Appendix A Immunizations and Postexposure Therapies
Carlos Mejia-Chew1 Stephen Y. Liang
Introduction
• Active immunization promotes the development of a durable primary immune response (B-cell proliferation, antibody response, T-cell sensitization) directed toward a specific pathogen such that subsequent exposure to that pathogen results in a secondary immune response that protects against infection (Table A-1).
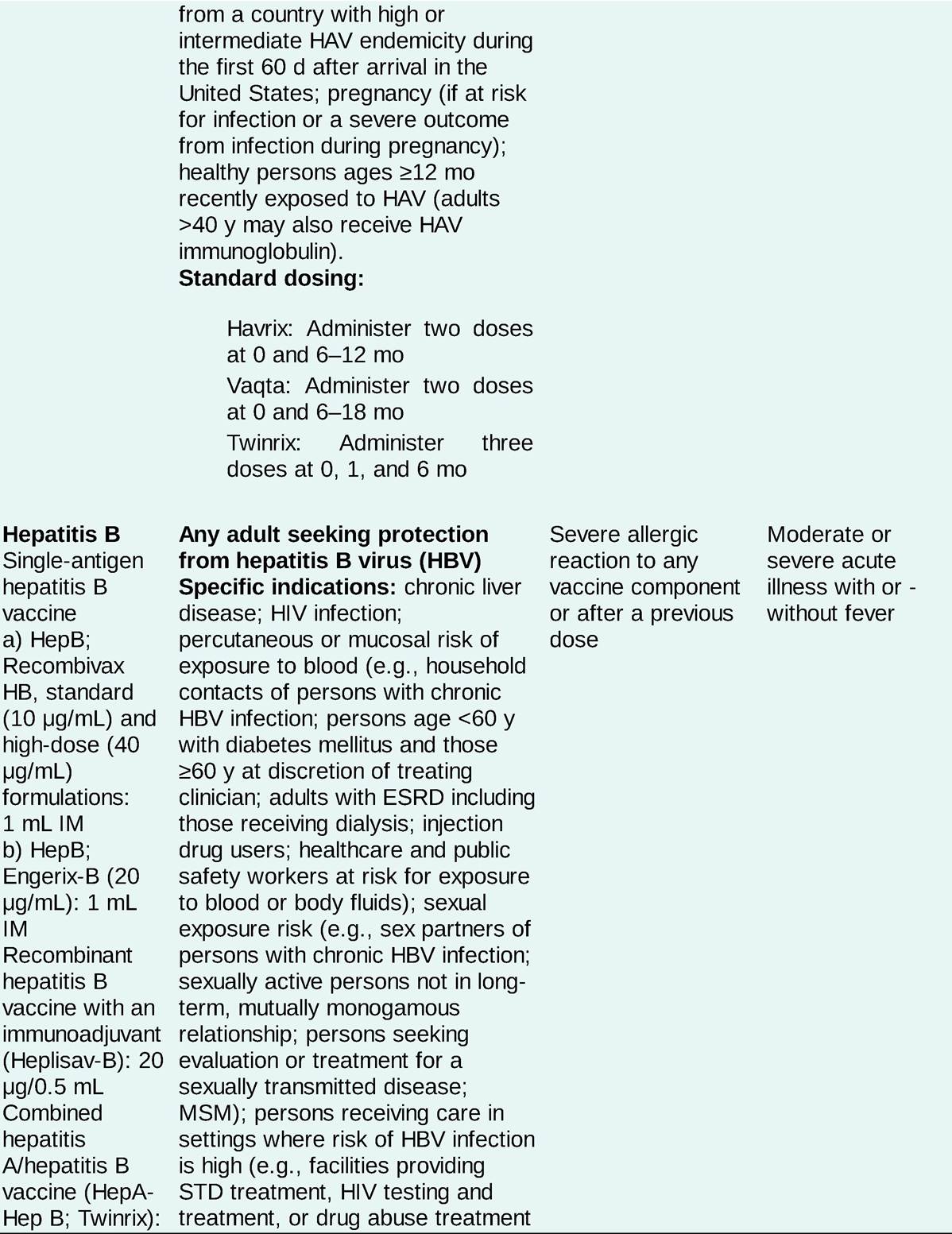
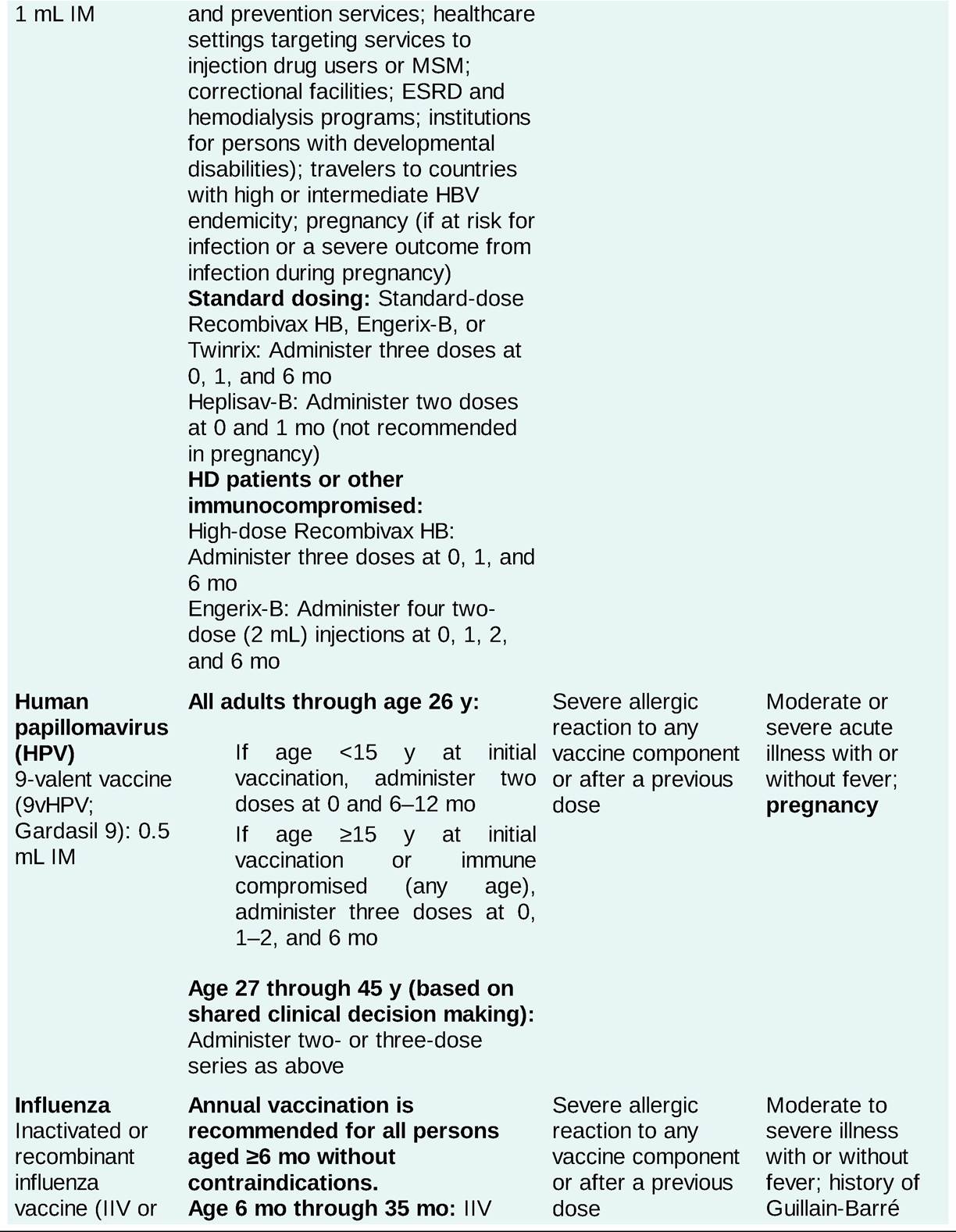
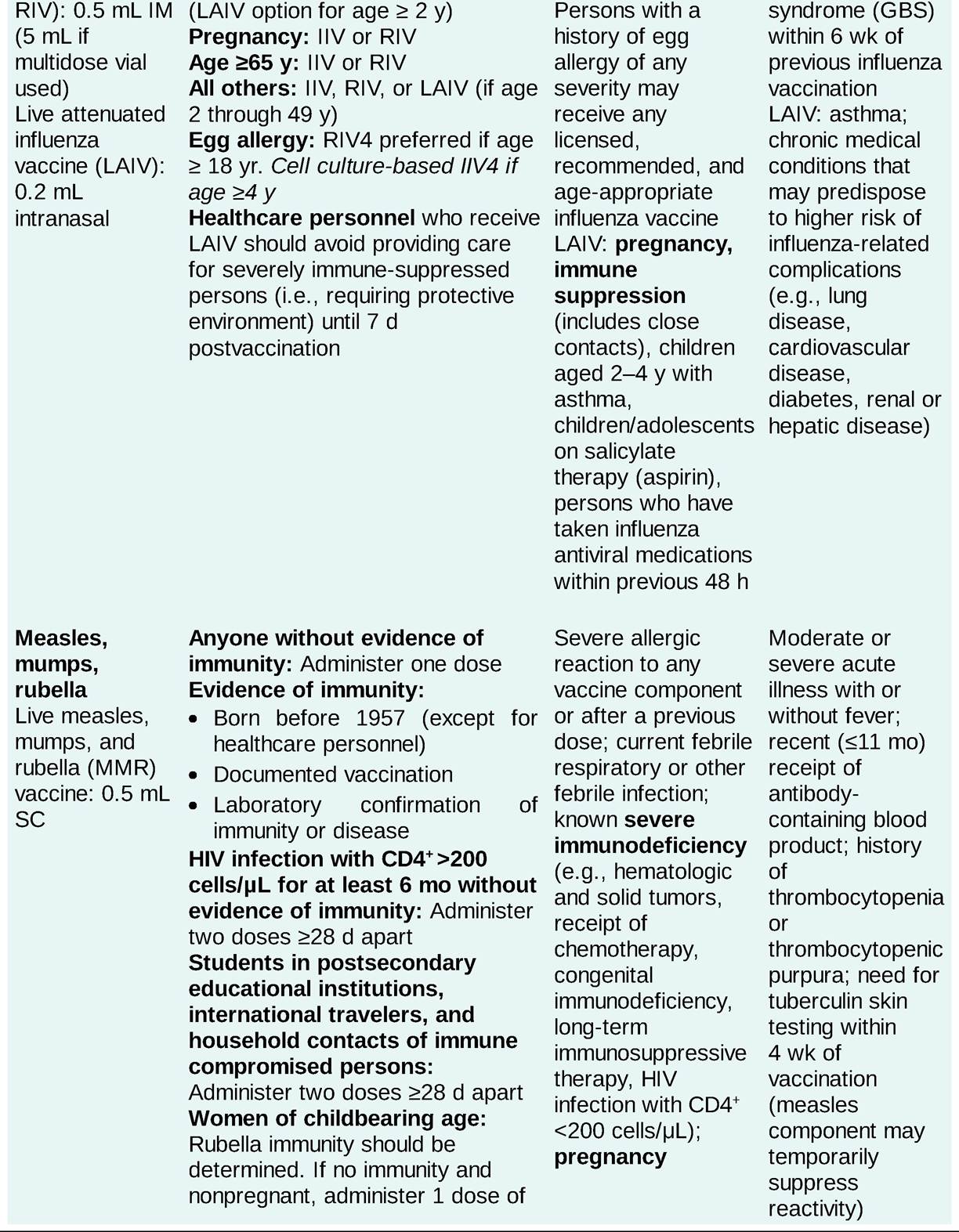
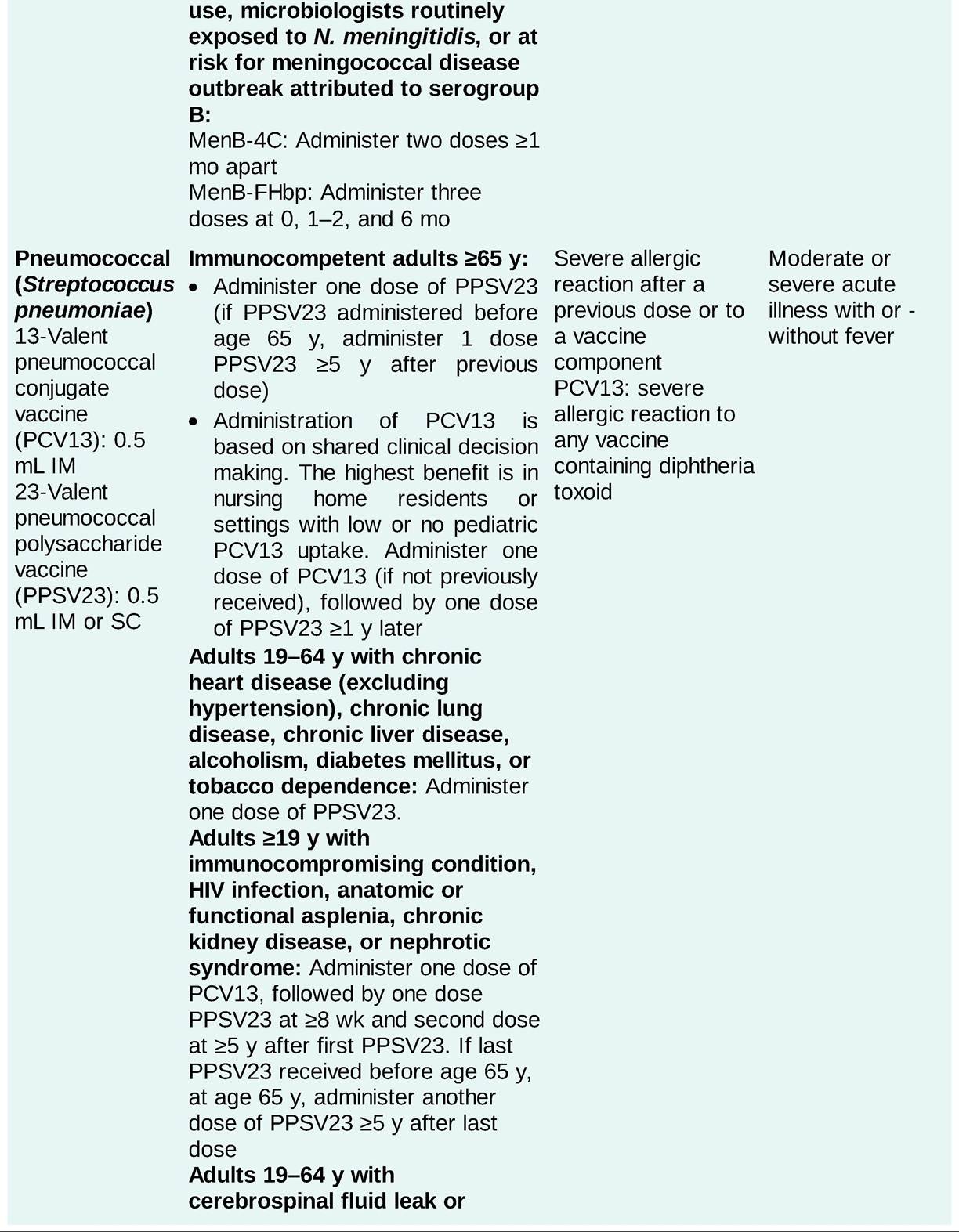
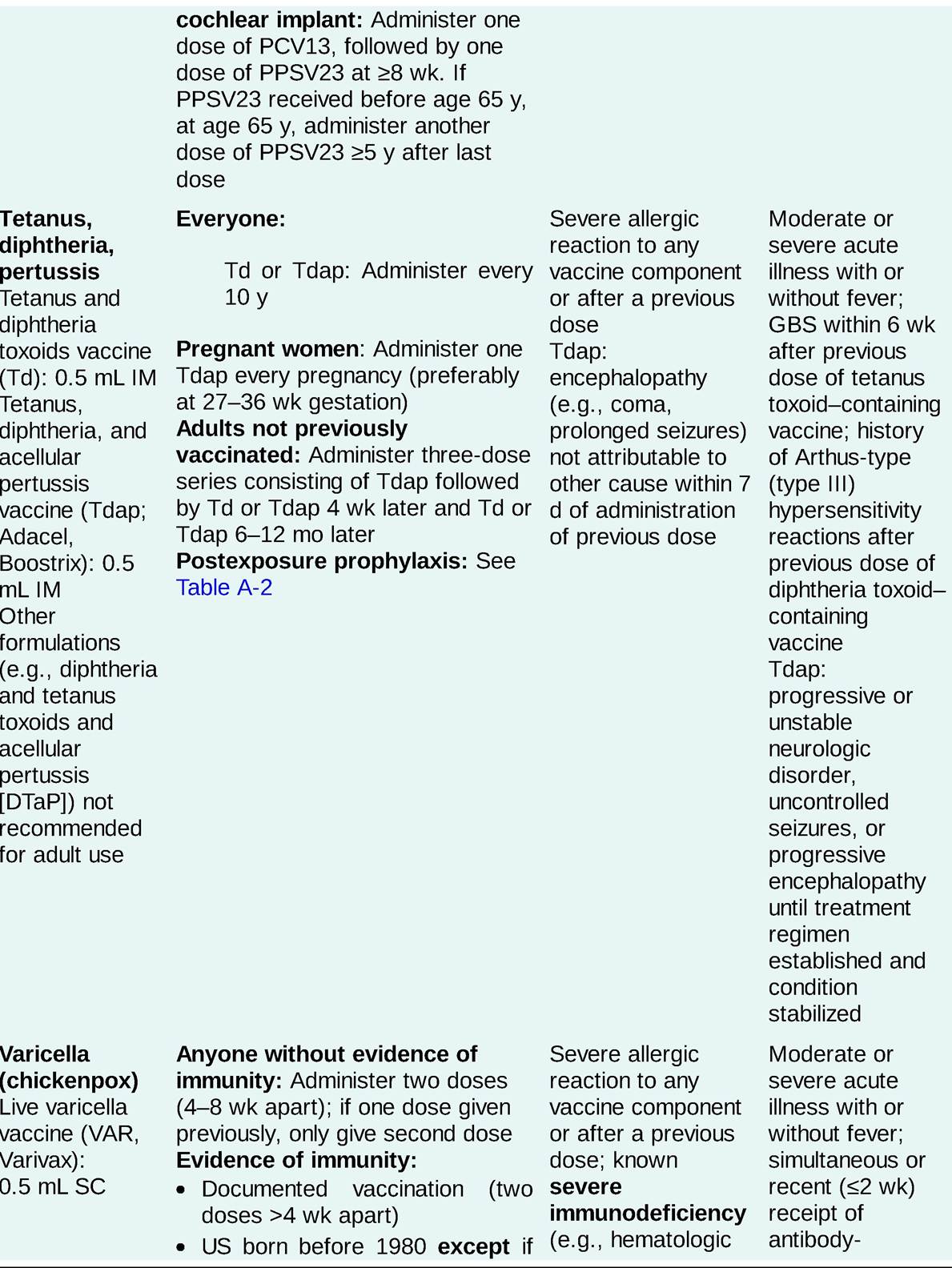
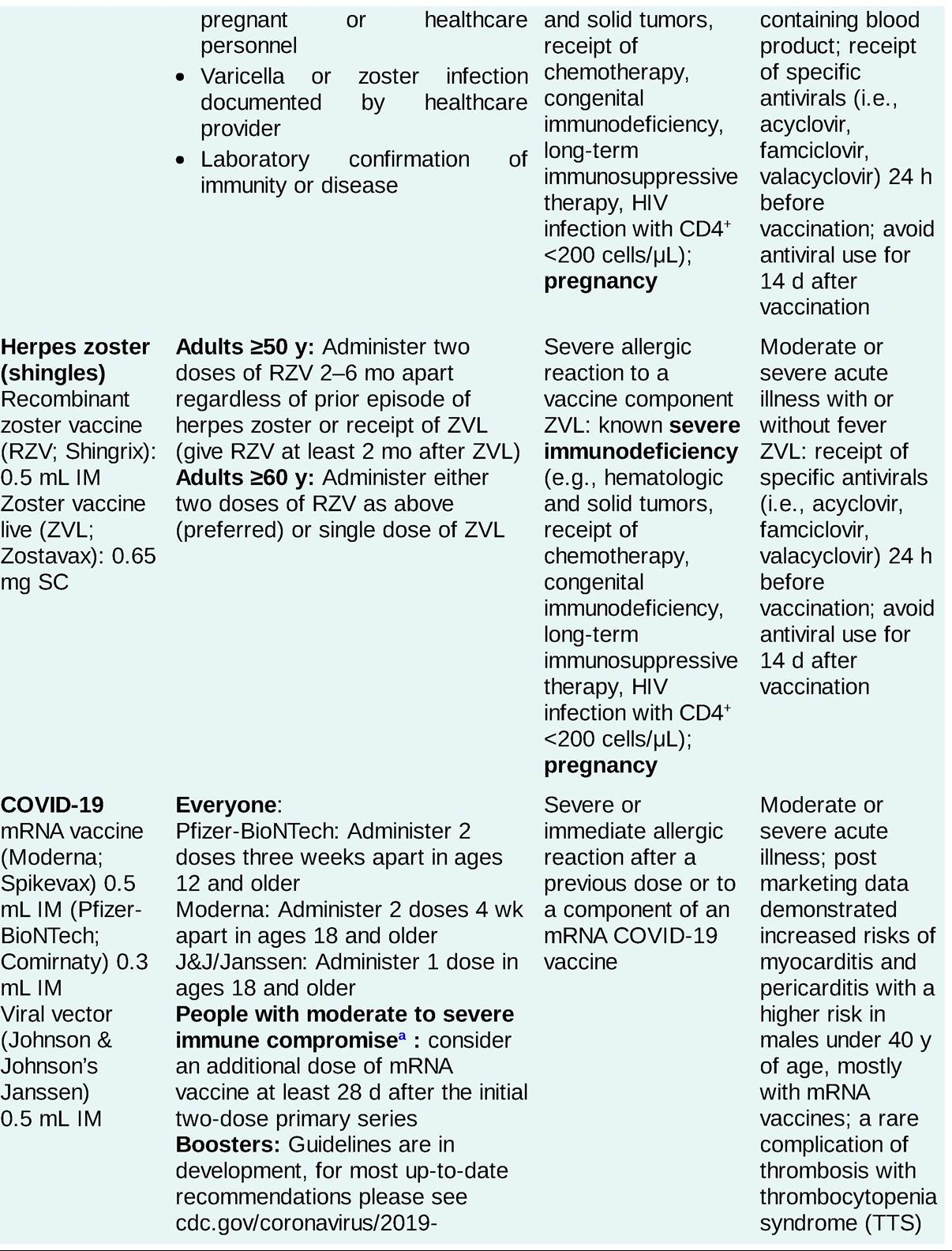
TABLE A-1
