Coronary Heart Disease and Stable Angina
GENERAL PRINCIPLES
Definition
• Coronary artery disease (CAD) refers to the luminal narrowing of a coronary artery, usually due to atherosclerosis. CAD is the leading contributor to ischemic heart disease (IHD).
IHD includes angina pectoris, myocardial infarction (MI), and silent myocardial ischemia.• Cardiovascular disease (CVD) includes IHD, cardiomyopathy, heart failure (HF), arrhythmia, hypertension, cerebrovascular accident (CVA), diseases of the aorta, peripheral vascular disease (PVD), valvular heart disease, and congenital heart disease.
• Stable angina is defined as angina symptoms or angina equivalent symptoms that are reproduced by consistent levels of activity and relieved by rest.
• American Heart Association/American College of Cardiology (AHA/ACC) guidelines provide a more thorough overview of stable IHD.1,2
Epidemiology
• The lifetime risk of IHD at age 40 is one in two for men and one in three for women.
• There are more than 15 million Americans with IHD, 50% of whom have chronic angina.
• CVD has become an important cause of death worldwide, accounting for nearly 30% of all deaths and has become increasingly significant in developing nations.3
Etiology
• CAD most commonly results from luminal accumulation of atheromatous plaque.
• Other causes of obstructive CAD include congenital coronary anomalies, myocardial bridging, vasculitis, and prior radiation therapy.
Pathophysiology
• Stable angina results from progressive luminal obstruction of angiographically visible epicardial coronary arteries or, less commonly, obstruction of the microvasculature, which results in a mismatch between myocardial oxygen supply and demand.
• Atherosclerosis is an inflammatory process, initiated by lipid deposition in the arterial intima layer followed by recruitment of inflammatory cells and proliferation of arterial smooth muscle cells to form an atheroma.
î The coronary lesions responsible for stable angina differ from the vulnerable plaques associated with acute MI. The stable angina lesion is fixed and is less prone to fissuring, hence producing symptoms that are more predictable.4
î All coronary lesions are eccentric and do not uniformly alter the inner circumference of the artery.
î Epicardial coronary lesions causing less than 40% luminal narrowing generally do not significantly impair coronary flow.
î Moderate angiographic lesions (40%-70% obstruction) may interfere with flow and are routinely underestimated on coronary angiograms given the eccentricity of CAD.
Risk Factors
• Of IHD events, >90% can be attributed to elevations in at least one major risk factor.5
• Assessment of traditional CVD risk factors includes:
î Age
î Blood pressure (BP)
î Blood glucose (Note: Diabetes is considered an IHD risk equivalent.)
î Lipid profile (low-density lipoprotein [LDL], high-density lipoprotein [HDL], triglycerides); direct LDL for nonfasting samples or very high triglycerides
î Tobacco use (Note: Smoking cessation restores the risk of IHD to that of a nonsmoker within approximately 15 years.)6
