Supraventricular Tachyarrhythmias
GENERAL PRINCIPLES
• SVTs—often recurrent, rarely persistent, and can result in visits to emergency departments and primary care physician offices.
• Always begin with prompt assessment of hemodynamic stability and clinical status.
• Diagnostic and therapeutic discussion that follows is aimed at hemodynamically stable patients. If a patient is clinically unstable based on signs and symptoms, immediately proceed to cardioversion per ACLS guidelines.
Definition
• Tachyarrhythmias that require atrial or AV nodal tissue or both for their initiation and maintenance are termed SVT.
• The QRS complex in most SVTs is narrow (QRS Usually, normal physiologic response to hyperadrenergic states (fever, pain, hypovolemia, anemia, hypoxia, etc.).
î Can be induced by illicit (cocaine, amphetamines, methamphetamine) and prescription (theophylline, atropine, β-adrenergic agonists) drugs.
î Inappropriate sinus tachycardia refers to persistently elevated resting sinus rate (>100 bpm) in the absence of identifiable physical, pathologic, or pharmacologic influence.
• Ectopic atrial tachycardia (EAT)
î EAT with variable block can present as an irregularly irregular rhythm and can be distinguished from AFL by an atrial rate of 150-200 bpm.
î EAT with variable block is associated with digoxin toxicity.
î Characterized by regular atrial activation pattern with P wave morphology originating outside the sinus node complex resulting in long RP tachycardia.
î Mechanism: Enhanced automaticity, triggered activity, and possibly microreentry.
• AVNRT
î Reentrant rhythm requiring functional dissociation of the AV node into two pathways with both antegrade and retrograde conduction through the AV node.
î Not correlated with structural heart disease and can occur at any age, with a predilection for middle age and female gender.
î Typical AVNRT—major cause of short RP tachycardia.
■ ECG appearance has characteristic “absent P waves” because atrial activation is coincident with the QRS complex. Commonly, atrial activation can occur at terminal portion of QRS to create a pseudo-r' (V1) or pseudo-s' (II) compared with sinus rhythm (SR) QRS.
■ Conduction occurs in an antegrade fashion down the slow AV nodal pathway with retrograde conduction occurring back up the fast pathway, manifesting in short RP tachycardia by ECG.
î Atypical AVNRT
■ Less common; antegrade conduction proceeds down a fast AV nodal pathway with retrograde conduction up a slow AV nodal pathway, leading to a long RP tachycardia.
■ ECG: Retrograde P wave inscribed well after QRS complex in second half of RR interval.
• AVRT
î Reentrant tachycardia with circuit consisting of the normal AV conduction system and accessory pathway linking atrial and ventricular tissues.
î Orthodromic AVRT—most common AVRT, accounting for about 95% of all AVRT.
■ Accessory pathway-mediated reentrant rhythm with antegrade conduction to the ventricle down the AV node and retrograde conduction to the atrium up an accessory or “bypass” tract, leading to short RP tachycardia.
■ ECG: Retrograde P waves frequently seen after the QRS complex and usually distinguishable from the QRS (i.e., separated by >70 ms).
■ Most common mechanism of SVT in patients with Wolff-Parkinson-White (WPW) syndrome who have preexcitation (defined by short PR and a delta wave on upstroke of QRS) present on SR ECG.
■ Can occur without preexcitation when conduction through bypass tract occurs only during tachycardia in retrograde fashion (“concealed pathway”).
■ Less commonly, retrograde conduction through the accessory pathway to the atrium proceeds slowly enough for atrial activation to occur in the second half of the RR interval, leading to a long RP tachycardia.
î Antidromic AVRT (A-AVRT): Occurs when conduction to the ventricle is down an accessory bypass tract with retrograde conduction through the AV node or second bypass tract.
■ ECG: QRS seems consistent with VT; however, the presence of preexcitation on the baseline QRS should be diagnostic for WPW syndrome.
