumab ozogamicin (CD33 ADC) typically used in younger CD33 positive AML patients with favorable risk disease. In patients who are ineligible for intensive induction chemotherapy, venetoclax (BCL2 inhibitor) in combination with a hypomethylating agent (azacitidine or decitabine) or the combination of glasdegib (hedgehog pathway inhibitor) with low-dose cytarabine may be considered. In patients with therapy-related AML and AML with MDS-related changes, CPX-351 (liposomal cytarabine and daunorubicin) may be considered. Additional targeted therapies for patients with AML harboring specific mutations may include decitabine for TP53, ivosidenib for IDH1, enasidenib for IDH2, and gilteritinib for FLT3 mutated AML.34
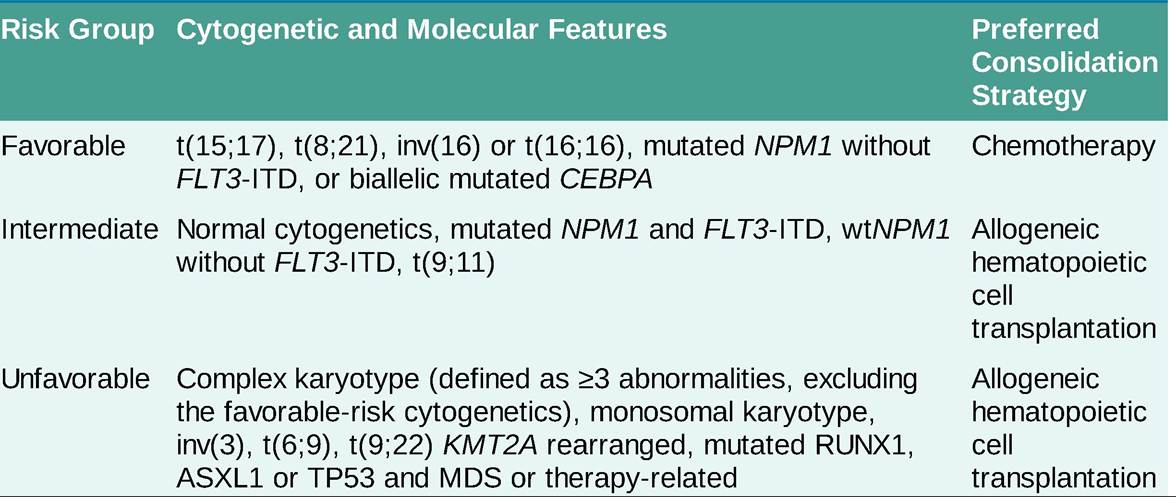
• Consolidation: intensive consolidation typically includes high-dose cytarabine (HiDAC) with or without subsequent allogeneic stem cell transplantation depending on risk group (Table 22-7). Also see section “Principles of Stem Cell Transplantation.”
TABLE 22-7
CYTOGENETIC ABNORMALITIES IN ACUTE MYELOID LEUKEMIA AND ASSOCIATED PROGNOSIS
• Relapsed/refractory AML is associated with very poor prognosis and may be managed with salvage chemotherapy, targeted therapies, tapering of immunosuppression with donor lymphocyte infusion if relapsing after allo-transplant, or enrollment in clinical trials.
• APL (AML-M3) represents a unique subset of AML which is characterized by high cure rates. Treatment includes the use of all-trans-retinoic acid (ATRA) and arsenic trioxide (ATO) for low- intermediate-risk patients (WBC #8804;10 ? 109#8725;L at presentation) and ATRA, ATO, and the addition of an anthracycline for high-risk patients (WBC gt;10 ? 109#8725;L at presentation). Glucocorticoids may also be added to the induction regimen for APL as prophylaxis for or treatment of differentiation syndrome.