Ventricular Tachyarrhythmias
GENERAL PRINCIPLES
• Ventricular tachyarrhythmias should be initially approached with assumption that they will have malignant course, until proven otherwise.
• Characterization of the arrhythmia involves consideration of hemodynamic stability, duration and ECG morphology of tachycardia, and the presence or lack of underlying structural heart disease.
• Characterization will aid in determining the patient's risk for sudden cardiac arrest (SCA) and need for therapeutic intervention and/or device implantation.
Definition
• Nonsustained ventricular tachycardia (NSVT): Three or more consecutive ventricular complexes (>100 bpm) that terminate spontaneously within 30 seconds.
• Sustained monomorphic ventricular tachycardia (SMVT): Tachycardia of ventricular origin with single QRS morphology lasting longer than 30 seconds or requiring cardioversion due to hemodynamic compromise.
• Polymorphic ventricular tachycardia (PMVT): VT is characterized by evolving QRS morphology. TdP is a variant of PMVT typically preceded by prolonged QT interval in SR. PMVT is associated with hemodynamic collapse or instability.
• VF: Associated with disorganized mechanical contraction of ventricles, hemodynamic collapse, and sudden death. ECG reveals irregular and rapid oscillations (250-400 bpm) of highly variable amplitude without clearly identifiable QRS complexes or T waves.
• Ventricular arrhythmias—major cause of sudden cardiac death (SCD).
î SCD—unexpected death that generally occurs within 1 hour of onset of symptoms in person without prior condition that would appear fatal. In the US, approximately 350,000 cases of SCD occur annually.
■ Among patients with aborted SCD, ischemic heart disease is most commonly associated cardiac structural abnormality. Most cardiac arrest survivors do not have evidence of acute MI; however, >75% have evidence of previous infarcts.
■ Nonischemic cardiomyopathy (NICM) is also associated with an elevated risk for SCD.15
Etiology
• VT associated with structural heart disease
î Most ventricular arrhythmias are associated with structural heart disease, typically related to active ischemia or prior infarct.
■ Scar and the peri-infarct area provide substrate for reentry that produces SMVT.
■ PMVT and VF—commonly associated with ischemia and are presumed cause of most out-ofhospital SCD.
o NICM typically involves progressive dilation and fibrosis of ventricular myocardium, providing arrhythmogenic substrate.
î Infiltrative cardiomyopathies (secondary to sarcoidosis, hemochromatosis, amyloidosis, etc.) affect smaller patient population that is at significant risk for ventricular arrhythmias and whose management is less clearly defined.
î Adults with prior repair of congenital heart disease are commonly afflicted with both VT and SVT.
î Arrhythmogenic right ventricular dysplasia (ARVD) or cardiomyopathy—marked by fibrofatty replacement of the RV (and sometimes LV) myocardium giving rise to left bundle branch block (LBBB) morphology VT and is associated with sudden death, particularly in young athletes.
î Bundle branch reentry VT—form of ventricular tachyarrhythmia that uses His-Purkinje system in a reentrant circuit and is typically associated with cardiomyopathy and abnormal conduction system.
• VT in the absence of structural heart disease
î Inherited ion channelopathies, such as those seen in Brugada syndrome and LQTS, can lead to PMVT and sudden death in patients without evidence of structural heart disease.
î Catecholaminergic PMVT involves inherited, exercise-induced VT related to irregular calcium processing.
î Idiopathic VT—diagnosis of exclusion that requires documented absence of structural heart disease, genetic disorders, and reversible etiologies (i.e., ischemia, metabolic abnormalities).
■ Most originate from RV outflow tract (RVOT) and are amenable to ablation.
■ LV outflow tract (LVOT) VTs, arising from near the coronary cusps or aortomitral continuity, or fascicular VTs (using anterior and posterior divisions of the left bundle branch) are less common forms of idiopathic VT.
■ Tachycardia-mediated cardiomyopathy can result if left untreated.
DIAGNOSIS
Clinical Presentation
• Evaluation of WCTs should always begin with prompt assessment of vital signs and symptoms. If arrhythmia is poorly tolerated, postpone further evaluation and proceed to acute management per ACLS guidelines. If patient is clinically stable, rhythm should be carefully analyzed to distinguish VT from SVT. A common mistake is the assumption that hemodynamic stability supports the diagnosis of SVT over VT.
• VT represents the majority of WCT seen in the inpatient setting with reported prevalence of ~80%. Eliciting historical points of emphasis and closely assessing ECG properties can help delineate mechanism of underlying rhythm disturbance. Begin with the following questions:
î Does patient have history of structural heart disease?
