ST-Segment Elevation Myocardial Infarction
GENERAL PRINCIPLES
Definition
Ģ STEMI is defined as a clinical syndrome of myocardial ischemia in association with persistent ECG ST elevations (see ōDiagnostic Testingö section).
Ģ STEMI is a medical emergency.
Ģ Compared to UA/NSTEMI, STEMI is associated with a higher in-hospital and 30-day morbidity and mortality. Left untreated, the mortality rate of STEMI can exceed 30%, and the presence of mechanical complications (papillary muscle rupture, ventricular septal defect [VSD], and free wall rupture) increases the mortality rate to 90%.
Ģ Ventricular fibrillation (VF) accounts for approximately 50% of mortality and often occurs within the first hour from symptom onset.
Ģ Keys to treatment of STEMI include rapid recognition and diagnosis, coordinated mobilization of health care resources, and prompt reperfusion therapy.
Ģ Mortality is directly related to total ischemia time.
Ģ AHA/ACC guidelines provide a more thorough overview of STEMI.75
Epidemiology
Ģ STEMI accounts for approximately 25%-30% of ACS cases annually, and the incidence has been declining.
Ģ Over the last several decades, there has been a dramatic improvement in short-term mortality to the current rate of 6%-10%.
Ģ Approximately 30% of STEMI presentations occur in women, but outcomes and complications continue to be worse compared with male counterparts.
Pathophysiology
Ģ STEMI is caused by acute, total occlusion of an epicardial coronary artery, most often due to atherosclerotic plaque rupture/erosion and subsequent thrombus formation.
Ģ As compared to NSTEMI/UA, thrombotic occlusion is complete such that there is total transmural ischemia/infarct in the distribution of the large, occluded artery.
DIAGNOSIS
Clinical Presentation
HISTORY
Ģ Severe tearing chest pain or focal neurologic deficits should raise concern for aortic dissection.
Aortic dissection can mimic ACS; in addition, dissections of the ascending aorta may involve the right coronary artery and cause ST elevations on the ECG.
Ģ STEMI may have an atypical presentation particularly in female, elderly, and postoperative patients, as well as those with diabetes and chronic or end-stage kidney disease. Such patients may experience atypical or no chest pain and may instead present with confusion, dyspnea, unexplained hypotension, or HF.
Ģ STEMI should always be considered as an etiology when any patient is hemodynamically compromised (i.e., postoperative, delirium, or shock).
Ģ The initial history by the clinician should always include an inquiry about prior cardiac procedures or surgery. Prior PCI or CABG can have profound implications for acute revascularization management.
Ģ The clinician should assess for absolute and relative contraindications to thrombolytic therapy (see the following text) and potential issues complicating primary PCI (IV contrast allergy, PVD/peripheral revascularization, renal dysfunction, central nervous system disease, pregnancy, bleeding diathesis, or severe comorbidity).
Ģ Inquire about recent cocaine use. In this setting, aggressive medical therapy with nitroglycerin, coronary vasodilators, and benzodiazepines should be administered before reperfusion therapy is considered.
PHYSICAL EXAMINATION
Physical examination should be directed at identifying hemodynamic instability, pulmonary congestion, mechanical complications of MI, and other causes of acute chest discomfort.
Ģ The identification of a new systolic murmur may suggest the presence of ischemic MR or a VSD.
Ģ A limited neurologic exam to detect baseline cognitive and motor deficits and a vascular examination (lower extremity pulses and bruits) will aid in determining candidacy and planning for reperfusion treatment.
Ģ Cardiogenic shock due to right ventricular MI (RVMI) may be clinically suspected by the presence of hypotension, elevated jugular venous pressure, and absence of pulmonary congestion.
Ģ Bilateral arm BPs should be obtained to assess for the presence of aortic dissection.
Diagnostic Testing
ELECTROCARDIOGRAPHY
The ECG is paramount to the diagnosis of STEMI and should be obtained within 10 minutes of presentation. If the diagnosis of STEMI is in doubt, serial ECGs may help elucidate the diagnosis. Classic findings include the following:
Ģ Peaked upright T waves are the first ECG manifestation of myocardial injury.