î Family history of premature CAD: Defined as first-degree male relative with IHD before age 55 years or female relative before age 65 years
° Measures for obesity, particularly central obesity; body mass index goal is between 18.5 and 24.9 kg/m2; waist circumference goal is done either with or without an imaging modality.
° Many stress testing modalities provide not only detection of ischemia/CAD but also prognostic information based on the burden of ischemia.
î Table 4-5 provides an overview of the sensitivity and specificity for each stress and imaging modality along with advantages and disadvantages for the clinician to consider.
TABLE 4-5
DIAGNOSTIC ACCURACY OF COMMON STRESS TESTING MODALITIES IN PATIENTS WITHOUT KNOWN ISCHEMIC HEART DISEASE
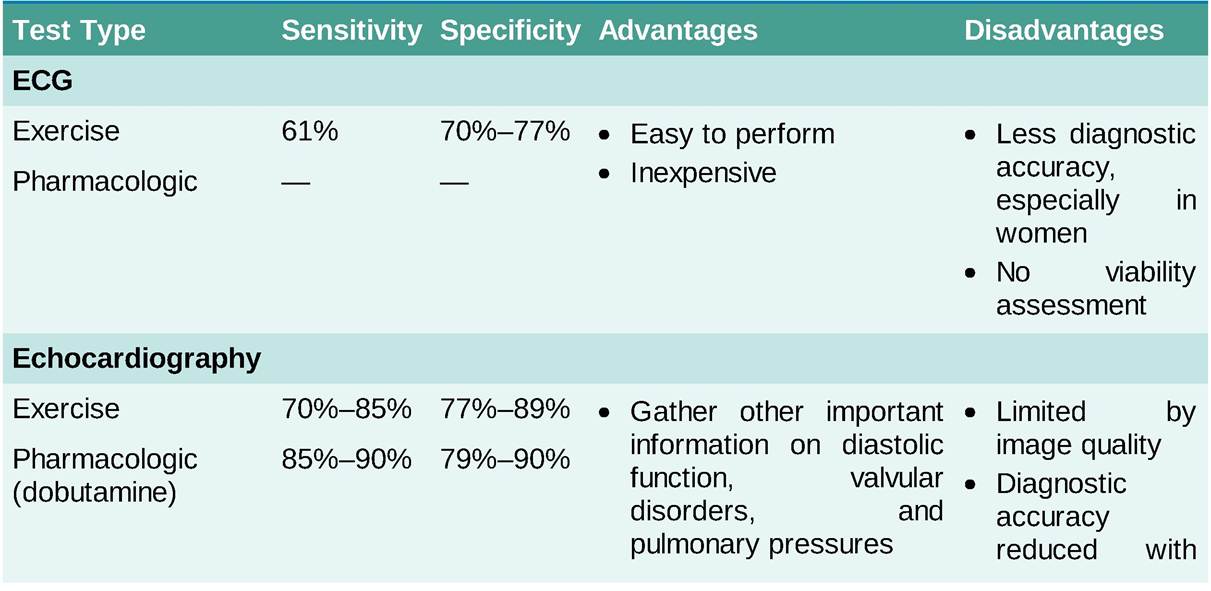
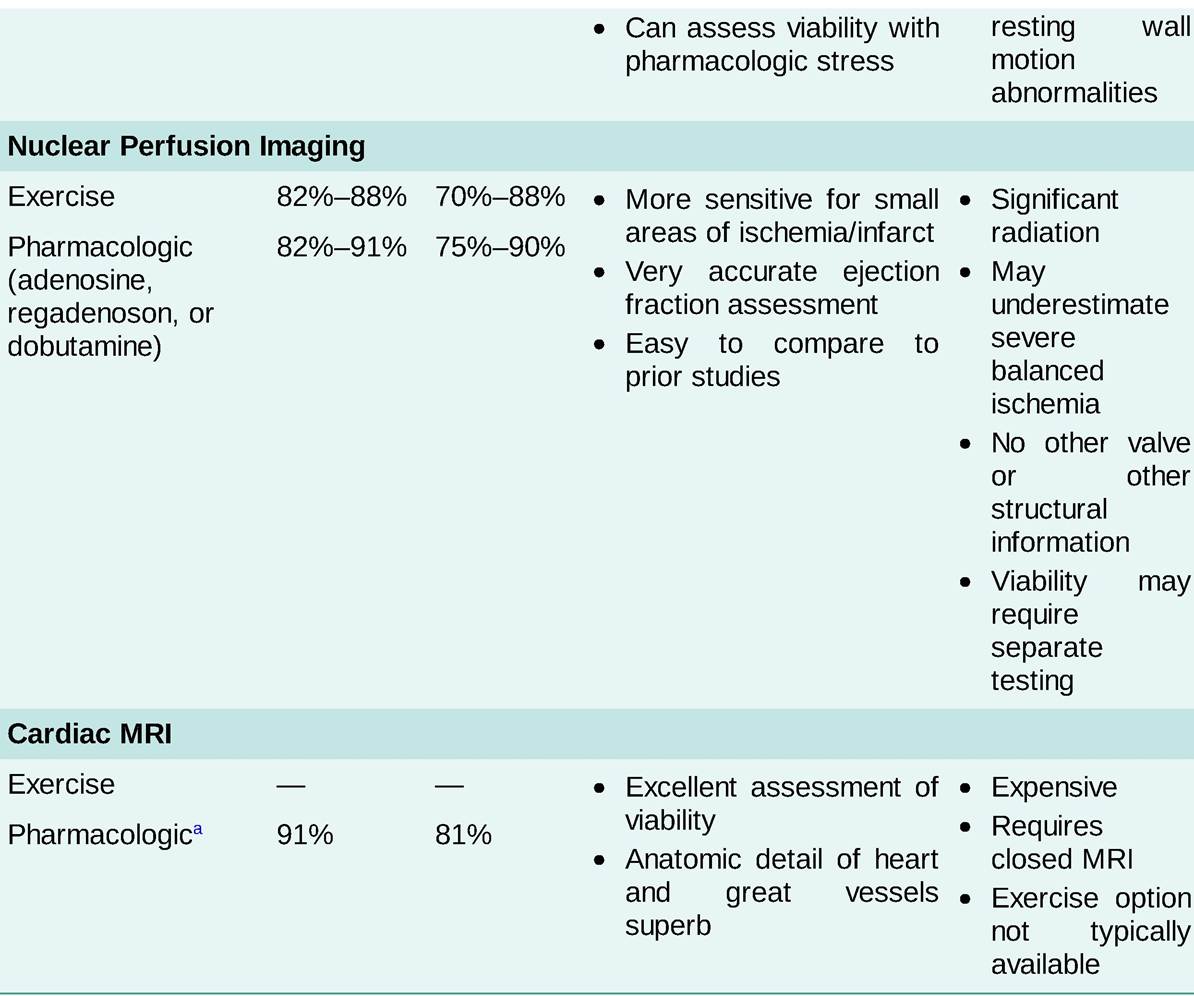
All diagnostic accuracies unadjusted for referral bias.1,2 aVasodilator stress only; dobutamine has sensitivity of 83% and specificity of 86%.
• Stress testing indications
î See the ACCF 2013 Multimodality Appropriate Use Criteria for the Detection and Risk Assessment of Stable Ischemic Heart Disease10 for a comprehensive list of the indications for stress testing.
î The following are some of the more common indications:
■ Patients without known CAD:
? Patients with anginal symptoms who are intermediate risk
? Asymptomatic intermediate-risk patients who plan on beginning a vigorous exercise program or working in a high-risk occupation (e.g., airline pilot)
? Atypical symptoms in patients with a high risk of IHD (i.e., diabetes or vascular disease patients)
■ Patients with known CAD:
? Post-MI risk stratification (see section on ST-segment elevation MI)
? Preoperative risk assessment if it will change management prior to surgery
? Recurrent anginal symptoms despite medical therapy or revascularization
• Contraindications to stress testing
î Acute MI within 2 days
î Unstable angina not previously stabilized by medical therapy
î Cardiac arrhythmias causing symptoms or hemodynamic compromise
î Symptomatic severe aortic stenosis
î Symptomatic HF
î Acute pulmonary embolus, myocarditis, pericarditis, or aortic dissection
• Stress modalities
î Exercise stress testing
■ The stress modality of choice for evaluating most patients of intermediate risk for CAD (see Table 4-2).
■ Bruce protocol: Consists of 3-minute stages of increasing treadmill speed and incline. BP, heart rate, and ECG are monitored throughout the study and the recovery period.
■ The ECG portion of the study is considered positive if:
? New ST-segment depressions of >1 mm in multiple contiguous leads
? Hypotensive response to exercise
? Sustained ventricular arrhythmias are precipitated by exercise
■ The Duke Treadmill Score provides prognostic information for patients presenting with chronic angina (Table 4-6).
TABLE 4-6
EXERCISE STRESS TESTING: DUKE TREADMILL SCORE11
Duke Treadmill Score (DTS) = Minutes exercised - [5 ? maximum ST-segment deviation] - [4 ? angina score].