■ A-AVRT is seen in unable to
| | procedure. | stimulation during relaxation phase. | against a closed airway for several seconds followed by relaxation. | tolerated. | follow commands. |
| Carotid | Check for | Vagal | First, apply enough | Well | Recent TIA or |
| sinus | carotid bruits | stimulation. | pressure to simply feel | tolerated. | stroke or |
| massage | and history of CVA; then place in recumbent position with neck extended. | | carotid pulse with index and middle fingers. If no effect, then use rotating motion for 35 s. | Risk of embolizing carotid plaque. Never massage both carotids. | ipsilateral significant carotid artery stenosis o carotid artery bruit. |
| Adenosine | Explain the | AV nodal | Initial: 6 mg IV rapid | Precipitate | Significant |
| | potential side effects to the patient. | blocking agent. Short acting (serum halflife 4 8 min). | bolus via antecubital vein, followed by 1030 mL saline flush. If desired or effect not achieved, can repeat 12 mg followed by 12 mg after 1- to 2-min intervals. Central venous line: 3 mg IV initial dose. | prolonged asystole in patients with sick sinus syndrome or second- or third- degree AV block. | bronchospasm. |
Atrioventricular nodal reentrant tachycardia, atrioventricular reentrant tachycardia, and many atrial tachycardias will terminate with vagal maneuvers or adenosine, and in atrial flutter, the appearance of flutter waveform will help diagnosis.
Water immersion, eyeball pressure, coughing, gagging, deep breathing, etc., are other alternative vagal maneuvers.
AV, atrioventricular; CVA, cerebrovascular accident; TIA, transient ischemic attack.
aPatients should be under continuous ECG monitoring for each of these procedures. To enhance diagnostic value of rhythm strip, use leads V1 and II (atrial activity).
Radiofrequency ablation (RFA): Definitive cure with high success rates ranging from 80% to 100% for many SVTs including AVNRT, accessory bypass tract-mediated tachycardias, focal AT, and AFL.
• Complication risk generally 60% in hospitalized patients.
• Paroxysmal—recurrent form of AF in which individual episodes are 1 year, still deemed manageable with cardioversion or RFA.
• Permanent—AF after failed attempts at electrical or chemical cardioversion, has been present for more than 1 year, or has been accepted due to contraindications for cardioversion or lack of symptoms.
Epidemiology
• Most common sustained tachyarrhythmia for which patients seek treatment and most likely etiology for irregularly irregular rhythm discovered on an inpatient ECG. Typically, a disease of the elderly, affecting >10% of those aged >75 years.
• Independent risk factors include advanced age, male gender, and comorbid presence of diabetes mellitus and cardiovascular diseases such as CHF, valvular heart disease, HTN, and previous MI.4 Age 100 bpm).
• Important to distinguish AF from other tachycardia mechanisms with an irregular ventricular response such as MAT and AFL with variable conduction.
Clinical Presentation
• Symptoms can range from nonexistent to nonspecific (fatigue) to severe (acute pulmonary edema, palpitations, angina, syncope).
• Symptoms usually secondary to rapid ventricular response (RVR) to AF rather than loss of atrial systole. However, patients with significant ventricular systolic or diastolic dysfunction can have symptoms directly attributable to loss of atrial systole.
• Prolonged tachycardia from AF may lead to tachycardia-induced cardiomyopathy.
TREATMENT
• Medical management is directed at three therapeutic goals: (1) rate or (2) rhythm control and (3) prevention of thromboembolic events.
• Previous studies have shown there is no mortality benefit to a strategy aimed at maintaining SR.10 Therefore, rate control and management of thromboembolic risk are preferred strategy in asymptomatic and minimally symptomatic patients. Rhythm control is reserved for patients who remain symptomatic despite reasonable efforts at rate control.
Medications
• Medical management begins with consideration of appropriate antithrombotic therapy. Coumadin has shown to be superior to aspirin (ASA) or ASA in combination with clopidogrel for prevention of thromboembolic events in patients with nonvalvular-associated AF.
• Direct oral anticoagulants (DOAC) such as dabigatran, rivaroxaban, apixaban, and edoxaban have been directly compared with warfarin in randomized prospective trials and have been shown to be either noninferior or superior to coumadin in preventing stroke in AF patients.
• Rate control of AF is achieved with medications that limit conduction through the AV node such as non- dihydropyridine calcium channel blockers (verapamil, diltiazem, etc.), β-adrenergic antagonists, and digoxin.
• Rhythm control can be attempted with selected antiarrhythmic drugs. Pharmacologic control with antiarrhythmic drugs is more effective at preventing recurrence of AF than chemical cardioversion (Table 7-3).