Ģ ST elevations correlate with the territory of injured myocardium (Table 4-14).
TABLE 4-14
| ELECTROCARDIOGRAM-BASED ANATOMIC DISTRIBUTION |
| ST Elevation | Myocardial Territory | Coronary Artery |
| V1-V6 or LBBB | Anterior and septal walls | Proximal LAD or left main |
| v1-v2 | Septum | Proximal LAD or septal branch |
| V2-V4 | Anterior wall | LAD |
| V5-V6 | Lateral wall | LCX |
| II, III, aVF | Inferior wall | RCA or LCX |
| I, aVL | High lateral wall | Diagonal or proximal LCX |
LAD, left anterior descending artery; LBBB, left bundle branch block; LCX, left circumflex artery; RCA, right coronary artery.
Ģ Diagnostic ECG criteria for STEMI76
Ņ When ST elevations reach threshold values in two or more anatomically contiguous leads, a diagnosis of STEMI can be made.
Ņ In men > 40 years of age, threshold value for abnormal ST-segment elevation at the J point is ≥2 mm in leads V2 and V3 and >1 mm in all other leads.
In men < 40 years of age, threshold value for abnormal ST-segment elevation at the J point in leads V2 and V3 is >2.5 mm. Ņ In women, the threshold value of abnormal ST-segment elevation at the J point is >1.5 mm in leads V2 and V3 and >1 mm in all other leads.
Ņ In right-sided leads (V3R and V4R), the threshold for abnormal ST elevation at the J point is 0.5 mm, except in males waves in V1 or V2 represent Q waves of the posterior territory.
■ Ischemia of the circumflex artery may also be electrocardiographically silent.
Ņ The presence of reciprocal ST-segment depression opposite of the infarct territory increases the specificity for acute MI.
Ņ New LBBB suggests a large anterior wall MI with a worse prognosis.
Ņ ECG criteria for STEMI in patients with preexisting LBBB or RV pacing can be found in Table 4-15. Above criteria do not apply.
TABLE 4-15
CRITERIA FOR ST-SEGMENT ELEVATION FOR PRIOR LBBB OR RV-PACED RHYTHM
ECG Change
ST-segment elevation >1 mm in the presence of a positive QRS complex (concordant with the QRS)
ST-segment elevation >5 mm in the presence of a negative QRS complex (disconcordant with the QRS)
ST-segment depression >1 mm in V1-V3
LBBB, left bundle branch block; RV, right ventricular.
Sgarbossa's (GUSTO) criteria: Am J Cardiol. 1996;77:423; N Engl J Med. 1996;334:481; Pacing Clin Electrophysiol.
2001;24:1289.
Ņ ECG changes that mimic MI. ST-segment elevation and Q waves may result from numerous etiologies other than acute MI, including prior MI with aneurysm formation, aortic dissection, LV hypertrophy, pericarditis, myocarditis, pulmonary embolism, or they may be a normal finding (Table 4-16). It is critical to obtain prior ECGs to clarify the diagnosis.
TABLE 4-16
| DIFFERENTIAL DIAGNOSIS OF ST-SEGMENT ELEVATION ON ECG EXCLUDING STEMI |
| Cardiac Etiologies | Other Etiologies |
| Prior MI with aneurysm formation Aortic dissection with coronary involvement Pericarditis Myocarditis LV hypertrophy or aortic stenosis (with strain)a Hypertrophic cardiomyopathy Coronary vasospasm (cocaine, Prinzmetal angina) Early repolarization (normal variant) Brugada syndrome | Pulmonary embolism Hyperkalemia |
LV, left ventricular; MI, myocardial infarction; ST-segment elevation myocardial infarction.
aStrain may occur in numerous settings including systemic hypertension, hypotension, tachycardia, exercise, and sepsis.