Angina score: 0 = none, 1 = not test limiting, 2 = test limiting| DTS | ||
| 5 | Annual mortality 0.25% | Low-risk study |
| -10 to 4 | Annual mortality 1.25% | Intermediate-risk study |
| 5% | High-risk study | |
In general, β-blockers, other nodal blocking agents, and nitrates should be discontinued prior to stress testing.11
■ When exercise testing is combined with imaging (e.g., echocardiography), and the test is normal at the target heart rate for age, the risk of infarction or death from CVD is Signs or symptoms of HF or decreased LV function
■ Angina that is inadequately controlled with medical therapy for the patient's lifestyle
■ Previous coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI)
■ Suspected or known left main (≥50% stenosis) or severe three-vessel CAD
■ To diagnose CAD in patients with angina who have not undergone stress testing due to a high pretest probability of having CAD (see Table 4-2)
î Can be used to evaluate patients who are suspected of having a nonatherosclerotic cause of ischemia (e.g., coronary anomaly, coronary dissection, radiation vasculopathy).
î Functional significance of intermediate stenotic lesions (50%-70% narrowing) can further be assessed by fractional flow reserve (FFR) or instantaneous wave-free ratio (iFR).
■ Both FFR and iFR are calculated by determining the ratio of pressure distal to the coronary obstruction to that of the aortic pressure (flow) using slightly different methods.
? An FFR ≤ 0.8 or iFR ≤ 0.89 is considered flow limiting, and PCI decreases the need for urgent revascularization for UA or MI, as well as risk of recurrent MI.12
? Whether PCI in stable IHD improves cardiovascular outcomes or symptoms compared to medical therapy is controversial.13
An early invasive strategy did not reduce death, death from cardiovascular causes, MI, or a composite of the three in stable IHD.14 These patients did have decreased angina and improved quality of life.
Patients with recent acute coronary syndrome (ACS), severe angina, left main disease, or left ventricular ejection fraction (LVEF) < 35% were excluded.
Physiological studies (FFR) were performed in only 20% of cases, and use of intravascular imaging (intravascular ultrasound, optical coherence tomography) was not reported.
♦ The use of physiological studies and intravascular imaging is associated with better outcomes in PCI.15,16
21% of patients assigned to a conservative strategy eventually underwent revascularization.
PCI for stable IHD did not improve survival, but was associated with decreased nonprocedural MI, unstable angina, and angina in a meta-analysis. However, there was an increased incidence of procedural MI.17
î Measurement of LV filling pressures (diastolic function) and aortic and mitral valve gradients, assessment of regional wall motion and LV function, and assessment for certain aortopathies can be accomplished by placing a catheter in the LV cavity or aorta directly and making the appropriate pressure measurements and/or injection of contrast.
î Contrast-induced nephropathy (CIN) occurs after 24-48 hours in up to 5% of patients undergoing coronary angiography. In most patients, creatinine returns to baseline within 7 days.18 The following are considerations in the prevention of CIN:
■ The volume of contrast media used should be minimized.
■ All patients should receive some CIN prophylactic therapy: oral hydration, IV hydration, held IV diuretics, and statin therapy have proven benefit.
■ We recommend a 3 mL/kg bolus of normal saline at least 6 hours prior to the procedure with a 1 mL/kg continuous infusion rate until procedure start.
■ A-Acetyl-l-cysteine has no advantage over simple hydration for prevention of CIN.
• Coronary CT angiography
° A noninvasive technique used to establish a diagnosis of CAD. Like cardiac angiography, it exposes the patient to both radiation and contrast material.
î Uses arterial phase contrast CT images to evaluate coronary stenosis. Where available, a proprietary
software package can calculate intracoronary hemodynamics akin to FFR.
î CT has a high negative predictive value, so it is better suited to rule out disease for symptomatic patients with a low pretest probability for CAD, such as a patient with repeated emergency room admissions for chest pain or patients with equivocal stress test results.
■ The 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain gives CT a class I indication for use in intermediate risk patients with acute chest pain, without known CAD, to exclude obstructive CAD.19
î May assist in identification of congenital anomalies of the coronary arteries.
î Due to diminished study quality, it is not useful in patients with extensive coronary calcification (e.g., elderly, or advanced CKD), coronary stents, or small-caliber vessels.
TREATMENT
• The major goal of treatment is to reduce symptoms.
• An absolute reduction in incidence of MI or cardiac death in patients with stable IHD is accomplished mainly through medical therapy and not revascularization.
• A combination of lifestyle modification, medical therapy, and coronary revascularization can be used. A recommended strategy for the evaluation and management of the patient with stable angina can be found in Figure 4-1.
