Appendix B Infection Control and Isolation Recommendations
Caline Mattar, Stephen Y. Liang
• Standard Precautions should be practiced on all patients at all times to minimize the risk of healthcare-associated infection.
î Performhand hygiene with an alcohol-based hand sanitizer before patient contact, before clean or aseptic procedures, after body fluid exposure, after touching a patient (including after gloves are removed), and after touching patient surroundings (Figure B-1, Table B-1).
Soap and water should be used to clean visibly contaminated hands and after contact with patients with confirmed or suspected Clostridioides difficile infection if the alcohol-based preparation used is not active against C. difficile spores.Your 5 moments for
HAND HYGIENE
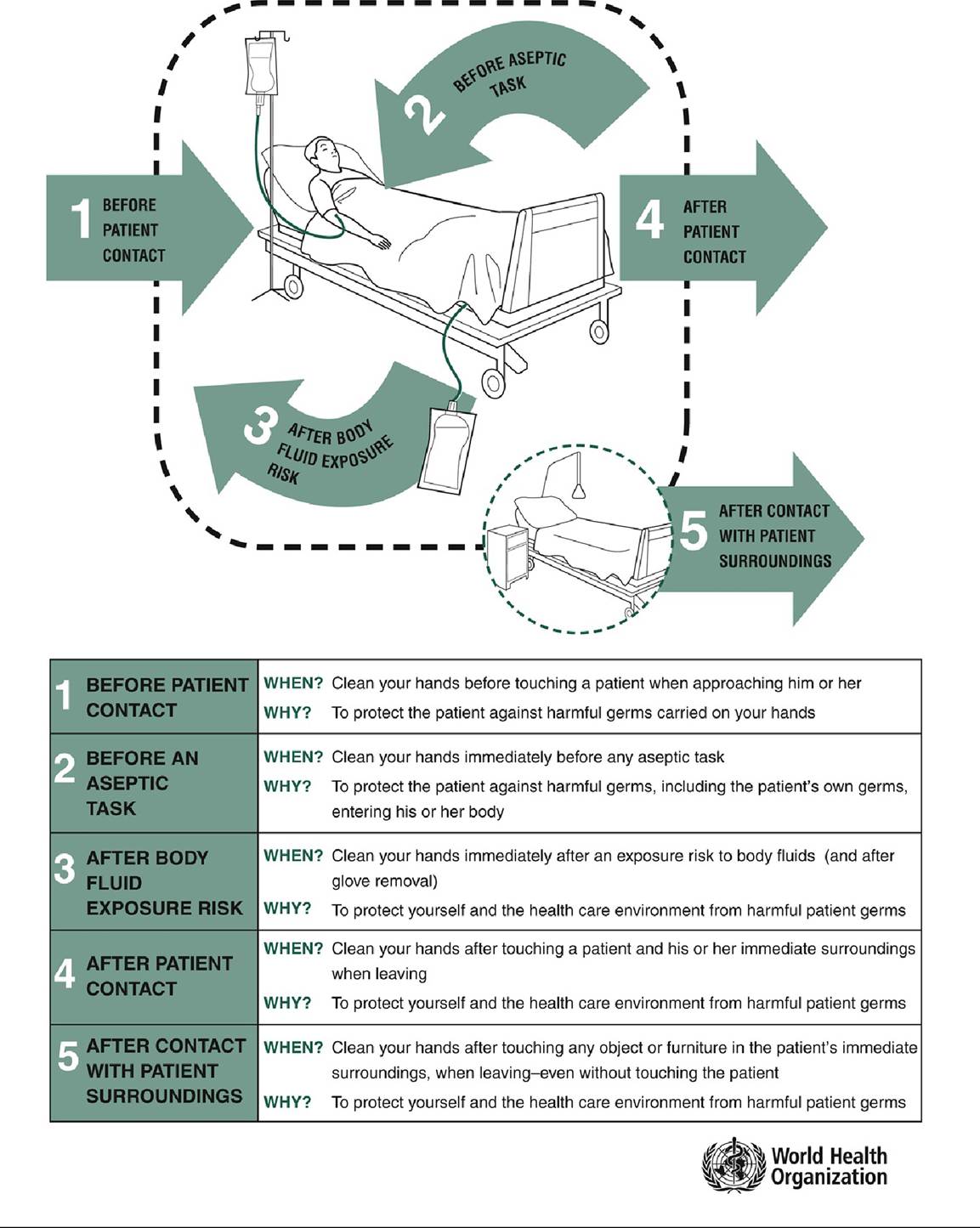
Figure B-1 World Health Organization’s My Five Moments for Hand Hygiene.From World Health Organization’s 5 Moments for Hand Hygiene in acute care settings.(Reproduced, with permission of the publisher, from “Five Moments for Hand Hygiene,” World Health Organization; 2009. Accessed February 2021. https://www.who.int/gpsc/tools/5momentsHandHygiene_A3.pdf?ua=1)
| HEALTHCARE ISOLATION RECOMMENDATIONS FOR SPECIFIC INFECTIONS | ||
| InfectionZCondition | Type | Duration, Comments |
| Adenovirus, pneumonia | Droplet, Contact | Duration of illness In immunocompromised hosts, extend duration of precautions owing to prolonged viral shedding. |
| Anthrax | Standard | Duration of illness Contact precautions indicated if wound with uncontained copious drainage. Alcohol hand rubs ineffective against spores; use soap and water or 2% chlorhexidine gluconate solution for hand hygiene. If aerosolizable spore-containing substance (e.g., powder) is present, wear respirator, protective clothing until decontamination is complete. |
| Botulism | Standard | Duration of illness |
| Burkholderia cepacia, pneumonia, or colonization | Contact | Unknown Recommendations will vary by institution. Avoid exposure to persons with cystic fibrosis. Private room preferred. |
| Clostridioides difficile | Contact | Duration of hospitalization and future hospitalizations Recommendations for initiation and discontinuation of precautions will vary by institution. |
| Conjunctivitis, acute viral | Contact | Duration of illness |
| Diphtheria | ||
| Cutaneous | Contact | Until off antimicrobial treatment and two cultures taken 24 h apart are negative |
| Pharyngeal | Droplet | Same as for cutaneous diphtheria |
| Hepatitis, viral | Standard | Duration of illness For hepatitis A and E, contact precautions are indicated for diapered or incontinent individuals. |
| Herpes simplex virus Encephalitis | Standard | Duration of illness |
| Mucocutaneous, recurrent (skin, oral, genital) | Standard | Duration of illness |