Ņ Q waves. Development of new pathologic Q waves is considered diagnostic for transmural MI but may occur in patients with prolonged ischemia or poor collateral supply. The presence of Q waves only is not an indication for acute reperfusion therapy; however, it is very helpful to have an old ECG to compare to in order to determine chronicity. Diagnostic criteria include the following:
■ In leads V2 and V3, a pathologic Q wave is >0.02 second or a QS complex in V2 or V3. An isolated Q wave in lead V1 or lead III is normal.
■ In leads other than V1 through V3, presence of a Q wave >0.03 second and >0.1 mV deep or a QS complex in any two contiguous leads suggests prior MI.
■ R wave >0.04 second in V1 and V2 and R/S ratio >1 with a positive T wave suggest prior posterior MI (in the absence of RV hypertrophy or right bundle branch block [RBBB]).
Laboratoriesand imaging
Ģ STEMI diagnosis and initiation of treatment are done in a patient who reports prolonged chest discomfort or anginal equivalent with qualifying ECG findings. Attempting to wait for results of cardiac biomarkers will add unnecessary delay.
Ģ Blood samples should be sent for cardiac biomarkers (troponin), complete blood cell count, coagulation studies (aPTT, prothrombin time [PT], international normalized ratio [INR]), creatinine, electrolytes including magnesium, and type and screen. A lipid profile should be obtained in all patients with STEMI for secondary prevention (note however, that lipid levels may be falsely lowered
during the acute phase of MI).
Ģ Initial cardiac biomarkers (including troponin assays) may be normal, depending on the time in relation to symptom onset.
Ģ The risk of subsequent cardiac death is directly proportional to the increase in cardiac-specific troponins.
Measuring biomarkers until the peak level has been attained can be used to determine infarct size. Ģ Routine use of cardiac noninvasive imaging is not recommended for the initial diagnosis of STEMI. When the diagnosis is in question, a TTE can be performed to document regional wall motion abnormalities. If not adequately evaluated by TTE, a transesophageal echocardiogram (TEE) can be obtained to assess for acute complications of MI and presence of aortic dissection.