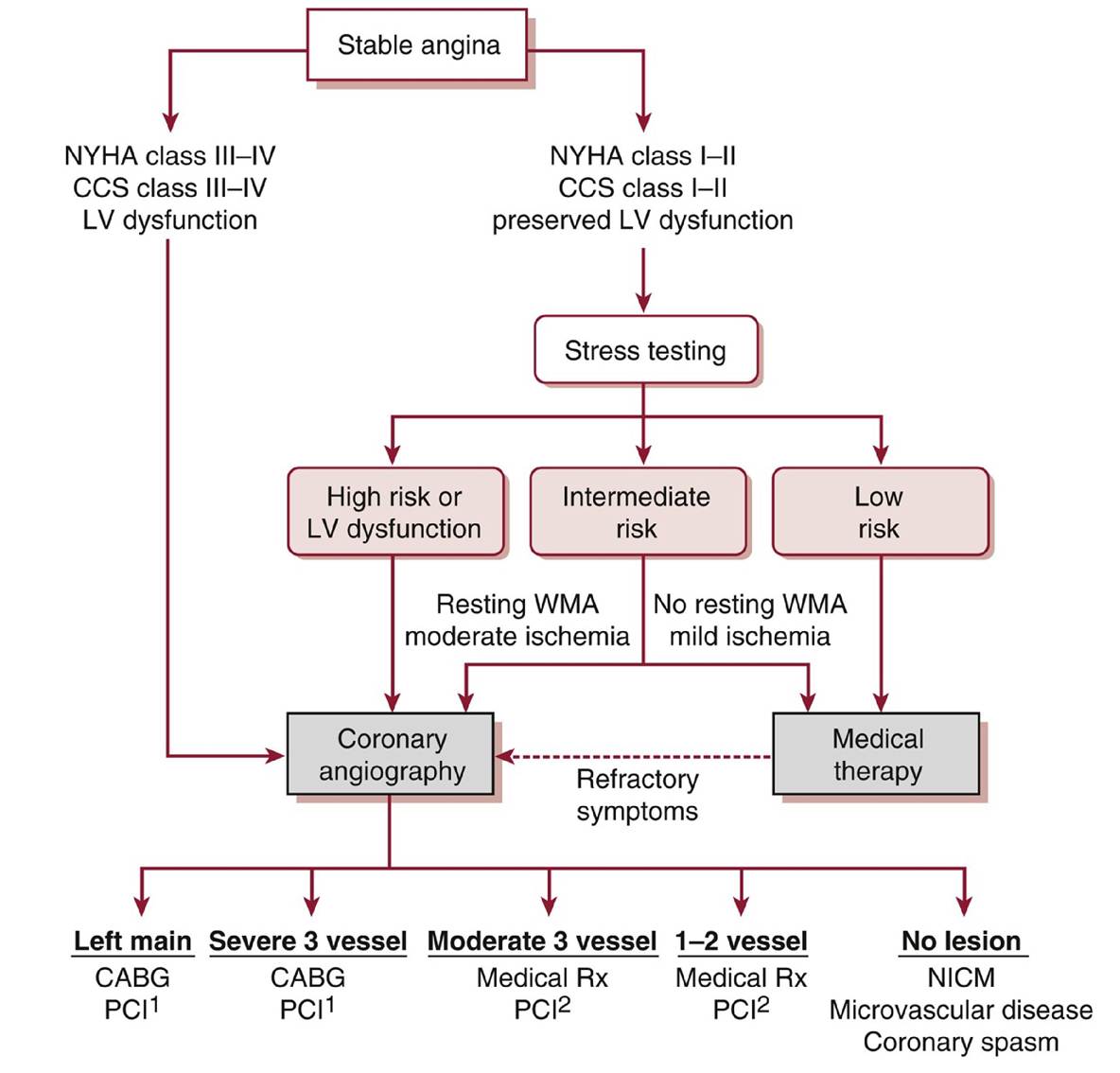
Figure 4-1 Approach to the evaluation and management of the patient with stable ischemic heart disease based on the ISCHEMIA trial,Qf note, patients with severe limiting angina, clinical heart failure, or left ventricle (LV) dysfunction should proceed directly to coronary angiography to define underlying coronary artery disease. Patients without these features may first undergo medical optimization with guideline-directed medical therapies (GDMT). If the patient is satisfied with their symptoms on optimal GDMT and is tolerating treatment without significant side effects, coronary CTA should then be obtained to rule out significant left main disease. If no significant left main disease is present, the patient may continue medical therapy without further testing or intervention. If significant left main disease is present, the patient should undergo cardiac catheterization. P atients who are not satisfied with the outcome of optimal GDMT may proceed directly to cardiac catheterization. Information obtained from cardiac catheterization should then be used by a multidisciplinary team to determine whether continued medical therapy, PCI, or CABG should be pursued. 1CABG generally preferred due to known survival advantage over medical therapy alone; however, if the coronary lesions are not complex, PCI may offer similar results to CABG but with a higher need for future revascularizations. 2PCI should be reserved for patients who have high-grade lesions, have severe ischemia, and are refractory to medical therapy. CABG, coronary artery bypass grafting; CCS, Canadian Cardiovascular Society Classification (angina);
CTA, computed tomography angiography; NICM, nonischemic cardiomyopathy; NYHA, New York Heart Association; PCI, percutaneous coronary intervention; WMA, wall motion abnormality.
• Medical treatment is aimed at improving myocardial oxygen supply, reducing myocardial oxygen demand, controlling exacerbating factors (e.g., anemia), and limiting the development of further atherosclerotic disease.
• Medical treatment often is sufficient to control anginal symptoms in chronic stable angina.
Medications
• Anti-ischemic therapy
î β-Adrenergic antagonists (Table 4-7) control anginal symptoms by decreasing heart rate and myocardial work, leading to reduced myocardial oxygen demand.
■ β-Blockers with intrinsic sympathomimetic activity should be avoided.
■ Dosage can be adjusted to result in a resting heart rate of 50-60 bpm.
■ Use with caution or avoid in patients with active bronchospasm, atrioventricular (AV) block, resting bradycardia, or poorly compensated HF.
î Calcium channel blockers can be used either in conjunction with or in lieu of β-blockers in the presence of contraindications or adverse effects as a second-line agent (Table 4-8).
■ Calcium antagonists are often used in conjunction with β-blockers if the latter are not fully effective at relieving anginal symptoms. Both long-acting dihydropyridines and nondihydropyridine agents can be used.
■ Calcium channel blockers are effective agents for the treatment of coronary vasospasm.
■ Nondihydropyridine agents (verapamil/diltiazem) should be avoided in patients with systolic dysfunction due to their negative inotropic effects.
î Nitrates, either long-acting formulations for chronic use or sublingual/topical preparations for acute anginal symptoms, are more often used as adjunctive antianginal agents (Table 4-9).
■ Sublingual preparations should be used at the first indication of angina or prophylactically before engaging in activities that are known to precipitate angina. Patients should seek prompt medical attention if angina occurs at rest or fails to respond to the third sublingual dose.
■ Nitrate tolerance resulting in reduced therapeutic response may occur with all nitrate preparations. The institution of a nitrate-free period of 10-12 hours (usually at night) can enhance treatment efficacy.
■ For patients with CAD, nitrates have not shown a mortality benefit.
■ Nitrates are contraindicated (even in patients with ACS) for use in patients who are on phoshodiesterase-5 inhibitors due to risk of severe hypotension. A washout period of 24 hours for sildenafil and vardenafil and 48 hours for tadalafil is required prior to nitrate use.