| Mucocutaneous, severe (disseminated or primary) | Contact | Until lesions dry and crusted |
| Herpes zoster | See Varicella | |
| Human metapneumovirus | Contact | Duration of illness |
| Influenza | Droplet | Immunocompetent: 7 d after illness onset or until 24 h after resolution of symptoms, whichever is longer Immunocompromised: Duration of illness Respiratory protection equivalent to an N95 respirator is recommended during aerosol-generating procedures. |
| Lice | ||
| Head (pediculosis) | Contact | Until 24 h after start of therapy |
| Body | Standard | Duration of illness Can be transmitted via infested clothing. Wear gown and gloves when handling clothing. |
| Pubic | Standard | Duration of illness |
| Measles (rubeola) | Airborne | Immunocompetent: 4 d after onset of rash Immunocompromised: Duration of illnessa |
| Meningitis, Haemophilus influenzae type B or Neisseria meningitidis | Droplet | Until 24 h after start of therapy For other etiologies of meningitis, standard precautions can be used. |
| Meningococcal disease (N. meningitidis) | Droplet | Until 24 h after start of therapy If colonization without active disease, standard precautions can be used. |
| Middle eastern respiratory syndrome coronavirus (MERS- CoV) | Airborne, Contact | Determine on a case-by-case basis in consultation with local, state, and federal public health authorities. |
| Monkeypox | Airborne, Contact | Airborne: Until monkeypox confirmed and smallpox excluded Contact: Until lesions crusted |
| Multidrug-resistant organisms, infection or colonization (e.g., MRSA, VRE, ESBL) | Contact | Duration of hospitalization and future hospitalizations Recommendations for initiation and discontinuation of precautions will vary by institution and organism. |
| Mumps (infectious parotitis) | Droplet | Until 5 d after onset of symptomsa |
| Mycoplasma, pneumonia | Droplet | Duration of illness |
| Parvovirus B19 (erythema infectiosum) | Droplet | Immunocompromised patient: Duration of hospitalization Transient aplastic crisis or red cell crisis: 7 d |
| Pertussis (Bordetella pertussis, whooping cough) | Droplet | Until 5 d after start of therapy |
| Plague (Yersinia pestis) | ||
| Bubonic | Standard | Duration of illness |
| Pneumonic | Droplet | Until 48 h after start of therapy |
| Poliomyelitis | Contact | Duration of illness |
| Respiratory syncytial virus | Contact | Duration of illness In immunocompromised hosts, extend duration of precautions due to prolonged viral shedding. |
| Rhinovirus | Droplet | Duration of illness Add contact precautions if copious moist secretions. |
| Rubella (German measles) | Droplet | Until 7 d after onset of rasha Pregnant women who are not immune should not care for these patients. |