Ģ A portable chest radiograph is useful to assess for pulmonary edema and evaluate for other causes of chest pain including aortic dissection. Importantly, a normal mediastinal width does not exclude aortic dissection, especially if clinically suspected.
TREATMENT
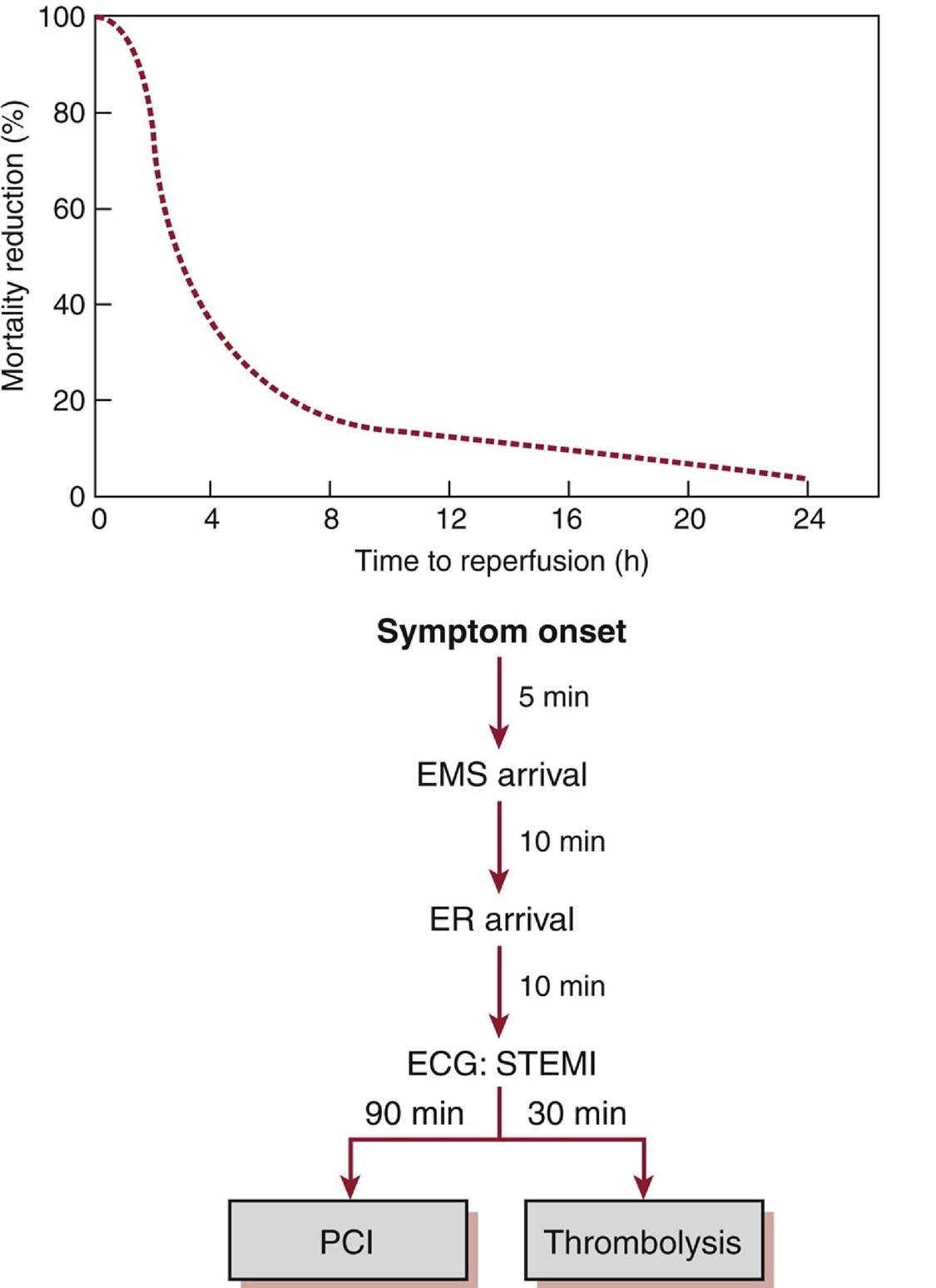
Ģ Prompt treatment should be initiated as soon as the diagnosis is suspected, as mortality and risk of subsequent HF are directly related to ischemia time (Figure 4-4).
![]()
Figure 4-4 The benefit of coronary reperfusion is inversely related to ischemia time.Top. Graphic representation of mortality benefit of coronary reperfusion as a function of ischemia time.77 Bottom. Recommended timeline of events following chest pain onset according to AHA/ACC guidelines.78 AHA/ACC, American Heart AssociationZAmerican College of Cardiology; ECG, electrocardiogram; EMS, emergency medical service; ER, emergency room; PCI, percutaneous coronary intervention; STEMI, ST-segment elevation myocardial infarction.
Ģ All medical centers should have in place and use an AHA/ACC guideline-based STEMI protocol. Centers that are not primary PCI capable should have protocols in place to meet accepted time-to- therapy guidelines, with either rapid transfer to a PCI-capable facility or administration of thrombolytics with subsequent transfer to a PCI center.
Ģ In the emergency department, an acute MI protocol should be activated that includes a targeted clinical examination and a 12-lead ECG completed within 10 minutes of arrival.
Ģ The goal of immediate management in patients with STEMI is to identify candidates for reperfusion therapy and to immediately initiate that process. Other priorities include relief of ischemic pain, as well as recognition and treatment of hypotension, pulmonary edema, and arrhythmia.