î Ranolazine is indicated for angina refractory to standard medical therapy and has shown benefit in improving symptoms and quality of life. Ranolazine interacts with simvastatin metabolism and should not be used together.
• Secondary prevention medications
î Acetylsalicylic acid (ASA) (75-162 mg/d) reduces cardiovascular events, including repeat revascularization, MI, and cardiac death, by approximately 33%.20
■ ASA 81 mg appears to be sufficient for most patients.
■ ASA desensitization may be performed in patients with ASA allergy.
■ Clopidogrel (75 mg/d) can be used in those allergic or intolerant of ASA.
î Angiotensin-converting enzyme inhibitors (ACE inhibitors) and angiotensin receptor blockers (ARBs) have cardiovascular protective effects that reduce the recurrence of ischemic events.
■ ACE inhibitor therapy, or ARBs in those with ACE inhibitors intolerance, should be used in all patients with an LVEF 70 mg/dL despite high-intensity statins. Currently, expense and insurance coverage limit the use of this class of medications.21
î Ezetimibe also improves cardiovascular outcomes among patients with IHD whose LDL remains >100 mg/dL despite high-intensity statin therapy.22
î Influenza vaccination is recommended for all patients with IHD.
TABLE 4-7
Β-BLOCKERS COMMONLY USED FOR ISCHEMIC HEART DISEASE
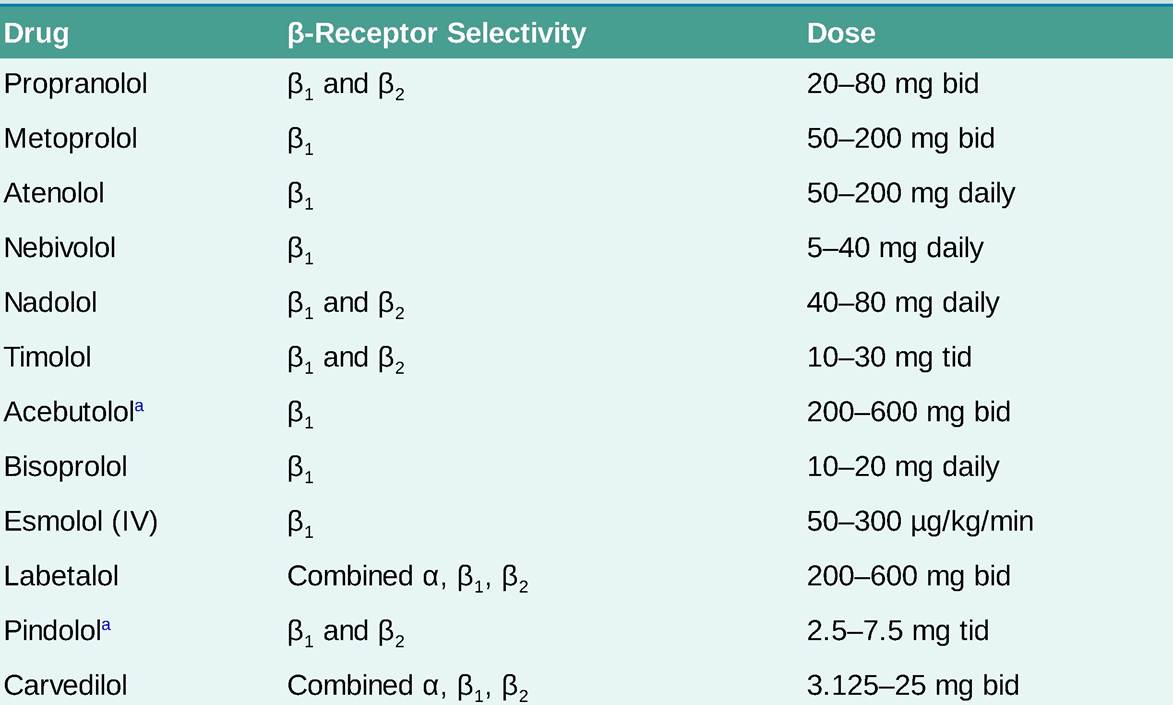
aβ-Blockers with intrinsic sympathomimetic activity.
TABLE 4-8
CALCIUM CHANNEL BLOCKERS COMMONLY USED FOR ISCHEMIC HEART DISEASE

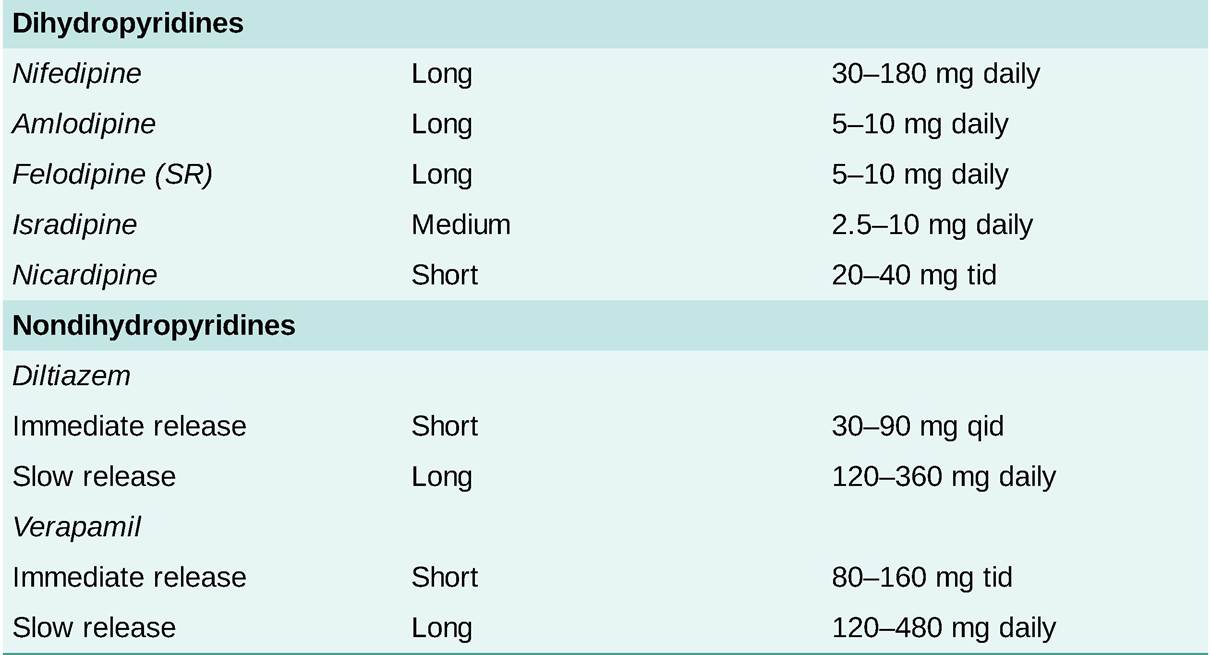
TABLE 4-9
NITRATE PREPARATIONS COMMONLY USED FOR ISCHEMIC HEART DISEASE
| Preparation | Dosage | Onset (min) | Duration |
| Sublingual nitroglycerin | 0.3-0.6 mg PRN | 2-5 | 10-30 min |
| Aerosol nitroglycerin | 0.4 mg PRN | 2-5 | 10-30 min |
| Oral isosorbide dinitrate | 5-40 mg tid | 30-60 | 4-6 h |
| Oral isosorbide mononitrate | 10-20 mg bid | 30-60 | 6-8 h |
| Oral isosorbide mononitrate SR | 30-120 mg daily | 30-60 | 12-18 h |
| 2% Nitroglycerin ointment | 0.5-2 in tid | 20-60 | 3-8 h |
| Transdermal nitroglycerin patches | 5-15 mg daily | >60 | 12 h |
| Intravenous nitroglycerin | 10-200 μg∕min | 50% left main CAD that has not been grafted (unprotected). PCI is a reasonable alternative for patients with left main disease if the patient is a poor surgical candidate (STS score > 5) and has a favorable morphology for PCI (low Syntax Score). PCI, in the right clinical context, can offer rates of MI, CVA, or death similar to CABG.25 ■ CABG for three-vessel disease or two-vessel disease that includes the proximal left anterior descending (LAD) artery. ■ CABG for patients with two-vessel disease, not including the LAD artery, if there is extensive ischemia (>20% myocardium at risk) or in patients with isolated proximal LAD artery disease when an internal mammary artery revascularization is performed. ■ CABG, as compared to PCI or medical therapy, in patients with multivessel disease and diabetes, if a left internal mammary artery to the LAD artery can be placed.26 PCI may offer similar survival outcomes in diabetics with multivessel disease and a low Syntax Score (in patients with recurrent angina after CABG. î The use of internal mammary artery grafts is associated with 90% graft patency at 10 years, compared with 40%-50% for saphenous vein grafts. The long-term patency of a radial artery graft is 80% at 5 years. After 10 years of follow-up, 50% of patients develop recurrent angina or other adverse cardiac events related to late vein graft failure or progression of native CAD. î The risks of elective PCI include 20 minutes), new-onset angina, and progressive angina (previously diagnosed angina that has become more frequent, lasts longer, or occurs with less exertion). New-onset and progressive angina should occur with at least mild to moderate activity, CCS class III severity. ° Female sex, diabetes, HF, end-stage kidney disease, and older age are traits that have been associated with a greater likelihood of atypical ACS symptoms. However, the most common presentation in these populations is still typical anginal chest pain. î Jaw, neck, arm, back, or epigastric pain and/or dyspnea can be anginal equivalents. î Pleuritic pain, pain that radiates down the legs or originates in the mid/lower abdomen, pain that can be reproduced by extremity movement or palpation, and pain that lasts seconds in duration are unlikely to be related to ACS. PHYSICAL EXAMINATION • Physical examination should be directed at identifying hemodynamic instability, pulmonary congestion, and other causes of acute chest discomfort. • Objective evidence of HF, including peripheral hypoperfusion, heart murmur (particularly mitral regurgitation [MR] murmur), elevated jugular venous pulsation, pulmonary edema, hypotension, and peripheral edema worsen the prognosis. • Killip classification can be useful to risk stratify and identify patients with features of cardiogenic shock (Table 4-10). TABLE 4-10 KILLIP CLASSIFICATION33