■ Patients with structural heart disease are much more likely to have VT than SVT as etiology of WCT. In one analysis, 98% of patients with WCT on ECG who had prior MI proved to have VT.16
î Does patient have implanted device (PPM or ICD) or wide QRS at baseline?
■ Presence of either pacemaker or ICD should raise suspicion for device-mediated WCT.
■ Device-mediated WCT can occur from ventricular pacing at rapid rate either caused by tracking of an atrial tachyarrhythmia or alternatively by “endless loop tachycardia” from tracking of retrograde atrial impulses created by preceding ventricular paced beat. In either case, tachycardia rate is a clue to mechanism because it is typically equal to programmed upper rate limit (URL) of the device. A commonly programmed URL is 120 bpm. Tachycardia rate above URL effectively excludes device-mediated WCT.
■ Presence of an implantable device can be confirmed by inspection of the chest wall (usually left chest for right-handed patients), CXR, or appearance of pacing spikes on ECG or telemetry.
■ Patients with known right bundle branch block (RBBB), LBBB, or intraventricular conduction delay (IVCD) at baseline presenting with WCT will have QRS morphology identical to baseline in the presence of SVT. In contrast, some patients with narrow QRS at baseline will manifest WCT due to SVT when a rate-related bundle branch block is present (SVT with aberrancy).
î What are patient's home medications?
■ Home medication list should be carefully reviewed for any drugs with proarrhythmic side effects, especially those that can prolong the baseline QT interval—including many class I and III antiarrhythmics, certain antibiotics, and antipsychotics.
■ Medications that can lead to electrolyte derangements, such as loop and potassium-sparing diuretics, ACE-I, ARB, and digoxin toxicity, if applicable, should be considered in setting of any arrhythmia.
Differential Diagnosis
