Central Nervous System Infections Meningitis
GENERAL PRINCIPLES
• Meningitis (inflammation of the meninges) is caused by bacterial, viral, or fungal infections or by noninfectious causes including medications.
• Bacterial meningitis is a medical emergency and requires immediate therapy without delay for diagnostic procedures.
Rapid initiation of antimicrobial treatment decreases mortality.• Streptococcus pneumoniae is the most common bacterial etiology in adults, followed by Neisseria meningitidis, group B Streptococcus, and Haemophilus influenzae. Listeria monocytogenes is more frequent in the elderly and in immunocompromised hosts.
• Health care-associated meningitis (after neurosurgical procedures or head trauma) and intraventricular shunt infections are caused by staphylococci (S. aureus and coagulase-negative staphylococci) and gram-negative bacilli (especially Pseudomonas aeruginosa).
DIAGNOSIS
Clinical Presentation
• Meningitis should be considered in any patient with fever and stiff neck or neurologic symptoms, especially altered mental status.
• Aseptic meningitis (meningitis with negative bacterial cultures) is usually milder and may be preceded by upper respiratory symptoms or pharyngitis. Enteroviruses, and occasionally arboviruses, are the most common cause; drugs such as NSAIDs and TMP-SMX are less common causes.
• Bacterial, viral, and noninfectious etiologies cannot be distinguished clinically.
Diagnostic Testing Diagnosis requires a lumbar puncture (LP) with measurement of opening pressure; cerebrospinal fluid (CSF) protein, glucose, and cell count with differential; and Gram stain with culture (Table 14-3). Blood cultures should also be obtained. Head CT scan before LP is not necessary for immunocompetent patients unless there are focal neurologic abnormalities, seizures, or diminished level of consciousness.6
• In bacterial meningitis, CSF shows a neutrophilic pleocytosis, elevated protein, and low glucose.
In aseptic meningitis, a lymphocytic CSF pleocytosis is common (although neutrophils may predominate early), along with a normal glucose. CSF PCR can detect enteroviruses, herpes simplex virus (HSV), and HIV. CSF lymphocytosis with profoundly decreased glucose level should prompt a workup for tuberculous or fungal meningitis.TABLE 14-3
TYPICAL CEREBROSPINAL FLUID FINDINGS IN MENINGITIS6
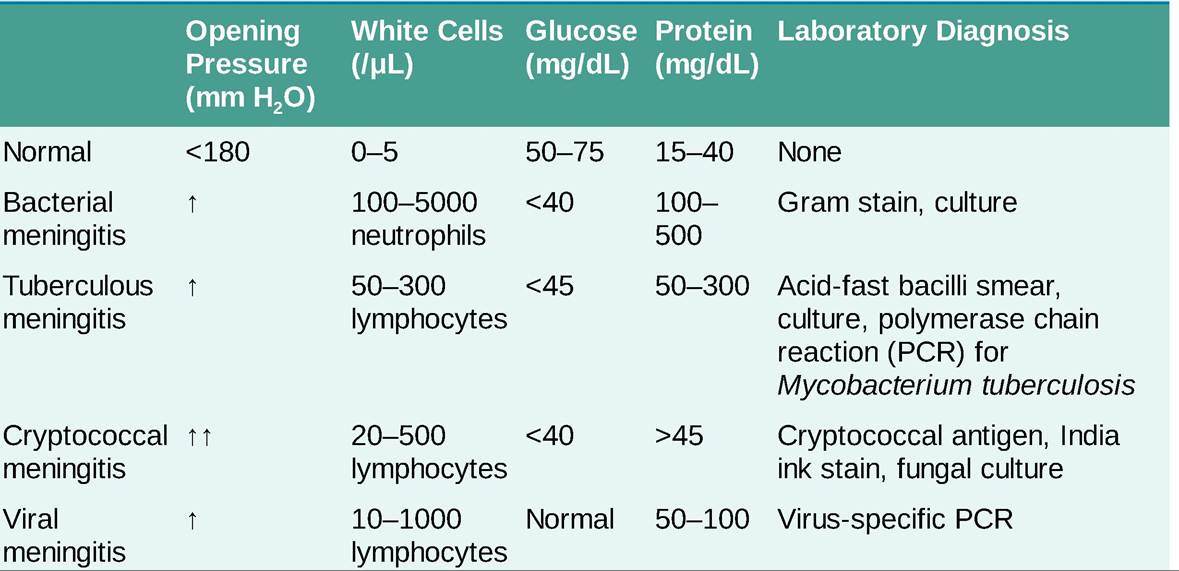
• Depending on the clinical scenario, other useful CSF studies include Venereal Disease Research Laboratory to diagnose neurosyphilis, acid-fast stain and culture, cryptococcal antigen (CrAg) and fungal culture, and arbovirus antibodies.
TREATMENT
• High-dose parenteral antimicrobial therapy should be started immediately after LP. An empiric regimen should be based on patient risk factors and Gram stain of the CSF.
• In patients aged 2-50 years, ceftriaxone 2 g IV q12h or cefotaxime 2 g IV q4-6h and vancomycin 1520 mg/kg IV q8-12h are recommended.
• Ampicillin 2 g IV q4h should be added for patients older than 50 years to cover L. monocytogenes.
• Immunocompromised patients should receive vancomycin plus ampicillin plus cefepime 2 g IV q8h or meropenem 2 g IV q8h.
• In the postneurosurgical setting, after head trauma or for intraventricular shunt infection, vancomycin and ceftazidime 2 g IV q8h or cefepime is indicated.
• Empiric regimens should be narrowed once cultures are known.
• Dexamethasone 0.15 mg/kg IV q6h started just before or with initial antibiotics and continued for 4 days reduces the risk of a poor neurologic outcome in meningitis caused by S. pneumoniae. Glucocorticoids should not be used for other pathogens.
• Therapy for specific infections
î For S. pneumoniae, initial therapy consists of ceftriaxone plus vancomycin. Vancomycin is discontinued if the isolate is susceptible to ceftriaxone (minimum inhibitory concentration [MIC] PCR does not rule it out. Other PCR tests (Ehrlichia, Bartonella, Mycoplasma, varicellazoster virus, cytomegalovirus) are sent if there is clinical suspicion.
• MRI may show temporal lobe enhancement in HSV encephalitis.
TREATMENT
• Acyclovir 10 mg/kg IV q8h should be started on all patients with suspected encephalitis and continued for 14-21 days, until HSV is definitively ruled out. Delayed therapy increases the risk of poor neurologic outcomes.
• Treatment of other viral causes is mainly supportive.
• Antibiotic therapy for presumed bacterial meningitis (see above) should be initiated if clinically indicated and discontinued once CSF cultures are negative. Doxycycline 100 mg q12h should be added if there is suspicion for tick-borne illness.7