Ņ Supplemental oxygen should be administered if saturations are bgcolor=white>Prasugrel 60 mg loading
dose, 10 mg/d
Compared to clopidogrel, prasugrel is a quicker acting and more potent antiplatelet agent with improved efficacy but did significantly increase CABG bleeding rates. Prasugrel should not be used in patients >75 y old, 75 y old should not be given a loading dose and receive 0.75 mg/kg SC bid. An additional loading dose of 0.3 mg/kg should be given if the last dose of LMWH was >8 h prior to PCI. The use of LMWH is only validated in thrombolysis and rescue PCI. | | Bivalirudin | 0.75 mg/kg IV bolus, then 1.75 mg/kg/h | Bivalirudin has been validated in patients undergoing PCI and has not been studied in conjunction with thrombolysis. Patients who received a heparin bolus prior to bivalirudin had a lower incidence of stent thrombosis than those who only received bivalirudin. |
| Fondaparinux | 2.5 mg IV bolus, 2.5 mg Sub-Q daily | Shown to be superior to UFH when used during thrombolysis with decreased bleeding rates. Fondaparinux increases the risk of catheter thrombosis when used during PCI.79 |
| Nitroglycerin | 0.4 mg SL or aerosol infusion; 10Ł200 μg∕min IV | Sublingual or aerosol nitroglycerin can be given every 5 min for a total of three doses in the absence of hypotension. IV nitroglycerin can be used for uncontrolled chest discomfort. |
| Metoprolol | 25 mg PO qid, uptitrate as needed | β-Blockers should be avoided in patients with evidence of heart failure, hemodynamic instability, marked first-degree AV block, advanced heart block, and bronchospasm. |
| | | | | |
AV, atrioventricular; CABG, coronary artery bypass graft; LMWH, low-molecular-weight heparin; MI, myocardial infarction; PCI, percutaneous coronary intervention; SL, sublingual; STEMI, ST-segment elevation myocardial infarction; TIA, transient ischemic attack.
Ģ ASA 162-325 mg should be given orally (chewed) or rectally immediately to all patients with suspected acute MI; 325 mg is preferred for those who are ASA naive. After PCI, the subsequent dose of ASA is 81 mg/d indefinitely.80
Ģ P2Y12 inhibitor loading dose should be given to all STEMI patients, as part of DAPT, as soon as possible after presentation. Cost and bleeding risk should be taken into consideration when choosing an agent. (Please also refer to the antiplatelet section on UA/NSTEMI for background information and dosing on agents listed in the following text.)
Ņ If the patient is going for PCI, one of the following should be added to ASA and anticoagulant:
■ Ticagrelor 180 mg loading dose, then 90 mg bid (Note: maintenance ASA must be 75 years and with weight < 60 kg). Prasugrel should only be given after diagnostic angiography (or within an hour of PCI) given a higher incidence of bleeding compared to clopidogrel.81
Ņ If the patient is to receive fibrinolytic therapy, along with ASA and an anticoagulant, patients should receive:
■ Clopidogrel 300 mg loading dose if given during the first 24 hours of therapy; if started 24 hours after administration of fibrinolytics, a 600-mg loading dose is preferred. Maintenance is 75 mg/d.
■ Patients older than 75 years should not be given the loading dose.
Ģ GPIIb/IIIa inhibitors do not have a routine role in the initial presentation of STEMI patients or as part of adjunctive therapy with thrombolytics.
Ģ Anticoagulant therapy should be initiated on presentation in all patients with STEMI regardless of the choice of PCI or thrombolytic therapy. Please also refer to the Medications section for UA/NSTEMI for background information on agents listed in the following text.
Ņ Anticoagulant choice for patients who will receive primary PCI:
■ UFH is often preferred during PCI by many operators due to the availability and real-time therapeutic monitoring with activating clotting times (ACTs) in the catheterization laboratory. Additional bolus doses of UFH are given at PCI, with the dose and ACT goal dependent on whether a GPIIb/IIIa antagonist has been given.
■ Enoxaparin use in STEMI patients as an anticoagulant for PCI is unclear, and we generally do not recommend it.
■ Bivalirudin can be given to patients already treated with ASA and clopidogrel on presentation.
? Bivalirudin is an acceptable alternative to the use of combined heparin and GPIIb/IIIa inhibitor during PCI with lower bleeding rates but higher rate of stent thrombosis.82,83
? It is the agent of choice in patients with known HIT.
? It can be given with or without prior treatment with UFH. If patient is being treated with UFH, discontinue UFH for 30 minutes prior to starting bivalirudin.
? Dose is 0.75 mg/kg bolus, then 1.75 mg/kg/h infusion.