• WCT is secondary to either SVT with aberrant conduction or VT. Differentiation between these rhythm abnormalities is of utmost importance. The pharmacologic agents used in the management of SVT (i.e., adenosine, β-blockers, calcium channel blockers) may cause hemodynamic instability if used
in the setting of VT. Therefore, all WCTs are considered ventricular in origin until proven otherwise.
• Other less common mechanisms of WCT include A-AVRT, hyperkalemia-induced arrhythmia, or pacemaker-induced tachycardia.
• Telemetry artifact from poor lead contact or repetitive patient motion (tremor, shivering, brushing teeth, chest physical therapy, etc.) can mimic VT or VF.
Diagnostic Testing
LABORATORIES
• Basic studies should include CBC, complete metabolic panel, magnesium level, and serial troponins.
• Additional labs based on clinical suspicion should also be obtained during initial workup.
ELECTROCARDIOGRAPHY
• Differentiation of SVT with aberrancy from VT based on ECG analysis is critical for determination of appropriate therapy.
Features diagnostic of VT: AV dissociation, capture or fusion beats, an absence of RS morphology in all precordial leads (V1-V6), and LBBB morphology with right axis deviation. In absence of these features, examination of an RS complex in a precordial lead for an RS interval >100 ms is consistent with VT. In addition, characteristic QRS morphologies that are suggestive of VT may be sought, as shown in Figure 7-2.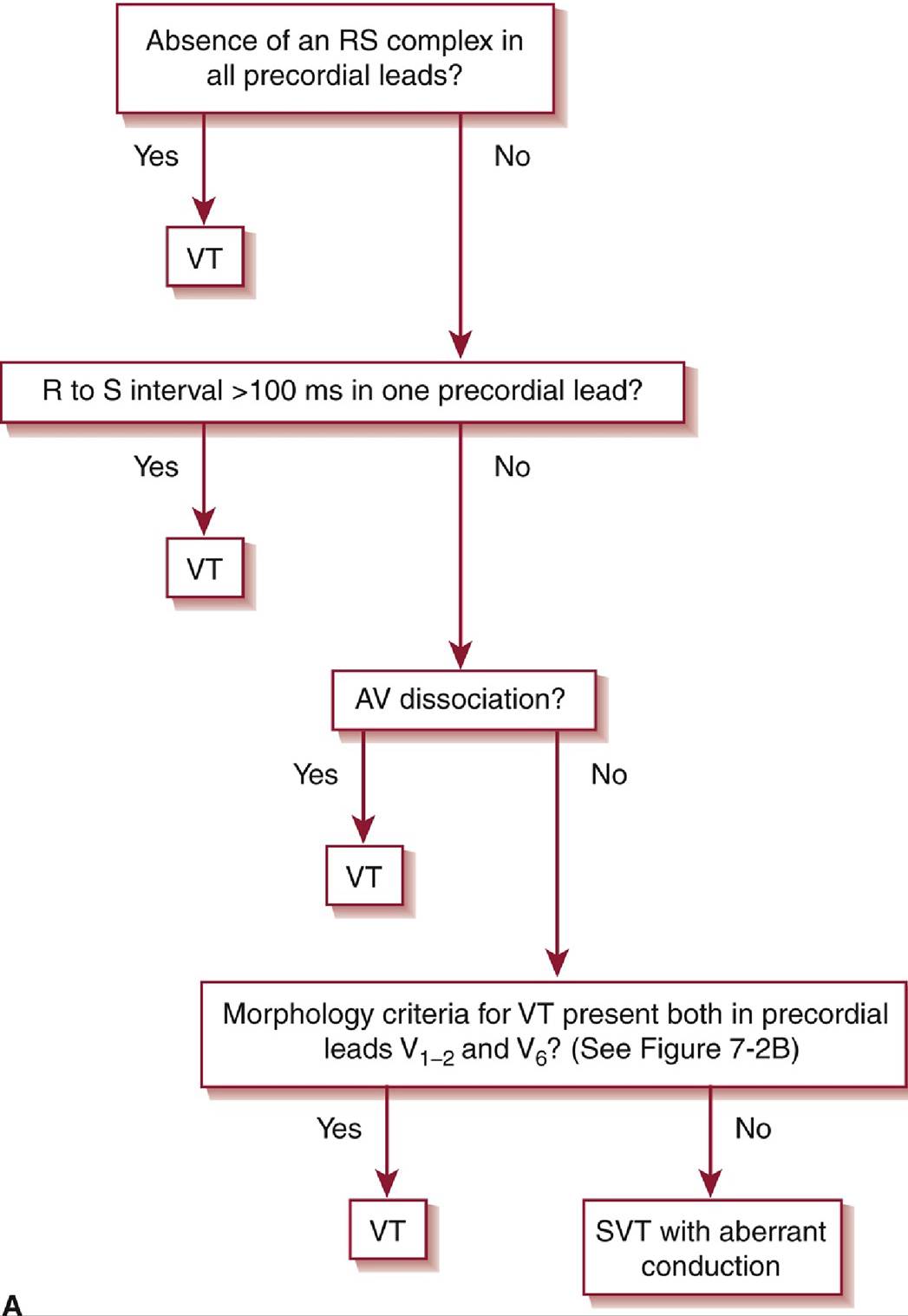
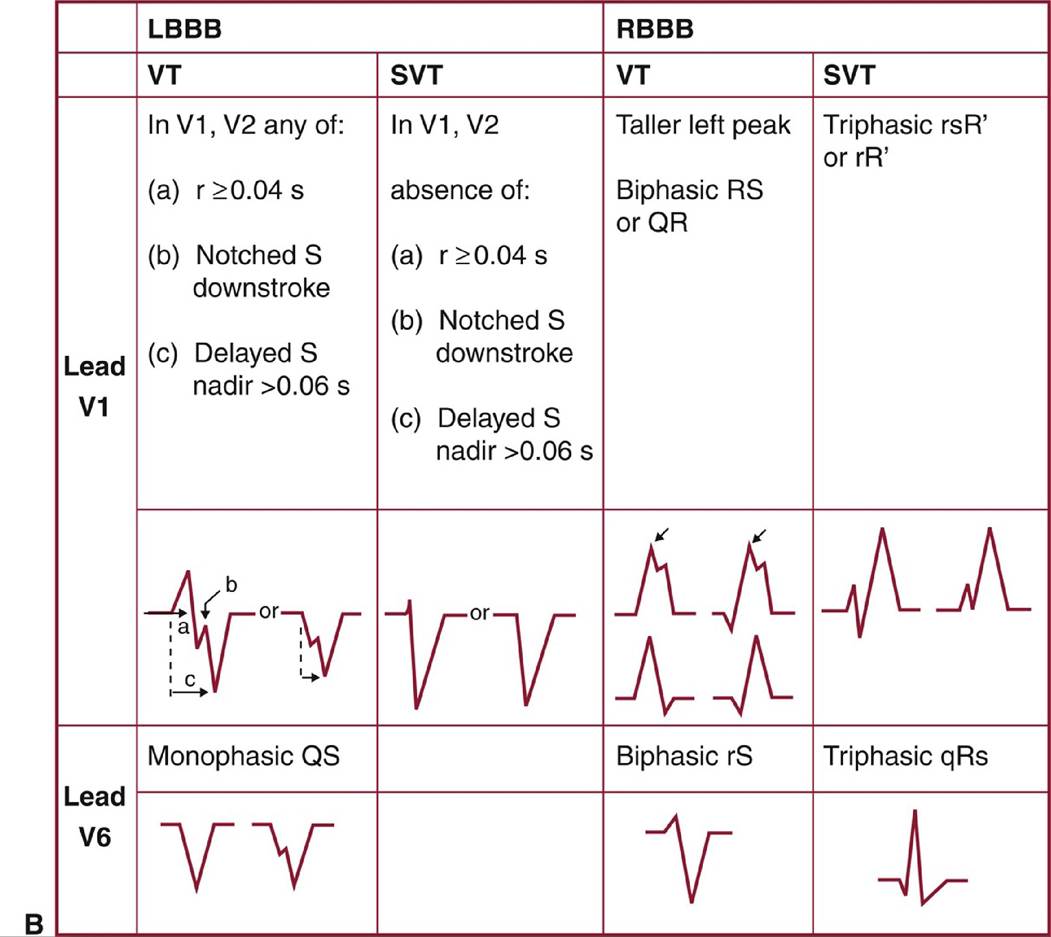
Figure 7-2 A and B, Brugada criteria for distinguishing ventricular tachycardia from supraventricular tachycardia with aberrancy in wide-complex tachycardias.LBBB, left bundle branch block; RBBB, right bundle branch block; SVT, supraventricular tachyarrhythmia; VT, ventricular tachycardia.(Reprinted with permission from Sharma S, Smith T. Advanced electrocardiography. In: Cuculich PS, Kates AM, eds. The Washington Manual of Cardiology Subspecialty Consult. 3rd ed. Lippincott, Williams & Wilkins; 2014.)