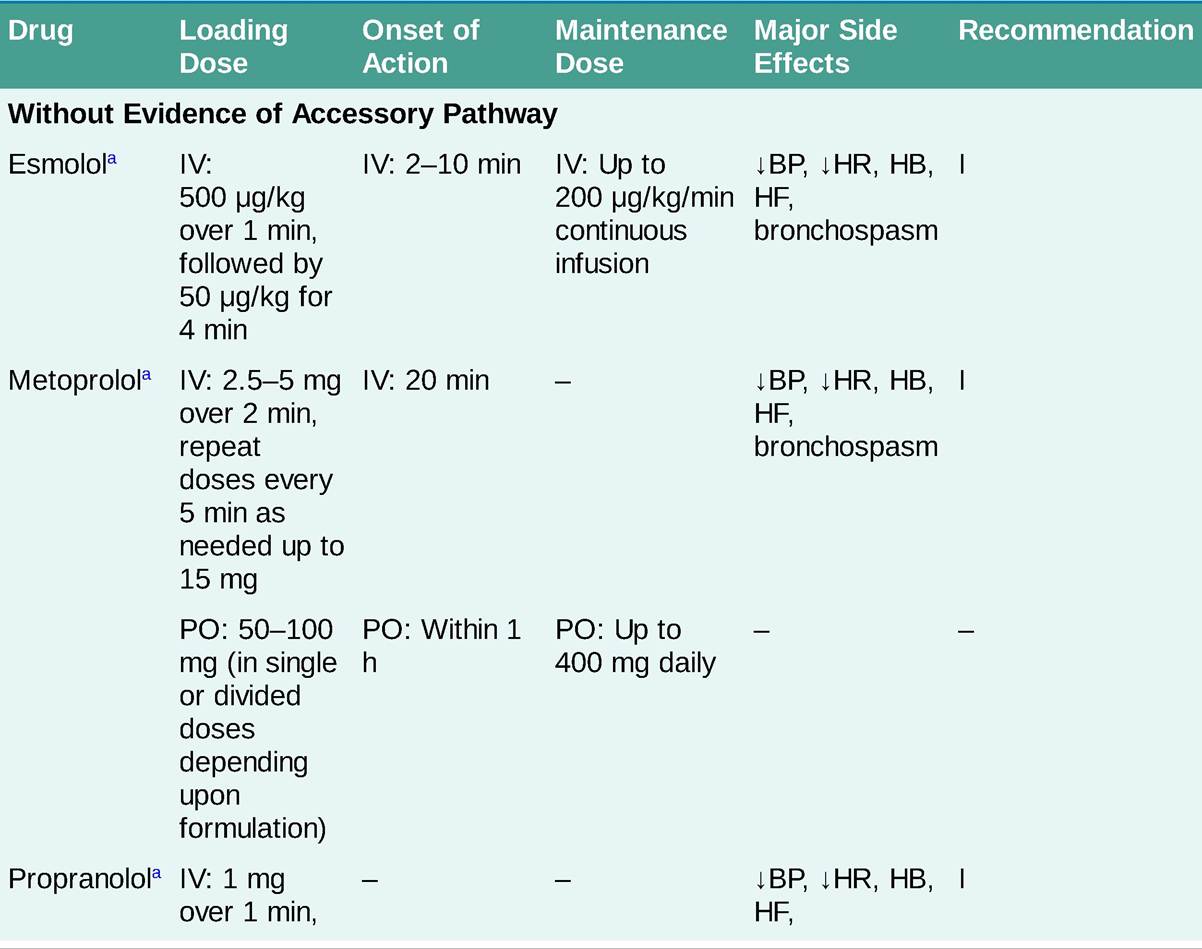
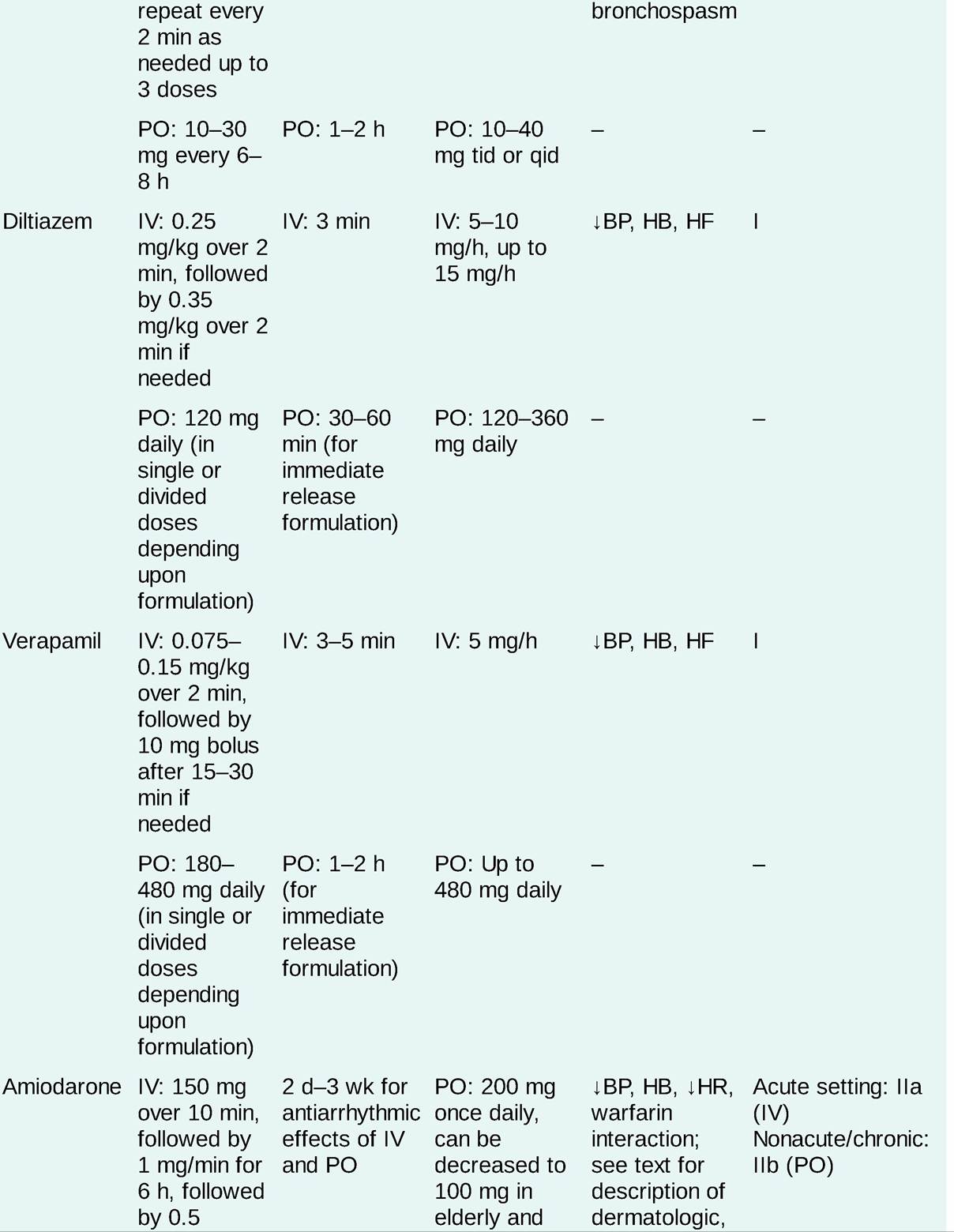
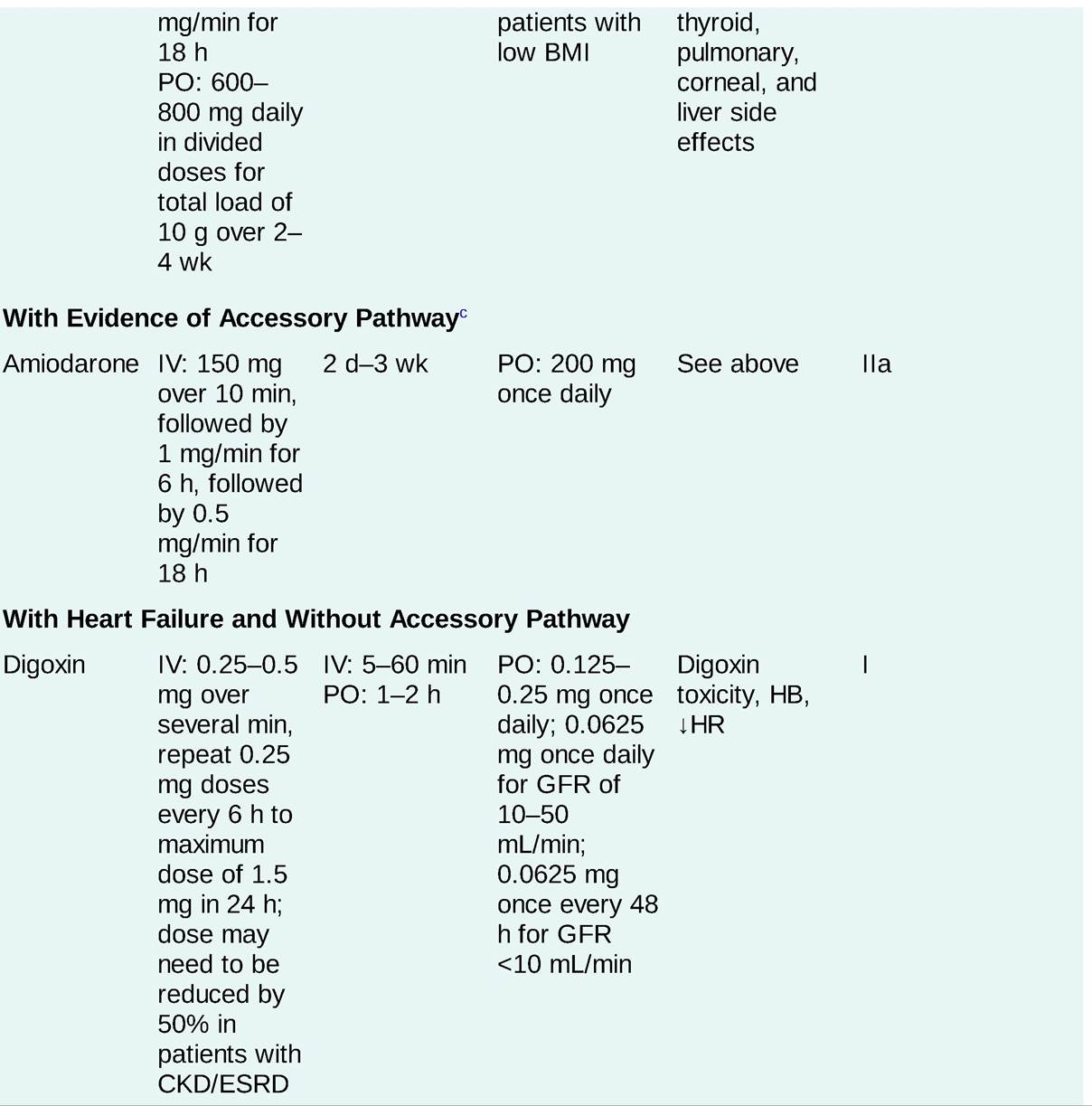
TABLE 7-3
PHARMACOLOGIC AGENTS USED FOR HEART RATE CONTROL IN ATRIAL FIBRILLATION
![]()
![]()
![]()
BMI, body mass index; J.BP, hypotension; CKD, chronic kidney disease; ESRD, end-stage renal disease; GFR, glomerular filtration rate; HB, heart block; HF, heart failure; ιHR, bradycardia; NA, not applicable.
aOnly representative β-blockers are included in the table, but other similar agents could be used for this indication in appropriate doses.
bOnset is variable, and some effects occur earlier.
cConversion to sinus rhythm and catheter ablation of the accessory pathway are generally recommended; pharmacologic therapy for rate control may be appropriate therapy in certain patients. See text for discussion of atrial fibrillation in setting of preexcitation/Wolff-Parkinson-White syndrome.
dAmiodarone can be useful to control the heart rate in patients with atrial fibrillation when other measures are unsuccessful or contraindicated.
FIRST LINE
• Prevention of stroke and systemic emboli—central tenet of AF management is guided by individual risk assessment. Systemic anticoagulation with coumadin or DOAC attenuates risk of stroke or systemic emboli associated with AF.
• Use of oral anticoagulants requires careful risk-benefit analysis to identify patients who are at sufficient risk for thromboembolic events without significant risk of hemorrhagic complications.