JVD, jugular venous distention; SBP, systolic blood pressure. aIn-hospital mortality of patients in 1965-1967 with no reperfusion therapy (n = 250).33 • Examination may also give clues to other causes of ischemia such as thyrotoxicosis or aortic dissection (see Table 4-4). Diagnostic Testing ELECTROCARDIOGRAPHY • Prior to or immediately on arrival to the emergency department, a baseline ECG should be obtained in all patients with suspected ACS. A normal tracing does not exclude the presence of disease. • The presence of Q waves, ST-segment changes, or T-wave inversions is suggestive of CAD. • Isolated Q waves in lead III only are a normal finding. • Serial ECGs should be obtained to assess for dynamic ischemic changes. • Comparison to prior ECGs is important when evaluating an ECG for dynamic changes. • The posterior circulation (i.e., circumflex coronary artery distribution) is poorly assessed with standard ECG lead pl acement and should always be considered when evaluating patients with ACS. Posterior leads or urgent echocardiography may more accurately assess the presence of ischemia when the suspicion is high. • Approximately 50% of patients with UA/NSTEMI have significant ECG abnormalities, including transient ST-segment elevations, ST depressions, and T-wave inversions.32,34 î ST-segment depression in two contiguous leads is a sensitive indicator of myocardial ischemia, especially if dynamic and associated with symptoms. ■ Threshold value for abnormal J-point depression should be 0.5 mm in leads V2 and V3 and 1 mm in all other leads. ■ ST-segment depression in multiple leads plus ST-segment elevation in aVR and/or V1 suggests ischemia due to multivessel or left main disease. î Biphasic or deeply inverted T waves (>5 mm) with QT prolongation in leads V2 to V4 in the setting of stuttering chest pain within the past 24 hours suggests a critical lesion in the LAD artery distribution (Wellens syndrome).34 î Nonspecific ST-segment changes or T-wave inversions (those that do not meet voltage criteria) are nondiagnostic and unhelpful in management of acute ischemia but are associated with a higher risk for future cardiac events. LABORATORIES • A complete blood count, basic metabolic panel, fasting glucose, and lipid profile should be obtained in all patients with suspected CAD. Other conditions may be found to be contributing to ischemia (e.g., anemia) or mimicking ischemia (e.g., hyperkalemia-related ECG changes) or may alter management (e.g., severe thrombocytopenia). • Troponin is the recommended biomarker for assessment of myocardial necrosis. î Troponin T and I assays are highly specific and sensitive markers of myocardial necrosis. Serum troponin levels are usually undetectable in normal individuals, and any elevation is considered abnormal. î In patients with troponin below the detectable limit of the assay within 6 hours of the onset of pain, a second sample should be drawn 8-12 hours after symptom onset. î MI size and prognosis are directly proportional to magnitude of increase in troponin.34 • Creatine kinase (CK)-MB is no longer a recommended marker for the initial diagnosis of NSTEMI. It lacks specificity because it is present in both skeletal and cardiac muscle cells. î CK-MB may be a useful assay for detecting postinfarct ischemia because a fall and subsequent rise in enzyme levels suggests reinfarction if accompanied by recurrent ischemic symptoms or ECG changes. • Brain natriuretic peptide (BNP) can be a useful biomarker of myocardial stress in patients with ACS, and elevations are associated with worse outcomes.35 Severe elevations of BNP in the setting of ACS in patients without known HF should raise concern for a large infarction and urgent angiography. TREATMENT • Acute treatment aims to reduce the symptoms of chest pain and risk of recurrent