• ECG pearls
î Brugada syndrome ECG patterns
■ Type 1: characterized by ST segment elevation of at least 2 mm with a coved morphology in leads V1 and V2, associated with an incomplete or complete RBBB, and followed by descending T wave.
■ Type 2 (also referred to as “saddleback” pattern): characterized by ST segment elevation of 2 mm followed by a trough within the ST segment with continued ST elevation of ≥1 mm and positive or biphasic T wave.
■ Patterns may be observed spontaneously or unmasked after fever, drug administration, stress, etc.
■ Only type 1 pattern is diagnostic of Brugada syndrome, while type 2 is suggestive but not specific. î ARVD
■ NSR ECG at baseline with the presence of an epsilon wave (late potential just after QRS) and/or T wave inversions in the right precordial leads is a diagnostic criterion for ARVD.
■ VT in ARVD generally arises from an RV origin and is therefore likely to have LBBB configuration; patients may present with NSVT or PMVT.
î Bundle branch reentrant VT
■ Baseline ECG often shows IVCD.
■ In VT, ECG typically presents with LBBB morphology with electrical impulse traveling “down” the right bundle and “up” the left bundle.
î FascicularVT
■ ECG in VT shows RBBB morphology with superior axis.
î LQTS
■ Abnormal prolongation of QT interval on ECG at baseline (ideally measured in leads II and V5 or V6).
■ QTc ≥450 ms in men and 460 ms in women.
■ ECG in VT often shows TdP degenerating into VF.
î Outflow tract VT
■ ECG characteristically has inferior axis with LBBB morphology.
■ R/S transition in precordial leads can aid in localization: early transition (V1 or V2) suggests an LVOT origin, whereas later transition (V4 or after) is suggestive of an RVOT origin.
IMAGING
• Presence or absence of structural heart disease should be initially evaluated by TTE.
• Further imaging (cardiac MRI, noninvasive stress test, coronary angiogram, etc.) should be obtained based on suspected etiology.
TREATMENT
• Differentiation of SVT with aberrancy from VT based on analysis of surface ECG is critical in the determination of appropriate treatment.
î For acute therapy of SVT, IV medications such as adenosine, calcium channel blockers, or β- blockers are used (see “Treatment” of “Supraventricular Tachyarrhythmias” earlier in this chapter). However, calcium channel blockers and β-blockers can produce hemodynamic instability in patients with VT.
• Immediate unsynchronized DCCV is the primary therapy for pulseless VT and VF.
Nonpharmacologic Therapies
• ICDs provide automatic recognition and treatment of ventricular arrhythmias. ICD implantation improves survival in patients resuscitated from ventricular arrhythmias (secondary prevention of SCD) and in individuals without prior symptoms who are at high risk for SCD (primary prevention of SCD).
î Idiopathic VT is thought to be benign in the absence of structural heart disease. Therefore, ICD implantation is not appropriate.
î Secondary prevention of SCD with ICD implantation is indicated for most patients who survive SCD outside of the peri-MI setting. The superiority of ICD therapy to chronic antiarrhythmic drug therapy has been demonstrated.17
î Primary prevention of SCD with ICD implantation is indicated for patients who are at high risk of SCD. The efficacy of ICD implantation for primary prevention of SCD in the setting of cardiomyopathy has been established in multiple prospective clinical trials.18-20 Most patients with LV ejection fraction of been shown to reduce both the burden of VT and ICD shocks in treated patients.27