î CHA2DS2-VASc score —validated risk stratification tool used in nonvalvular AF to predict stroke or systemic embolus risk based on the presence of following risk factors: CHF, HTN, age >65 or >75 years, diabetes mellitus, female gender, prior stroke or transient ischemic attack (TIA), and history of vascular disease (Table 7-4).11
TABLE 7-4
| ANNUAL STROKE RISK IN PATIENTS WITH NONVALVULAR ATRIAL FIBRILLATION NOT TREATED WITH ANTICOAGULATION ACCORDING TO THE CHA2DS2-VASC SCORE |
| CHA2DS2-VASc Score | Stroke Risk (%)a |
| 0 | 0 |
| 1 | 1.3 |
| 2 | 2.2 |
| 3 | 3.2 |
| 4 | 4.0 |
| 5 | 6.7 |
| 6 | 9.8 |
| 7 | 9.6 |
| 8 | 12.5 |
| 9 | 15.2 |
CHA2DS2-VASc, cardiac failure, hypertension, age 65-74 years or age >74 years (doubled), diabetes, female sex, stroke (doubled), and a history of vascular disease.
aThe adjusted stroke rate was derived from multivariate analysis assuming no aspirin usage.
° Antithrombotic therapy can be omitted in patients with a CHA2DS2-VASc score = 0.
î In patients with a CHA2DS2-VASc score of 1, no antithrombotic therapy or treatment with an oral anticoagulant or ASA may be considered.
î Systemic anticoagulation with coumadin or DOAC is recommended for male patients with a CHA2DS2-VASc risk of ≥2 and female patients with a CHA2DS2-VASc risk of ≥3 in women who have no contraindications for anticoagulation.
î DOACs are recommended over coumadin for DOAC-eligible patients.
î Measurement of renal function is critical to assess safety and dosing of certain DOACs in patients with CHA2DS2-VASc score of ≥2 and chronic kidney disease.
î For AF patients at risk for thromboembolism but unable to tolerate long-term anticoagulation, consideration can be given to percutaneous occlusion or surgical ligation of left atrial appendage (LAA).
î Role of antithrombotic therapy leading up to and after restoration of SR discussed in the context of cardioversion.
• Pharmacologic rate control of AF is achieved with drugs that prolong conduction through the AV node. Principally, these include the non-dihydropyridine calcium channel blockers (diltiazem, verapamil), β-adrenergic blockers, and digoxin. Refer to Table 7-3 for loading and dosing recommendations.
î Digoxin can be useful in controlling the resting ventricular rate in AF in the setting of LV dysfunction and CHF when other agents fail. Utility in other clinical settings is limited by reduced efficacy of rate control during exertion and significant concerns of toxicity.
■ Digitalis toxicity is characterized by nausea, abdominal pain, vision changes, confusion, and delirium. Patients with renal dysfunction are at risk for digitalis toxicity as are patients on agents known to increase digoxin levels (e.g., verapamil, diltiazem, erythromycin, cyclosporine).
■ Paroxysmal AT with varying degrees of AV block and bidirectional VT—most commonly seen arrhythmias in association with digitalis toxicity. Treatment is supportive (i.e., withholding drug, inserting temporary pacemaker for prolonged AV block, administering IV phenytoin for bidirectional VT).
• Nonpharmacologic rate control—accomplished by AV nodal ablation in association with PPM implantation. Strategy reserved for patients deemed to be in permanent AF, who have failed pharmacologic rate control, and in whom rhythm control is either ineffective or contraindicated.
SECOND LINE
Pharmacologic rhythm control of AF accomplished with antiarrhythmic drugs that modify impulse formation or propagation to prevent initiation of AF. Risk of thromboembolism associated with pharmacologic cardioversion should be considered before beginning antiarrhythmic drug therapy.
• Pharmacologic cardioversion should be performed in hospital setting with continuous ECG monitoring due to small risk of life-threatening tachy- or bradyarrhythmias.
î Ibutilide—only drug approved by US Food and Drug Administration for pharmacologic cardioversion. Clinical trials have shown a 45% conversion rate for AF and a 60% conversion rate for AFL.
î Ibutilide is associated with 4%-8% risk for torsades de pointes (TdP), especially in first 2-4 hours after administration. Because of this risk, patients must be monitored on telemetry with an external defibrillator immediately available during ibutilide infusion and for at least 4 hours after infusion. The risk for TdP is higher in patients with cardiomyopathy and CHF.
î Ibutilide is administered intravenously, at dosage of 1 mg (0.01 mg/kg if patient is 7 days in duration. For shorter duration episodes, dofetilide, sotalol, flecainide, and propafenone have some efficacy; amiodarone has limited efficacy to achieve pharmacologic cardioversion.
• Maintenance of NSR with antiarrhythmic agents is associated with small risk for life-threatening proarrhythmia. As a result, antiarrhythmic therapy should be reserved for patients who have symptomatic AF with or without adequate rate control. Commonly used antiarrhythmic agents, their major route of elimination, and dosing regimens are listed in Table 7-5. Most effective agents for maintenance of SR are flecainide, propafenone, sotalol, dofetilide, amiodarone, and dronedarone.