Ņ Patients who will receive fibrinolytic therapy should be started on either:
■ UFH with monitoring to ensure the activated PTT is twice the upper limit of normal. UFH should be continued for at least 48 hours after fibrinolysis. If angiography with intent to perform PCI is anticipated to occur early after fibrinolysis, then UFH may be preferable.
■ Enoxaparin, if the serum creatinine is 100 bpm or phosphodiesterase inhibitors (e.g., sildenafil) in previous 48 hours
Ņ Morphine (2-4 mg IV) can be used for refractory chest pain that is not responsive to nitroglycerin. Adequate analgesia decreases levels of circulating catecholamines and reduces myocardial oxygen consumption.
Ņ BBs improve myocardial ischemia, limit infarct size, and reduce major adverse cardiac events including mortality, recurrent ischemia, and malignant arrhythmias.
■ Oral BBs should be started in all patients with STEMI within the first 24 hours who do not have signs of new HF, evidence of cardiogenic shock (Killip class II or greater), age older than 70 years, SBP < 120 mm Hg, pulse > 110 or 120 minutes or time-to-transfer > 120 minutes). Transfer to a PCI-capable facility should occur regardless of whether fibrinolytics are given or not.
■ Fibrinolytic therapy is indicated for use if given within 12 hours of the symptom onset with qualifying ECG changes of ST elevation, new LBBB, or true posterior MI. When given, it should be administered within 30 minutes of initial patient contact. Fibrinolytic therapy is most successful when given in the first 3 hours of symptom onset, after which the benefit tapers.
■ Patients presenting to a hospital without PCI capability should be transferred for primary PCI, rather than being given fibrinolytics, if time from first medical contact to PCI will not be >120 minutes. This seems particularly relevant to patients arriving 3-12 hours from symptom onset.
■ In patients transferred for PCI, primary PCI significantly lowered the incidence of death, MI, or stroke compared to on-site thrombolysis.91-94
■ All patients should be transferred to a PCI-capable facility after fibrinolysis (early routine angiography); this should occur urgently if patients are in shock or have failed reperfusion.
■ Available thrombolytic agents include the fibrin-selective agents such as alteplase (recombinant tissue plasminogen activator [rt-PA]), reteplase (r-PA), and tenecteplase (TNK-tPA). Streptokinase is the only nonselective agent in use. Further details and dosing information can be found in Table 4-18.
? TNK-tPA is the current agent of choice due to similar efficacy, lower risk of bleeding, and convenient single bolus administration as compared to rt-PA. Streptokinase is the cheapest and still widely used worldwide.
| |
| FiBRiNOLYTil | C AGENTS |
| Medication | Dosage | Comments |
| Streptokinase | 1.5 million | Produces a generalized fibrinolytic state (not clot |
| (SK) | units IV over 60 min | specific). SK reduces mortality following STEMI: 18% relative risk reduction and 2% absolute risk reduction.95 Allergic reactions including skin rashes, fever, and anaphylaxis may be seen in 1%-2% of patients. Isolated hypotension occurs in 10% of patients and usually responds to volume expansion. Because of the development of antibodies, patients who were previously treated with SK should be given an alternate thrombolytic agent. |
| Recombinant | 15 mg IV | Fibrin-selective agent with improved clot specificity |
| tissue | bolus | compared to SK. |
| plasminogen | 0.75 mg/kg | Does not cause allergic reactions or hypotension. |
| activator (rt- PA) | over 30 min (maximum 50 mg) | Mortality benefit compared to SK at the expense of an increased risk of intracranial hemorrhage.96Æ97 |
| | 0.5 mg/kg over 60 min (maximum 35 mg) |
| Reteplase (rŁ PA) | Two 10-unit IV boluses administered 30 min apart | Fibrin selective agent with a longer half-life but reduced clot specificity compared to rt-PA. Mortality benefit equivalent to that of rt-PA.97 |
| Tenecteplase (TNK-tPA) | 0.5 mg/kg IV bolus (total dose 30-50 mg) | Genetically engineered variant of rt-PA with slower plasma clearance, improved fibrin specificity, and higher resistance to PAI-1. Mortality benefit equivalent to that of rt-PA with reduced bleeding rates.98 Monitoring is required with a goal aPTT of 1.5-2.5 times control. |
aPTT, activated partial thromboplastin time; PAI-1, plasminogen activator inhibitor-1; STEMI, ST-segment elevation myocardial infarction.