SELECTED ADULT IMMUNIZATION RECOMMENDATIONS IN THE UNITED STATES
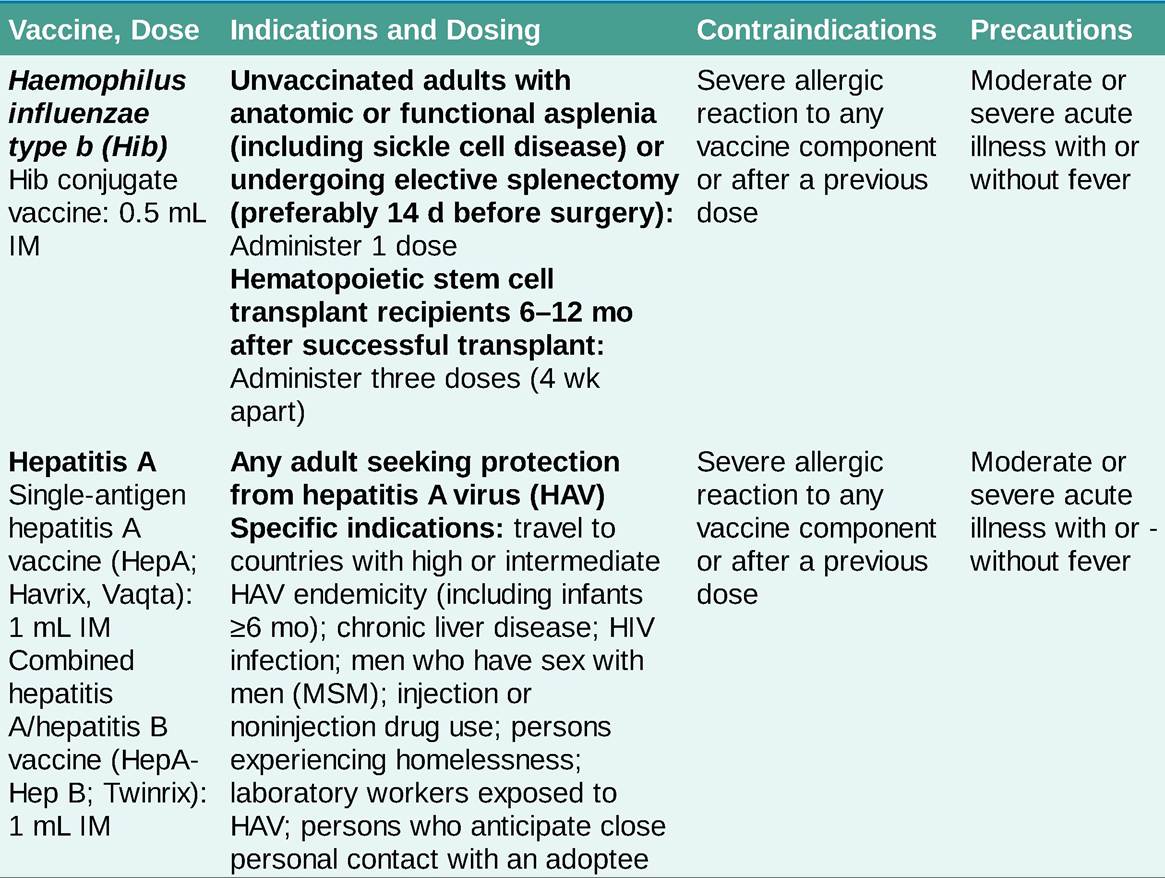
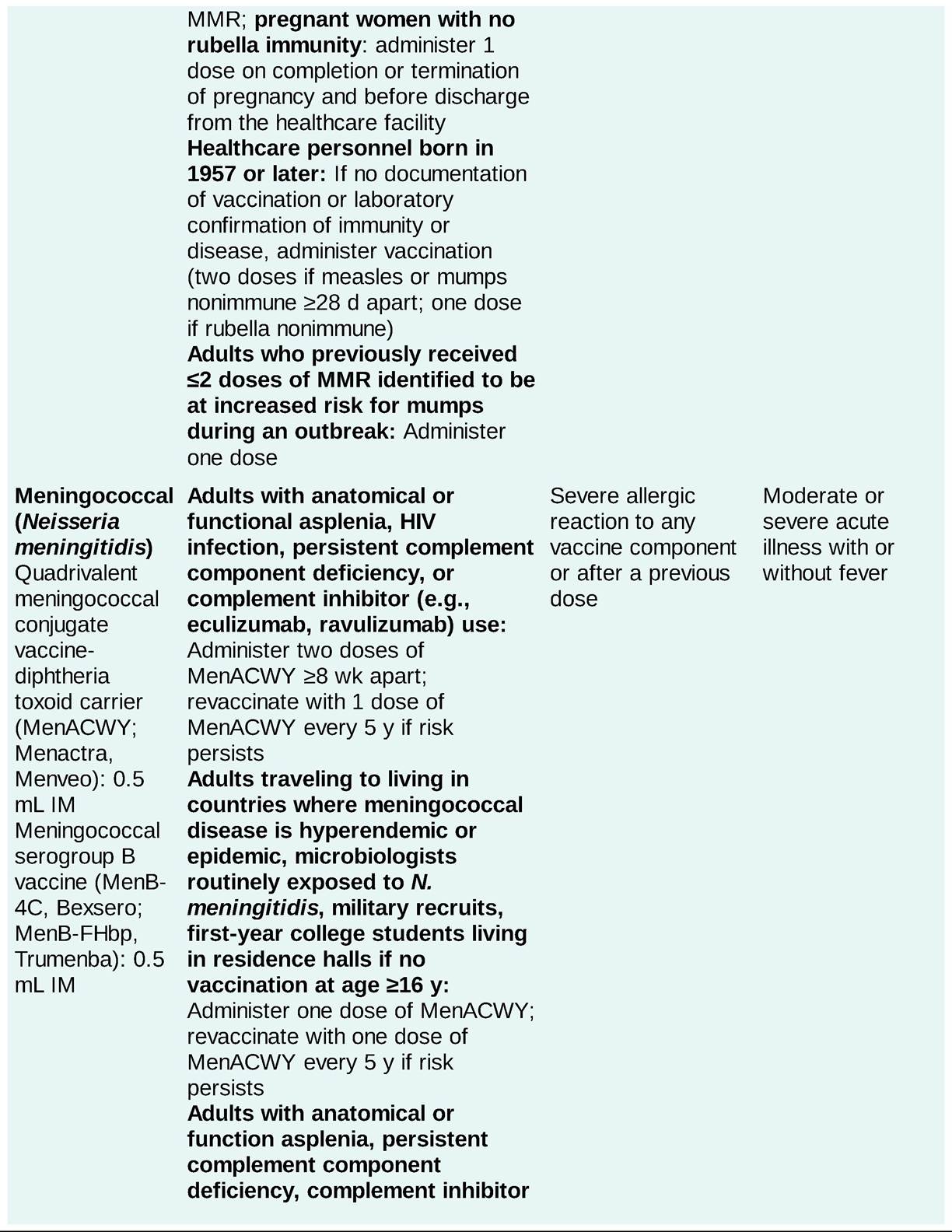

Adapted from Centers for Disease Control and Prevention. Advisory Committee on Immunization Practices recommended adult immunization schedule for ages 19 years or older—United States, 2020.
https://www.cdc.gov/vaccines/schedules/hcp/imz/adult.html
ESRD, end-stage renal disease
aNot limited to: moderate or severe primary immunodeficiency (e.g., DiGeorge syndrome, Wiskott-Aldrich syndrome); advanced/untreated HIV infection; active treatment for malignancies, solid-organ transplant; chimeric antigen receptor (CAR)-T- cell or hematopoietic stem cell transplant; immunosuppressive therapy (e.g., alkylating agents, antimetabolites, transplant-related immunosuppressive drugs, cancer chemotherapeutic agents, tumor-necrosis factor [TNF] blockers, and other biologic agents, and high-dose corticosteroids equivalent to prednisone #8805;20 mg/day for #8805;2 wk).