î Flecainide and propafenone
For maintenance of NSR in patients with structurally normal hearts.
TABLE 7-5
COMMONLY USED ANTIARRHYTHMIC DRUGS
| Class | Drug | Route of Administration (Elimination) | InitialZLoading Dose | Maintenance Dose | Major Adverse EffectsaZCommc |
| Ia | Procainamide | IV (R, H) PO (R, H) | 15-18 mg/kg at 20 mg/min 50 mg/kg/24 h, max: 5 g/24 h | 1-4 mg/min IR: 250-500 mg q3-6h SR: 500 mg q6h Procanbid: 1000-2500 mg q12h | GI, CNS, +ANA/SLE-like syndrome, fever, hematologic, anticholinergic. Follow QTc, seru procainamide (48 mg/L) and NAP levels (bgcolor=white> | PO: 800 mg/d | 0.5 mg/min | see text for |
| | | for 1 wk, then | 100-400 mg | description of |
| | | 600 mg/d for 1 | PO daily | dermatologic, |
| | | wk, then | | thyroid, pulmona |
| | | 400 mg/d for 1 | | corneal, and liver |
| | | wk | | effects |
| | | | | | | | | | | |
AMI, acute myocardial infarction; ANA, antinuclear antibodies; ιBP, hypotension; CNS, central nervous system; CHF, congestive heart failure; CrCl, creatinine clearance; ER, extended release; GI, gastrointestinal; H, hepatic; HA, headache; HB, heart block; HF, heart failure; !HR, bradycardia; IR, immediate release; NA, not applicable; NAPA, N- acetylprocainamide; R, renal; SLE, systemic lupus erythematosus; SR, sustained release; TdP, torsades de pointes; VT, ventricular tachycardia.
aEither common or life-threatening adverse effects of these medications are listed. This is not a comprehensive list of all possible adverse effects.
■ Associated with increased mortality rate in patients with structural heart disease.12
■ Potent negative inotropes that can provoke or exacerbate heart failure.
■ Prolong QRS duration as early manifestation of toxicity.
? Toxicity increases with heart rate because of preferential blockade of active sodium channels. Property is described as positive-use dependence.
? Exercise ECG used to give additional information about dose safety at higher heart rates.
? Flecainide should be used cautiously without concomitant dosing with AV nodal blocker because paradoxical increase in the ventricular rate may occur from drug-induced conversion of AF to AFL. Propafenone is less prone to this because of intrinsic β-adrenergic antagonism.
î Sotalol—mixture of stereoisomers (dl-)
■ d-sotalol is a potassium channel blocker, whereas l-sotalol is a β-antagonist. Side effects of the drug reflect both mechanisms of action.
■ dl-sotalol may result in QT interval prolongation leading to TdP as well as sinus bradycardia or AV conduction abnormalities.
■ Should not be used in patients with decompensated CHF (because of negative inotropic effect) or with a prolonged QT interval.
■ Initiation should be performed in an inpatient monitored setting.
■ Renal adjustment is necessary as sotalol is excreted by the kidneys.
î Dofetilide—pure potassium channel blocker.
■ Initiation of dofetilide should be done in an inpatient monitored setting due to increased risk of QT interval prolongation leading to TdP.
■ QT prolongation with sotalol or dofetilide is intensified by bradycardia, known as “reverse-use dependence.”
■ Contraindicated in patients with baseline corrected QT interval (QTc) >440 ms (or >500 ms with baseline bundle branch block).
■ Dosing is based on the creatinine clearance. A 12-lead ECG should be obtained before the first dose and 1-2 hours after each dose, thereafter. If QTc prolongs by 15% of baseline or exceeds 500 ms, 50% dosage reduction is indicated. If the QTc exceeds 500 ms after the second dose, dofetilide must be discontinued.
■ Several medications block renal secretion of dofetilide (verapamil, cimetidine, prochlorperazine, trimethoprim, megestrol, ketoconazole) and are contraindicated with the use of dofetilide.
■ Not associated with increased mortality in patients with LV dysfunction and does not cause conduction disturbances.
î Dronedarone—newest antiarrhythmic agent approved for management of AF.
■ Shares properties with Vaughan Williams classes I-IV antiarrhythmic drugs.