| Scabies | Contact | Until 24 h after start of therapy For Norwegian scabies: 8 d or 24 h after the second treatment with scabicide |
| Severe acute respiratory syndrome coronavirus (SARS- CoV) | Airborne, Droplet, Contact | Duration of illness plus 10 d after resolution of fever if respiratory symptoms are absent or improving Eye protection (goggles, face shield) also recommended. |
| Severe acute respiratory syndrome coronavirus 2 | Airborne (if performing an aerosolgenerating | Duration of illness; at least 10 d and up to 20 d from symptom onset AND at least 24 h have passed since last fever (without use of fever-reducing medications) AND symptoms have improved. Recommendations |
| (SARS-CoV-2), COVID-19 | procedure), Droplet, Contact | may continue to evolve with the COVID-19 pandemic. Immunocompromised patients may shed virus longer. Expert consultation should be obtained. |
| Smallpox (variola) | Airborne, Contact | Duration of illness; until all scabs have crusted and separated (3-4 wk)a For vaccine complications, see Vaccinia. |
| Streptococcus group A | Droplet | Until 24 h after start of therapy For endometritis or limited skin, wound, or burn infection, standard precautions can be used. |
| Tuberculosis (Mycobacterium tuberculosis) | Recommendations regarding initiation and discontinuation of precautions will vary by institution. | |
| Extrapulmonary, draining lesion | Airborne, Contact | Until patient is improving clinically and drainage has ceased or there are three consecutive negative cultures of drainage Rule out active pulmonary disease. |
| Extrapulmonary, without draining lesion | Standard | Duration of illness Rule out active pulmonary disease. |
| Pulmonary or laryngeal disease, confirmed | Airborne | Until patient is on effective therapy, is improving clinically, and has three consecutive sputum smears negative for acid-fast bacilli collected on separate days |
| Pulmonary or laryngeal disease, suspected | Airborne | Until likelihood of infectious tuberculosis is deemed negligible and either there is another diagnosis that explains the clinical syndrome or the results of three sputum smears for AFB are negative Each of the sputum specimens should be collected 824 h apart, and at least one should be an early- morning specimen. |
| Tularemia | Standard | Duration of illness |
| Vaccinia | Standard | Duration of illnessa Contact precautions recommended for eczema vaccinatum, fetal vaccinia, generalized vaccinia, progressive vaccinia, and blepharitis or conjunctivitis with significant drainage. If unvaccinated, only healthcare workers without contraindications to - vaccine should provide care. |
| Varicella | ||
| Varicella disease (chickenpox) | Airborne, Contact | Until lesions dry and crusteda In immunocompromised host, prolong duration of |
precautions for duration of illness.