? Fibrin-selective agents should be used in combination with anticoagulant therapy, ASA, and clopidogrel (see earlier). GPIIb/IIIa inhibitors should not be used in conjunction. Prasugrel and ticagrelor have not been studied for use with fibrinolytics.
■ Fibrinolytic therapy is contraindicated:
? In patients with ECG evidence of ST-segment depressions (unless posterior MI suspected).
? In those who are asymptomatic with initial symptoms occurring >24 hours prior (this is in contrast to patients who are asymptomatic with symptom onset 50% reduction in ST-segment elevations at 90 minutes
Reperfusion arrhythmia (i.e., accelerated idioventricular rhythm) up to 2 hours after completion of infusion
Emergency CABG is a high-risk procedure that should be considered only if the patient has severe left main disease or refractory ischemia in the setting of failed PCI or coronary anatomy that is not amenable to PCI. Emergency surgery should also be considered for patients with acute mechanical complications of MI including papillary muscle rupture, severe ischemic MR, VSD, ventricular aneurysm formation in the setting of intractable ventricular arrhythmias, or ventricular free wall rupture.
ri-infarct Management
Γhe coronary care unit (CCU) was the first major advance in the modern era of treatment of acute MI. ž patients with STEMI should be observed in a specialized CCU or intensive care unit setting for at east 24 hours after STEMI.
atients should have continuous telemetry monitoring to detect for recurrent ischemia and arrhythmias. )aily evaluation should include assessment for recurrent chest discomfort, new HF symptoms, and outine ECGs. Physical exam should focus on new murmurs and any evidence of HF.
baseline echocardiogram should be obtained to document EF, wall motion abnormalities, valvular esions, and presence of ventricular thrombus.
Dardiac pacing may be required in the setting of an acute MI. Rhythm disturbance may be transient in ature, in which case temporary pacing is sufficient until a stable rhythm returns (see the following ext). As compared to inferior wall MIs where AV block is transient and stable, AV block with anterior vall MIs can be unstable with wide QRS escape rhythms with 80% mortality and usually requires
temporary and then permanent pacemakers.
Post-STEMI Medical Therapy
Ģ See also Medications section for UA/NSTEMI.
Ģ ASA should be continued indefinitely. Dose of 81 mg/d has been shown to be effective after PCI; however, the range of 75-162 mg/d has also been endorsed.
Ģ Clopidogrel (75 mg/d), prasugrel (10 mg/d), or ticagrelor (90 mg bid) should be given for a minimum of 12 months regardless of whether a bare metal stent (BMS) or drug-eluting stent (DES) was used (this is in contrast to non-ACS patients who receive a BMS and the minimum duration of therapy is 1 month).
Ģ BBs confer a mortality benefit following acute MI. Treatment should begin as soon as possible (preferably within the first 24 hours) and continued indefinitely unless contraindicated.
Ģ ACE inhibitors provide a reduction in short-term mortality, incidence of HF, and recurrent MI when initiated within the first 24 hours of an acute MI.101,102
Ņ Patients with EF < 40%, large anterior MI, and prior MI derive the most benefit from ACE inhibitor therapy.
Ņ Contraindications include hypotension, history of angioedema with use, pregnancy, acute renal failure, and hyperkalemia.
Ņ ARBs can be used in patients who are intolerant of ACE inhibitors.
Ģ HMG-CoA reductase inhibitors should be started in all patients in the absence of contraindications. Several trials have shown the benefit of early and aggressive use of high-dose statins following acute MI. The goal is at least 50% reduction in LDL or LDL High-dose ASA (up to 650 mg qid maximum) is generally considered a first-line agent. NSAIDs such as ibuprofen may be used if ASA is not effective but should be avoided early after acute MI.
■ Colchicine along with ASA may also be beneficial for recurrent symptoms and may also be superior to each agent alone.