■ More effective than placebo but less effective than amiodarone at maintaining SR after cardioversion.
■ Incidence of proarrhythmia and organ toxicity low with dronedarone.
■ Trend toward increased mortality has been shown in patients with advanced heart failure symptoms; as such, it is contraindicated in this patient group.
■ Metabolized by the liver and should not be used in patients with significant hepatic dysfunction.
■ Can be used in patients with significant renal dysfunction.
î Amiodarone—most effective antiarrhythmic agent for maintenance of SR.
■ Because of extensive toxicity profile, should not be considered first-line agent for rhythm control of AF in patients in whom alternative antiarrhythmic can be safely used.
■ Low efficacy for acute conversion of AF, although conversion after several days of IV has been observed. Adverse effects of oral amiodarone are partially dose dependent and may occur in up to 75% of patients treated at high doses for 5 years. At lower doses (200-300 mg/d), adverse effects that require discontinuation occur in approximately 5%-10% of patients per year.
■ Pulmonary toxicity in 1%-15% of treated patients but appears less likely in those who receive by one-half when amiodarone is initiated, and levels followed closely.
Nonpharmacologic Therapies
• Nonpharmacologic methods of rhythm control include electrical cardioversion, catheter ablation, or surgical techniques that block initiation and maintenance of AF.
• Direct current cardioversion (DCCV)—safest and most effective method of acutely restoring SR. Prior to cardioversion:
î Consideration of anticoagulation is critical, to minimize thromboembolic events triggered by the cardioversion process.
î AF with RVR in setting of ongoing myocardial ischemia, MI, hypotension, or respiratory distress should receive prompt cardioversion regardless of the anticoagulation status.
î If duration of AF is 48 hours (or for unknown duration), patients should be therapeutically anticoagulated for at least 3 weeks before cardioversion (elective situation), and anticoagulation should be continued following successful cardioversion for a minimum of 4 weeks.
î Alternative to anticoagulation for 3 weeks prior to cardioversion is to perform transesophageal echocardiogram to rule out LAA thrombus before cardioversion. This method is safe and has advantage of shorter time to cardioversion. Therapeutic anticoagulation is indicated after cardioversion for minimum of 4 weeks.14
î When practical, periprocedural sedation is accomplished with midazolam (1-2 mg IV q2min to a maximum of 5 mg), methohexital (25-75 mg IV), etomidate (0.2-0.6 mg/kg IV), or propofol (initial dose, 5 mg/kg/h IV).
î Proper synchronization of DC shock to the QRS is critical to avoid induction of VT by shock delivered during vulnerable period of the ventricle.
î For cardioversion of atrial arrhythmias, anterior patch electrode should be positioned just right of the sternum at the level of third or fourth intercostal space, with second electrode positioned just below left scapula posteriorly. Care should be taken to position patch electrodes at least 6 cm from PPM or implantable cardioverter-defibrillator (ICD) generators. If electrode paddles are used, firm pressure and conductive gel should be applied to minimize contact impedance. Direct contact with the patient or the bed should be avoided. Atropine (1 mg IV) should be readily available to treat prolonged pauses. Reports of serious arrhythmias, such as VT, ventricular fibrillation (VF), or asystole are rare and more likely in setting of improperly synchronized cardioversions, digitalis toxicity, or concomitant antiarrhythmic drug therapy.
• Catheter ablation of AF—highly effective in younger patients with structurally normal hearts and paroxysmal pattern of AF.6
î Success rates in this cohort are in the range of 70%-80% over 12-18 months follow-up period.
î Success rates are diminished in patients with structural heart disease, advanced age, and persistent AF. A significant fraction of patients require more than one ablation procedure to achieve long-term successful elimination of AF.
î Goal of catheter ablation in paroxysmal AF patients is to achieve electrical isolation of the pulmonary veins. In patients with persistent AF, this goal is frequently combined with substrate modification strategies whereby regions of the atria are targeted for ablation to block reentry or the presence of focal drivers of AF.
Surgical Management
Surgical techniques for cure of AF have been evaluated since the 1980s. Among these, the Cox maze procedure has highest demonstrated efficacy and most robust follow-up data documenting sustained efficacy. Including patients with persistent AF and structural heart disease, success rates approach 90%. Because of its invasive nature, surgical treatment is usually reserved for those who have failed catheter ablation or who have planned concomitant cardiac surgery.6