Bradyarrhythmias
GENERAL PRINCIPLES
• Bradyarrhythmias can be encountered in both the inpatient and outpatient settings.
• Clinical decision-making is guided by patient symptoms and signs of hemodynamic stability.
Definition
Cardiac rhythms whose ventricular rate is below 60 bpm.
• Anatomy of the conduction system
î The SA node—collection of specialized pacemaker cells located in high right atrium. Under normal conditions, a wave of depolarization spreads inferiorly and leftward via atrial myocardium and intranodal tracts, producing atrial systole.
î Wave of depolarization then reaches another group of specialized cells, the AV node, located in the lower right atrial side of the interatrial septum. Normally, AV node should serve as lone electrical connection between the atria and ventricles.
î From the AV node, wave of depolarization travels down the His bundle, located in the membranous septum, and into right and left bundle branches before reaching the Purkinje fibers that depolarize the remaining ventricular myocardium.
Etiology
Common causes of bradycardia are listed in Table 7-6.
TABLE 7-6
CAUSES OF BRADYCARDIA
Intrinsic
Congenital disease (may present later in life)
Idiopathic degeneration (aging)
Infarction or ischemia
Cardiomyopathy
Infiltrative disease: sarcoidosis, amyloidosis, hemochromatosis
Collagen vascular diseases: systemic lupus erythematosus, rheumatoid arthritis, scleroderma
Surgical trauma: valve surgery, transplantation
Infectious disease: endocarditis, Lyme disease, Chagas disease
Extrinsic
Autonomically mediated
Neurocardiogenic syncope
Carotid sinus hypersensitivity
Increased vagal tone: coughing, vomiting, micturition, defecation, intubation Drugs: β-blockers, calcium channel blockers, digoxin, antiarrhythmic agents Hypothyroidism
Hypothermia
Neurologic disorders: increased intracranial pressure
Electrolyte imbalances: hyperkalemia, hypermagnesemia HypercarbiaZobstructive sleep apnea
Sepsis
DIAGNOSIS
Clinical Presentation
• When evaluating suspected bradyarrhythmia, history, physical examination, and available data should be used to address stability, symptoms, reversibility, site of dysfunction, and the need for temporary as well as permanent pacing.
• If patient demonstrates signs of poor perfusion (hypotension, confusion, decreased consciousness, cyanosis, etc.), immediate management per ACLS protocol should be initiated. Clinical manifestations of bradyarrhythmias are variable, ranging from asymptomatic to nonspecific (lightheadedness, fatigue, weakness, exercise intolerance) to overt (syncope).
• Emphasis should be placed on determining if presenting symptoms have a direct temporal relationship to underlying bradycardia. Other historical points of emphasis include the following:
î Ischemic heart disease, particularly involving right coronary circulation, can precipitate a number of bradyarrhythmias. Therefore, signs and symptoms of acute coronary syndrome should be thoroughly investigated.
î Precipitating circumstances (micturition, coughing, defecation, noxious smells) surrounding episodes may help identify neurocardiogenic etiology of bradycardia.
î Tachyarrhythmias, particularly in patients with underlying sinus node dysfunction, can be followed by long pauses (conversion pauses) because of sinus node suppression during tachycardia.
î History of structural heart disease, hypothyroidism, OSA, collagen vascular disease, infections (bacteremia, endocarditis, Lyme, Chagas), infiltrative diseases (amyloid, hemochromatosis, and sarcoid), neuromuscular diseases, and prior cardiac surgery (valve replacement, congenital repair) should be elicited.
î Medications should be reviewed with emphasis on those that affect the SA and AV nodes (i.e., calcium channel blockers, β-adrenergic blockers, digoxin).
• After hemodynamic stability is confirmed, a more thorough examination with emphasis on the cardiovascular system and any findings consistent with the above comorbidities is appropriate (Figure 7-3).