■ Glucocorticoids (prednisone 1 mg/kg daily) may be useful if symptoms are severe and refractory to initial therapy. Steroids should be used sparingly because they may lead to an increased risk of recurrence of pericarditis. Use should also be deferred until at least 4 weeks after acute MI due to their adverse impact on infarct healing and risk of ventricular aneurysm.
■ Heparin should be avoided in the setting of pericarditis with or without pericardial effusion because it may lead to pericardial hemorrhage.
Ņ Dressler syndrome is thought to be an autoimmune process characterized by malaise, fever, pericardial pain, leukocytosis, elevated erythrocyte sedimentation rate, and often a pericardial effusion. In contrast to acute pericarditis, Dressler syndrome occurs 1-8 weeks after MI. Treatment is identical to acute pericarditis.
Ņ Arrhythmias. Cardiac rhythm abnormalities are common following MI and may include conduction block, atrial arrhythmias, and ventricular arrhythmias. Arrhythmias that result in hemodynamic compromise require prompt, aggressive intervention. If the arrhythmia precipitates refractory angina or HF, urgent therapy is warranted. For all rhythm disturbances, exacerbating conditions should be addressed, including electrolyte imbalances, hypoxia, acidosis, and adverse drug effects. Refer to section on Cardiac Arrhythmia management for further details. Atropine should be attempted for all bradyarrhythmias in the setting of STEMI. Bradycardia is a common complication of intense vagal input to the AV node as a result of baroreceptor activation in the myocardium (also called Bezold- Jarisch reflex).
Ņ Transcutaneous and transvenous pacing. Conduction system disease that progresses to complete heart block or results in symptomatic bradycardia can be effectively treated with cardiac pacing. A transcutaneous pacing device can be used under emergent circumstances; however, a temporary transvenous system should be used for longer duration therapy.
■ Absolute indications for temporary transvenous pacing include asystole, symptomatic bradycardia, recurrent sinus pauses, complete heart block, and incessant polymorphic VT.
■ Temporary transvenous pacing may also be warranted for new trifascicular block, new Mobitz II block, and patients with LBBB who require a pulmonary artery catheter, given the risk of developing complete heart block.
Ņ Implantable cardioverter-defibrillators (ICDs) should not routinely be implanted in patients with reduced LV function following MI or those with VT/VF in the setting of ischemia or immediately following reperfusion (20 mm Hg), depressed cardiac index (Echocardiography may identify patients with particularly thinned ventricular walls at risk for rupture.
■ Despite optimal intervention, mortality of free wall rupture remains >90%.
Ņ Papillary muscle rupture (please also refer to earlier MR section) is a rare complication after MI and is associated with abrupt clinical deterioration. The posterior medial papillary muscle is most commonly affected due to its isolated vascular supply, but anterolateral papillary muscle rupture has been reported. Of note, papillary muscle rupture may be seen in the setting of a relatively small acute MI or even NSTEMI.
■ The diagnostic test of choice is echocardiography with Doppler imaging and/or TEE because physical exam reveals a murmur in only ~50% of cases.
■ Initial medical therapy should include aggressive afterload reduction. Patients with refractory HF and those with hemodynamic instability may require inotropic support with dobutamine and/or IABP. Surgical repair is indicated in the majority of patients.
Ņ Ventricular septal rupture is most commonly associated with anterior MI occurring 3-5 days after MI. The perforation may follow a direct course between the ventricles or a serpiginous route through the septal wall.
■ Diagnosis can be made by echocardiography with Doppler imaging and often requires TEE.
■ Diagnosis should be suspected in the postinfarct patient who develops HF symptoms and a new holosystolic murmur.
■ Stabilization with afterload reduction, inotropic support, and/or IABP may be necessary for hemodynamically unstable patients until definitive therapy with surgical repair can be performed.
■ In hemodynamically stable patients, surgery is best deferred for at least a week to improve patient outcome. Left untreated, mortality approaches 90%.
■ Percutaneous device closure in the cardiac catheterization laboratory can be performed in select patients with an unacceptable surgical risk.