| Herpes zoster, - Standard localized (shingles) | Duration of illnessa In immunocompromised host, use airborne and contact precautions until disseminated disease ruled out. |
| Herpes zoster, - Airborne, disseminated Contact | Duration of illnessa |
Viral hemorrhagic fevers
| Ebola virus disease Droplet, Contact | Discontinue only in consultation with local, state, and federal public health officials. In addition to droplet and contact precautions, a powered air-purifying respirator (PAPR) or N95 respirator, examination gloves with extended cuffs, and fluid-resistant or impermeable gowns, aprons, and boot covers are recommended. Detailed information and updated recommendations can be found at http://www.cdc.gov/vhf/ebola/healthcare-us/- hospitals/infection-control.html. |
| Lassa, Marburg, Droplet, and Crimean-Congo Contact fever viruses | Duration of illness Single-patient room preferred. Emphasize use of sharps safety devices and safe work practices, hand hygiene, barrier protection against blood and body fluids, including goggles or face shields, and appropriate waste handling. Use N95 or higher respirators when performing aerosol-generating procedures. |
AFB, acid-fast bacilli; ESBL, extended-spectrum #946;-lactamase; MRSA, methicillin-resistant Staphylococcus aureus; VRE, vancomycin-resistant enterococcus.
aSusceptible healthcare workers should not enter room if immune caregivers are available.
Adapted from Siegel JD, Rhinehart E, Jackson M, et al. 2007 Guideline for isolation precautions: Preventing transmission of infectious agents in healthcare settings. Am J Infect Control. 2007;35:S65-S164. Copyright © 2007 Elsevier. With permission.
î Wear gloves when direct contact with body secretions or blood is anticipated.
î Wear a gown when clothing may be in contact with body fluids.
î Wear a surgical mask when prolonged procedures, including lumbar puncture, are performed.
î Wear a surgical mask and protective eyewear when splashes of body fluid are possible.
î Use proper respiratory hygiene and cough etiquette (applies to all healthcare personnel, patients, and visitors). Mouth and nose must be covered when coughing, and tissues must be disposed of properly. Hand hygiene must be performed after contact with respiratory secretions.
î Safely dispose of sharp instruments, needles, wound dressings, and disposable gowns.
• Transmission-Based Precautions supplement Standard Precautions for patients with documented or suspected infection or colonization depending on the major mode of microorganism transmission in healthcare settings.
î Contact Precautions are used when microorganisms can be transmitted via direct contact between patients and healthcare personnel or by contact between patients and contaminated objects and/or
environments. In addition to Standard Precautions, the following must be done:
#9632; Assign the patient to a private room if possible. Cohorting of patients with the same organisms is allowed if necessary.
#9632; Wear gown and gloves to enter the room; remove them before leaving the room.
#9632; Use a dedicated stethoscope and thermometer.
#9632; Minimize environmental contamination during patient transport (e.g., patient can be placed in a gown).
î Droplet Precautions are used when microorganisms can be transmitted by respiratory droplets (gt;5 #956;m). Droplets remain suspended in the air for limited periods, and exposure of #8804;3 ft (1 m) is usually required for human-to-human transmission. In addition to Standard Precautions, the following must be done:
#9632; Assign the patient to a private room. The door must be kept closed as much as possible. Rooms with special air handling systems are not required.
#9632; Wear a surgical mask within 6 ft of the patient.
#9632; Limit patient transport and activity outside their room. If transporting the patient outside the room is necessary, the patient must wear a surgical mask.
î Airborne Precautions must be used when microorganisms can be transmitted by respiratory droplet nuclei (lt;5 #956;m). These droplet nuclei remain suspended in the air for extended periods. In addition to Standard Precautions, the following must be done:
#9632; Assign the patient to a negative-pressure airborne infection isolation room. Doors must remain closed.
#9632; Wear a tight-fitting respirator that covers the nose and mouth with a filtering capacity of 95% (e.g., N95 respirator) or powered air-purifying respirator (PAPR) to enter the room. Susceptible individuals should not enter the room of patients with confirmed or suspected measles or chicken pox. An N95 respirator should be fitted to the wearer.
#9632; Limit patient transport and activity outside their room. If transporting the patient outside the room is necessary, the patient must wear a surgical mask. Higher level respiratory protection (e.g., N95 respirator) is not required for the patient.