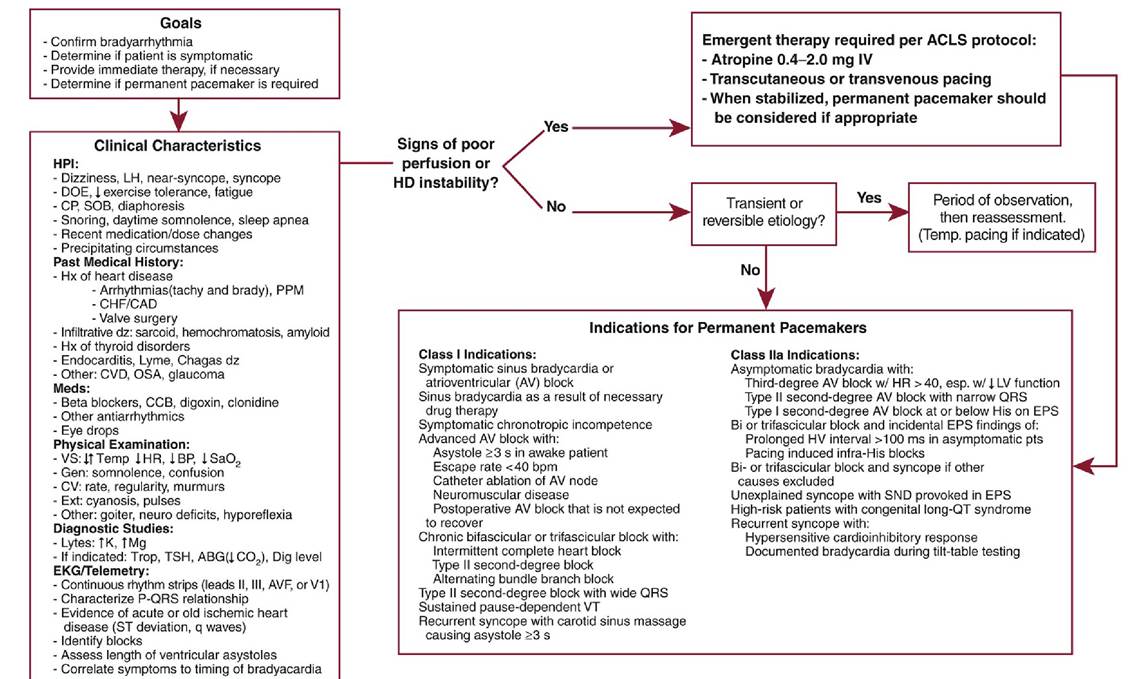
Figure 7-3 Approach to bradyarrhythmias.ABG, arterial blood gas; ACLS, advanced cardiac life support; tBP, hypotension; CAD, coronary artery disease; CCB, calcium channel blocker; CHF, congestive heart failure; CP, chest pain; CVD, cerebrovascular disease; DOE, dyspnea on exertion; dz, disease; EPS, electrophysiologic study; HD, hemodynamic; HPI, history of present illness; tHR, bradycardia; Hx, history; ↑K, hyperkalemia; LH, lightheadedness; ↑Mg, hypermagnesemia; OSA, obstructive sleep apnea; PPM, permanent pacemaker; lSaO2, hypoxia; SND, sinus node dysfunction; SOB, shortness of breath; TSH, thyroid-stimulating hormone; VS, vital signs; VT, ventricular tachycardia.(Reprinted with permission from Fansler D, Chen J.
Bradyarrhythmias and permanent pacemakers. In: Cuculich PS, Kates AM, eds. The Washington Manual Cardiology Subspecialty Consult. 3rd ed. Lippincott, Williams & Wilkins; 2014.)Diagnostic Testing
LABORATORIES
The laboratory testing should include serum electrolytes and thyroid function tests in most patients. Digoxin levels and serial troponins should be drawn when clinically appropriate.
ELECTROCARDIOGRAPHY
• A 12-lead ECG is the cornerstone for diagnosis in any workup where arrhythmia is suspected.
• Rhythm strips from leads that provide best view of atrial activity (II, III, aVF, or V1) should be examined closely.
• Emphasis should be placed on identifying evidence of SA node dysfunction (P wave intervals) or AV conduction abnormalities (PR interval).
SPECIAL CONSIDERATIONS
• Episodes of bradycardia are often transient and episodic; therefore, a baseline ECG may not be sufficient to capture bradycardia. Some form of continuous monitoring can be required.
î In inpatient setting, continuous central telemetry monitoring can be used.