• Passive immunization involves the administration of immune globulin resulting in transient protection against infection. It is usually employed in a host with limited capacity to mount a primary immune response, when exposure to a pathogen occurs in a previously unvaccinated host, or to protect against toxin-mediated disease.
• Postexposure prophylaxis is therapy given following exposure to a pathogen to prevent the development of disease. This can include active immunization, passive immunization, and/or antimicrobial therapy (Tables A-2 and A-3).
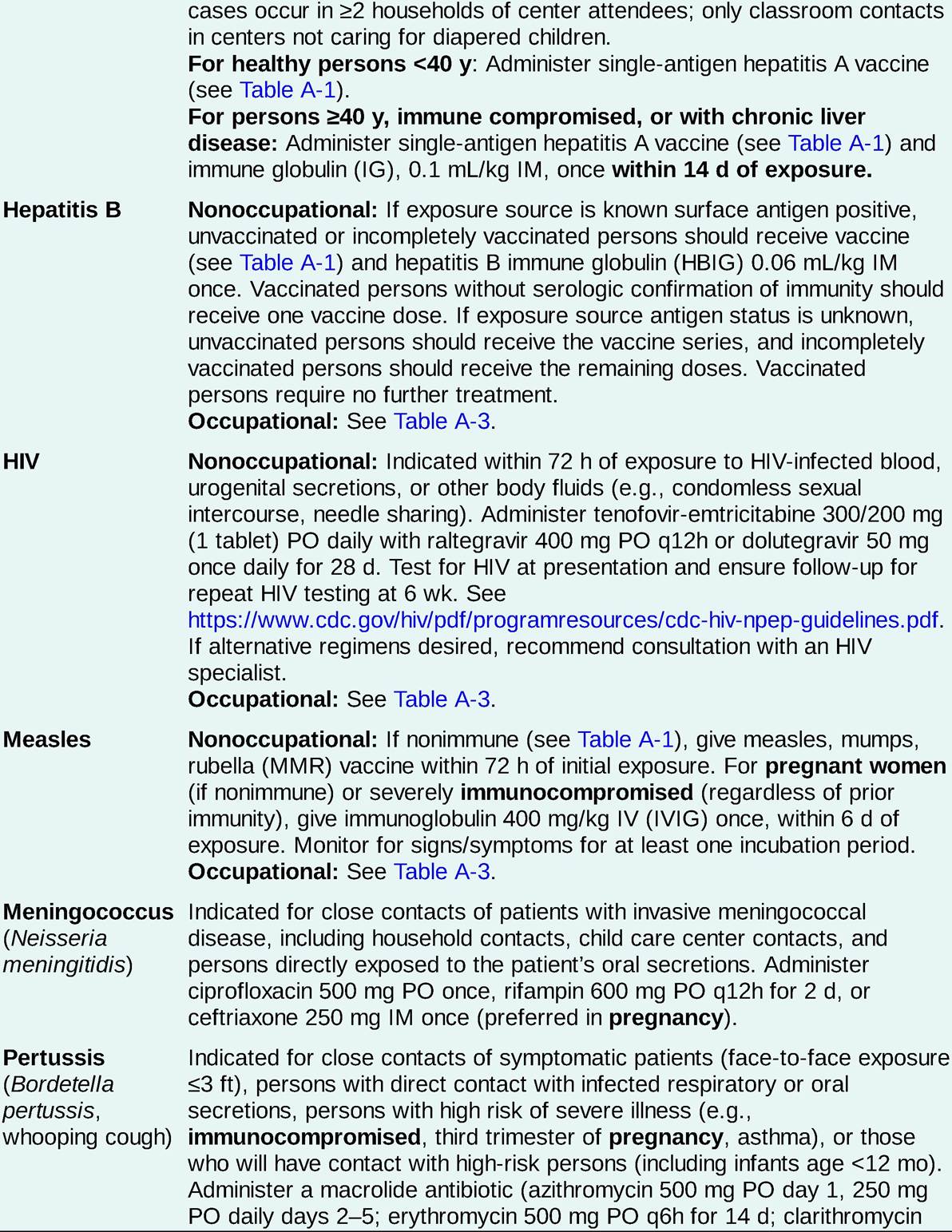
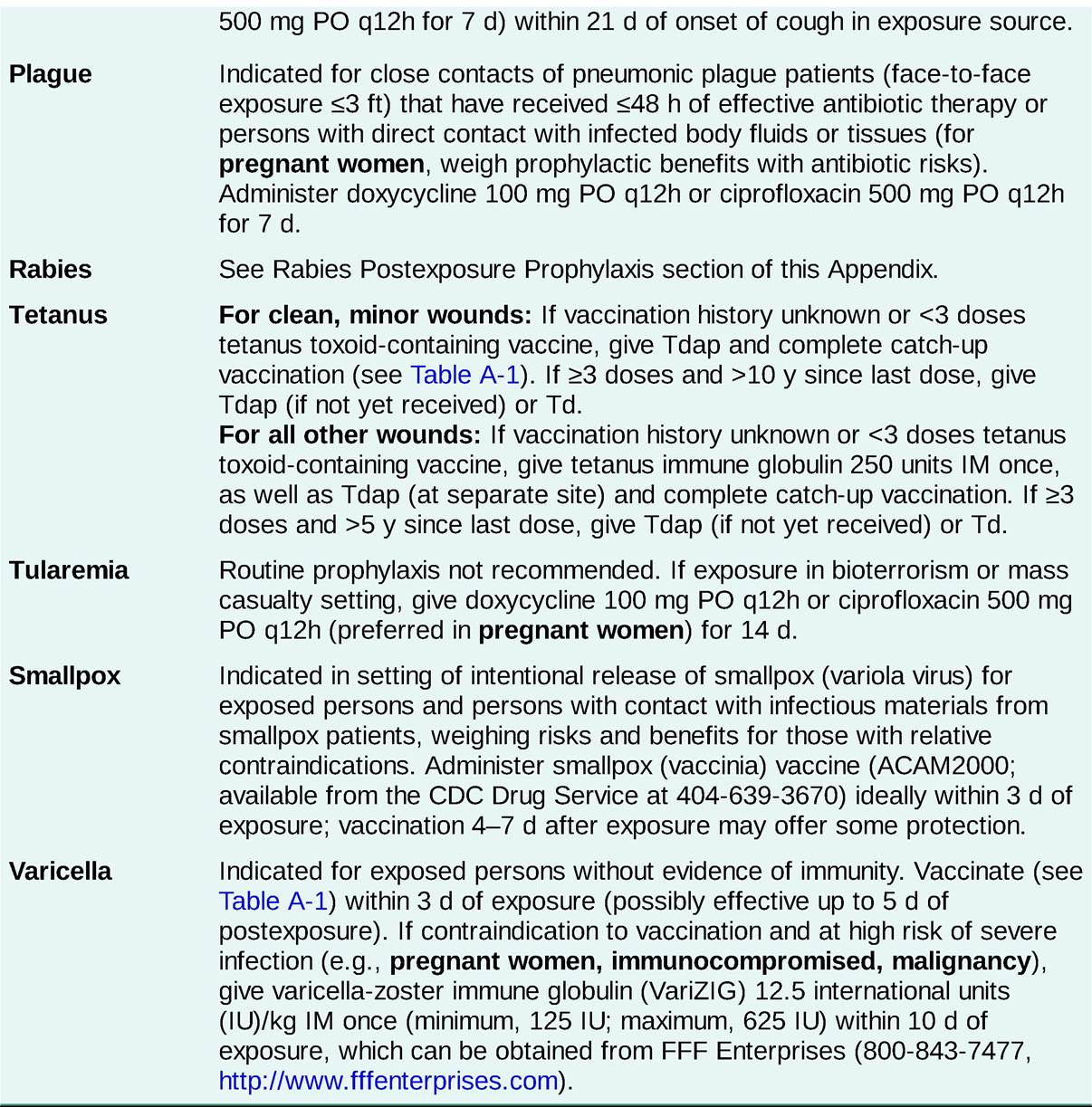
TABLE A-2
SELECTED ADULT POSTEXPOSURE PROPHYLAXIS RECOMMENDATIONS
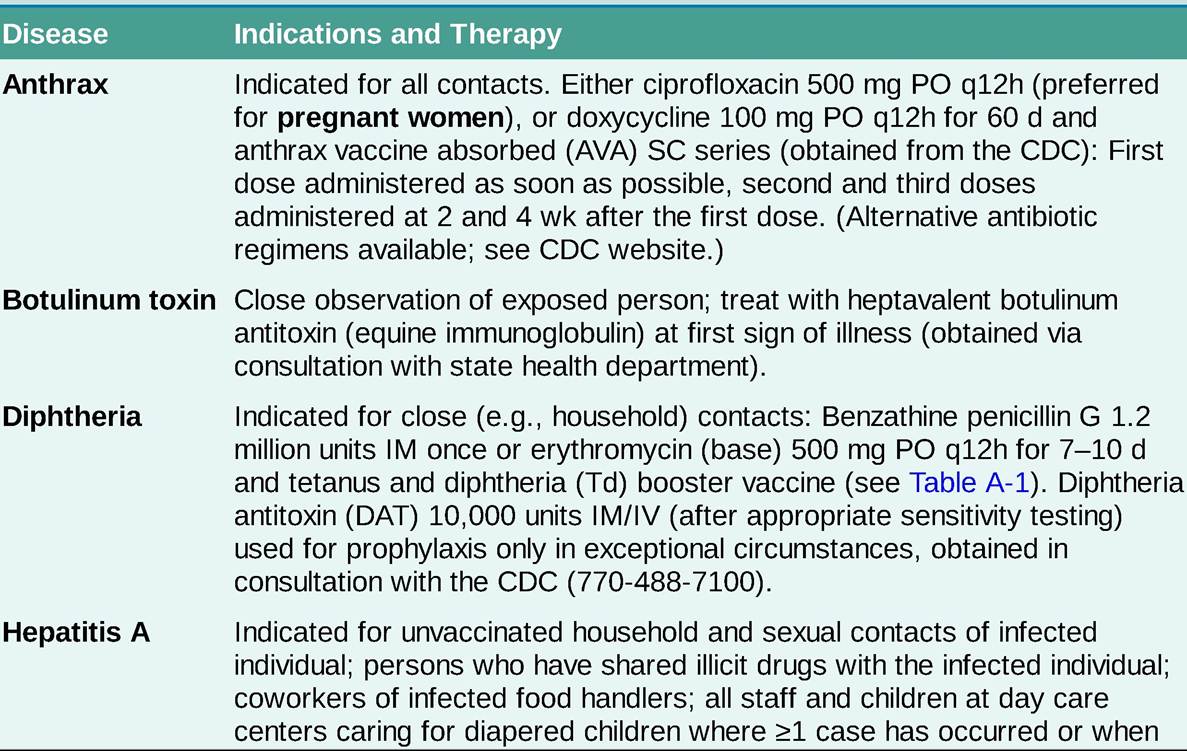
CDC, Centers for Disease Control and Prevention; Tdap, tetanus, diphtheria, pertussis.