MI or death. • Risk stratification can be helpful in determining the appropriate testing, pharmacologic interventions, and timing or need for coronary angiography. î Risk of death or MI progression is elevated with the following high-risk ACS characteristics, which should prompt urgent coronary angiography (myocardial infarction; PCI, percutaneous coronary intervention; TIMI, Thrombolysis in Myocardial Infarction; UA, unstable angina; VF, ventricular fibrillation; VT, ventricular tachycardia. î In ACS, as opposed to stable IHD, a routine invasive approach with possible PCI has been shown to reduce the incidence of recurrent MI, hospitalizations, and death. In general, patients with ACS should undergo a routine invasive strategy unless it is clear that the risk outweighs the possible benefit in a given patient. î In the ischemia-driven approach, if the patient does not develop high-risk ACS features, has normal subsequent cardiac biomarkers, has no dynamic ECG changes, and responds to medical therapy, a noninvasive stress test should be obtained for further risk stratification. ■ Patients should be angina free for at least 12 hours prior to stress testing. ■ If a patient with positive cardiac biomarkers is selected for noninvasive testing, a submaximal or pharmacologic stress test 72 hours after the peak value may be performed. ■ Coronary angiography is reserved for patients who develop high-risk ACS features, have a high- risk stress test, develop angina at low levels of stress, or are noted to have an LVEF < 40%. î In the routine invasive strategy, the patient is planned for a coronary angiography with intent to revascularize. An early (is a prodrug whose metabolite blocks the P2Y12 receptor and inhibits platelet activation and aggregation by blocking the adenosine diphosphate receptor site on platelets. ■ The addition of clopidogrel to ASA reduced cardiovascular mortality and recurrent MI both acutely and at 11 months of follow-up.39 ■ A loading dose of 600 mg should always be given in naive patients. ■ In patients unable to take oral medications or unable to absorb oral medications due to ileus, rectal administration is unproven but has been reported. Alternatively, parenteral agents (e.g., cangrelor or eptifibatide) may be considered. ■ Can be used as part of the protocol in both the ischemia-driven and routinely invasive strategies. ° Prasugrel is also a prodrug that blocks the P2Y12 adenosine receptor; its conversion to its active metabolite occurs faster and to a greater extent than clopidogrel. ■ Results in faster, greater, and more uniform platelet inhibition compared to clopidogrel at the expense of higher risk of bleeding.55 ■ It decreases risk of CVD death, MI, CVA, and acute stent thrombosis as compared to clopidogrel in ACS patients, including STEMI patients. ■ It should be used with caution or avoided in patients older than 75 years and who weigh less than 60 kg. It is contraindicated in those with prior stroke or transient ischemic attack (TIA). ■ Used only in the invasive approach of ACS and only after coronary anatomy is known and PCI is planned. There is no benefit over clopidogrel when tested before initiation of PCI. ■ Prasugrel may be superior to ticagrelor with regards to the composite of MI, stroke, and death.56 î Ticagrelor is not a prodrug and blocks the P2Y12 adenosine receptor directly. ■ Reduces the risk of death, MI, CVA, and stent thrombosis as compared to clopidogrel in ACS patients, including STEMI patients.42 ■ After the loading dose of ASA, the maintenance dose of ASA must be of LMWH with possibly reduced bleeding rates.66 | |
| Bivalirudinb | 0.75 mg/kg IV bolus, 1.75 mg/kg/h | When used in conjunction with ASA and clopidogrel, bivalirudin is at least as effective as the combination of ASA, UFH, clopidogrel, and GPIIb/IIIa antagonists with decreased bleeding rates.67 May increase risk for stent thrombosis. Monitoring is required with a goal aPTT of 1.5-2.5 times control. |


aPTT, activated partial thromboplastin time; ASA, aspirin; GFR, glomerular filtration rate; GP, glycoprotein; LMWH, low- molecular-weight heparin; MI, myocardial infarction; UFH, unfractionated heparin.
aLMWH should be given at reduced dose (50%) in patients with a serum creatinine >2 mg/dL or GFR < 30 mL/min.
bBivalirudin requires dosage adjustment in patients with a GFR less than 30 mL/min or those on hemodialysis.