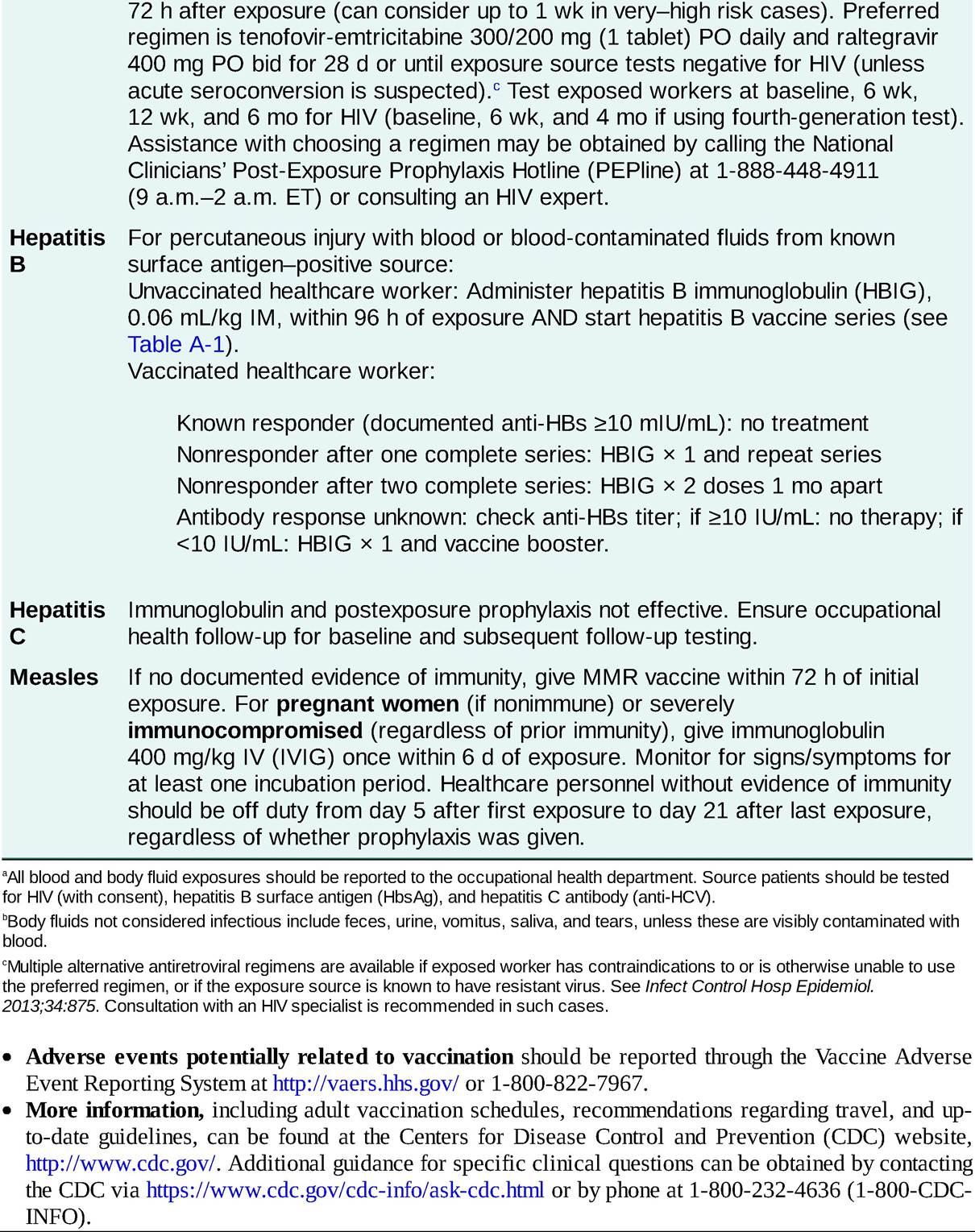
SELECTED POSTEXPOSURE GUIDELINES FOR HEALTHCARE PERSONNELa

Rabies Postexposure Prophylaxis
• For all suspected rabies exposures, consultation with local or state health officials is recommended. Contact information can be found at http://www.cdc.gov/rabies/resources/contacts.html.
• Postexposure prophylaxis is generally indicated only for bite wounds from mammals.[1]
î Bites from bats, skunks, raccoons, foxes, and most other carnivores warrant immediate prophylaxis unless the animal is confirmed to be rabies negative by laboratory testing. Animals should not be held for observation but euthanized as soon as possible.
î Bites from dogs, cats, and ferrets that are rabid or suspected to be rabid also warrant immediate prophylaxis. If the animal is healthy and can be observed for 10 days, do not begin prophylaxis but observe.
If signs or symptoms of rabies develop in the animal, prophylaxis should begin immediately. For bites where the status of the animal is unknown, consult with public health officials.î Bites from all other sources (e.g., rodents, hares, livestock) should be considered on an individual basis and prophylaxis initiated in consultation with public health officials.
• Postexposure prophylaxis consists of wound care, vaccination, and in certain situations, administration of human rabies immune globulin (HRIG) (Table A-4).[2]
° All wounds should be cleaned thoroughly with soap and water and irrigated with a virucidal solution such as povidone-iodine.
TABLE A-4
| RABIES POSTEXPOSURE PROPHYLAXIS RECOMMENDATIONS | ||
| Vaccination Status | Therapy | |
| Vaccine | HRIG | |
| Not previously vaccinated | Yes, on days 0, 3, 7, and 14 | Yes, once on day 0 |
| Previously vaccinated | Yes, on days 0 and 3 | No |
HRIG, human rabies immune globulin.
î Human diploid cell vaccine or purified chick embryo cell vaccine, 1 mL IM, should be administered in the deltoid region, the only acceptable site for vaccination in adults.
î If HRIG is indicated, give 20 IU/kg IM once. Do not administer in the same syringe as the vaccine. When possible, infiltrate as much of the product around and into the wound(s). The remaining volume can be administered intramuscularly at any site anatomically distant from the site of vaccination. Subsequent vaccine doses at later dates can be given at the same site as previous HRIG.
REFERENCES
Immunization Practices. MMWR Recomm Rep. 2010;59(RR-2):1-9.
3. National Center for Immunization and Respiratory Diseases (NCIRD). Selective Adverse Events Reported after COVID-19 Vaccination. 2021. Accessed date September 28, 2021. cdc.gov/coronavirus/2019-ncov/vaccines/safety/adverse-events.html