î Anticoagulation accompanied by DAPT is required for all UA/NSTEMI patients, whether along the early invasive or conservative pathway.
î Unfractionated heparin (UFH) works by binding antithrombin III, which catalyzes the inactivation of thrombin and other clotting factors.
■ Most commonly used and easily monitored but also most inconsistent in its anticoagulation and metabolism.
■ Heparin-induced thrombocytopenia (HIT) is a concern with prior use.
■ Easily reversed in the event of a severe hemorrhagic complication.
■ Always requires aggressive bolus dosing and anticoagulation monitoring in the setting of ACS.
■ Recommended anticoagulant to be used in the setting of ACS.
î Low-mole cular-weight heparin (LMWH) inhibits mostly factor Xa but also affects thrombin activity and offers an ease of administration (weight-based, twice-daily subcutaneous dose). The risk of HIT is lower but not absent.
■ As compared to UFH, LMWH has a more predictable anticoagulant effect.
■ It has a similar efficacy as UFH but is associated with a higher risk of postprocedural bleeding.68
■ LMWH must be adjusted for renal dysfunction and should be avoided in patients with severe impairments.
■ Enoxaparin 0.3 mg/kg IV should be administered at the time of PCI in patients who have received less than two therapeutic doses or if the last dose was received more than 8 hours before PCI.
î Fondaparinux is a synthetic polysaccharide that selectively inhibits factor X and can be subcutaneously administered on a daily routine.
■ Associated with an increased risk of thrombosis during PCI and should not be used without additional antithrombin anticoagulation; as such, it is not recommended for the routine management of ACS.
■ In patients not undergoing invasive management, fondaparinux may significantly reduce bleeding and improve outcomes compared to LMWH.69
î Bivalirudin is a direct thrombin inhibitor given as a continuous IV infusion and requires partial thromboplastin time (PTT) monitoring when used for >4 hours.
■ It does not cause HIT and is used in the treatment of patients who develop HIT or patients with ACS who have history of HIT.
■ Bivalirudin can be given in conjunction with ASA and clopidogrel in patients presenting with UA/NSTEMI who will undergo a routine invasive strategy.
■ Bivalirudin alone compared to UFH/LMWH + GPIIb/IIIa inhibitor was associated with less bleeding.70
■ Recent evidence has shown that in ACS without significant GPIIb/IIIa inhibitor use, bivalirudin is associated with increased risk of stent thrombosis and target lesion revascularization.71
■ Caution should be used with routine use of bivalirudin in ACS unless there is a high risk of bleeding.
• Anti-ischemic therapy (please also refer to Treatment section of stable angina)
î Nitroglycerin
■ Treatment can be initiated at the time of presentation with sublingual nitroglycerin. NOTE: 40% of patients with chest pain not due to CAD will get relief with nitroglycerin62 (see Table 4-9).
■ Patients with ongoing ischemic symptoms or those who require additional agents to control significant hypertension can be treated with IV nitroglycerin until pain relief, hypertension control, or both are achieved.
■ Rule out right ventricular (RV) infarct prior to administration of nitrates because this can precipitate profound hypotension.
î β-Adrenergic blockers (BBs) (please also refer to the Treatment section for stable angina)
■ Oral therapy should be started early in the absence of contraindications.
■ Treatment with an IV preparation should be reserved for treatment of arrhythmia, ongoing chest pain, or advanced hypertension rather than routine use.
■ Routine use of IV BBs is associated with increased risk of cardiogenic shock and should be avoided.
■ Contraindications to BB therapy include advanced AV block, active bronchospasm, decompensated HF, cardiogenic shock, hypotension, and bradycardia.
î Morphine 2-4 mg IV may be used as an adjunct to BB, nitrates, and calcium channel blockers. Care must be used not to mask further clinical evaluation by heavy use of narcotic medications.
• Adjunctive medical therapy
î ACE inhibitors (refer to Treatment section for stable angina) are effective antihypertensive agents and have been shown to reduce mortality in patients with CAD and LV systolic dysfunction. ACE inhibitors should be used in patients with LV dysfunction (EF < 40%), hypertension, or diabetes presenting with ACS. ARBs are appropriate in patients who cannot tolerate ACE inhibitors.
î Aldosterone antagonists should be added, if there are no contraindications (potassium > 5 mEq/L or creatinine clearance [CrCl] < 30 mL/min), after initiation of ACE inhibitors to patients with diabetes or an LVEF < 40%.
î 3-Hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA) reductase inhibitors (statins) are potent lipid-lowering agents that reduce the incidence of ischemia, MI, and death in patients with CAD. High-intensity statins should be routinely administered within 24 hours of presentation in patients presenting with ACS. A lipid profile should be obtained in all patients.
■ Aggressive statin therapy reduces the risk of recurrent ischemia, MI, and death in patients presenting with ACS.62
■ A reduction in adverse CVD outcomes following early initiation of a high-dose statin with achievement of an LDL < 70 mg/dL can be seen as early as 30 days following initial presentation with ACS.72 Aggressive LDL lowering also reduces the incidence of periprocedural MI following PCI.67’73
î NSAIDs are associated with an increased risk of death, MI, myocardial rupture, hypertension, and HF in large meta-analyses.74 Adverse outcomes have been observed for both nonselective and selective cyclooxygenase-2 (COX-2) agents. NSAIDs should be discontinued in patients presenting with UA/NSTEMI.
î Blood glucose should not be tightly controlled in diabetic patients who have suffered ACS because it may increase mortality. Goal is prior to the induction of anesthesia.
Monitoring/Follow-Up
The highest rate of progression to MI or development of recurrent MI is in the first 2 months after presentation with the index episode. Beyond that time, most patients have a clinical course similar to those with chronic stable angina.
• Patients should be discharged on dual antiplatelet, BB, and statin therapy.
• Most patients should be discharged on ACE inhibitors.
• Patients should be evaluated for the need of aldosterone antagonists.
• Screen for life stressors and depression. Refer for depression treatment as needed.
• Smoking cessation and risk factor modification should be stressed.
• Referral to cardiac rehabilitation should also be pursued.