î If further workup is done as an outpatient, short-term Holter monitoring can be used if the episodes occur somewhat frequently. If infrequent, an event recorder or ILR should be considered.
î Vital to correlate symptoms with rhythm disturbances discovered via continuous monitoring. Importance of accurate symptom diaries in ambulatory setting should be emphasized to patients.
• To evaluate sinus node response to exertion (chronotropic competence), walking the patient under supervision is easy and inexpensive. Formal exercise ECG can be ordered, if necessary.
• EPS can be used to assess sinus node function and AV conduction but is rarely necessary if rhythm is already diagnosed by noninvasive modalities.
DIFFERENTIAL DIAGNOSIS
• Sinus node dysfunction, or sick sinus syndrome (SSS), represents most common reason for pacemaker implantation in the US. Manifestations of SSS include the following (Figure 7-4):
î Sinus bradycardia—regular rhythm with QRS complexes preceded by “-sinus” P waves (upright in II, III, aVF) at a rate of the sinus node leading to the observed pauses.
D, Tachy-brady syndrome. Note the termination of the irregular tachyarrhythmia followed by a prolonged 4.5-second pause prior to the first sinus beat.(Reprinted with permission from Fansler D, Chen J. Bradyarrhythmias and permanent pacemakers. In: Cuculich PS, Kates AM, eds. The Washington Manual Cardiology Subspecialty Consult. 3rd ed. Lippincott, Williams & Wilkins; 2014.)î Sinus arrest and sinus pauses—failure of sinus node to depolarize; manifests as periods of atrial asystole (no P waves). May be accompanied by ventricular asystole or escape beats from junctional tissue or ventricular myocardium. Pauses of 2-3 seconds can be found in healthy, asymptomatic people, especially during sleep. Pauses >3 seconds, particularly during daytime hours, raise concern for sinus node dysfunction.
î Sinus exit block—appropriate firing of sinus node, but wave of depolarization fails to traverse past perinodal tissue. Indistinguishable from sinus arrest on surface ECGs except that the RR interval will be a multiple of RR preceding the bradycardia.
î Tachy-brady syndrome —when tachyarrhythmias alternate with bradyarrhythmias. Can be seen in conjunction with a number of types of SVT but is most commonly noted in patients with paroxysmal AF.
î Chronotropic incompetence—inability to increase the heart rate appropriately in response to metabolic need. Usually determined by exercising patients.
• AV conduction disturbances
î AV conduction can be diverted (fascicular or bundle branch blocks); delayed (first-degree AV block); occasionally interrupted (second-degree AV block); frequently, but not always, interrupted (advanced or high-degree AV block); or completely absent (third-degree AV block). Assignment of the bradyarrhythmia under investigation to one of these categories determines prognosis and guides therapy.
î First-degree AV block—conduction delay that results in PR interval >200 ms on surface ECG.
î Second-degree AV block—periodic interruptions (i.e., “dropped beats”) in AV conduction.
Distinction between Mobitz I and II is important because entities possess differing natural rates of progression to complete heart block.■ Mobitz type I block (Wenckebach)—progressive delay in AV conduction with successive atrial impulses until an impulse fails to conduct. On ECG, classic Wenckebach block manifests as follows:
? Progressive prolongation of PR interval of each successive beat before dropped beat.
? Shortening of each subsequent RR interval before dropped beat.
? A regularly irregular grouping of QRS complexes (group beating).
? Type I block usually within the AV node and portends more benign history with progression to complete heart block unlikely.
? Mobitz type II block carries less favorable long-term prognosis and is characterized by abrupt AV conduction block without evidence of progressive conduction delay.
? On ECG, PR intervals remain unchanged preceding nonconducted P wave.
? Presence of type II block, particularly if bundle branch block is present, often antedates progression to complete heart block.
■ Presence of 2:1 AV block makes differentiation between Mobitz type I and II mechanisms difficult. Diagnostic clues to the site of block include the following:
? Concomitant first-degree AV block, periodic AV Wenckebach, or improved conduction (1:1) with enhanced sinus rates or sympathetic input suggests more proximal interruption of conduction (i.e., Mobitz type I mechanism).
? Concomitant bundle branch block, fascicular block, or worsened conduction (3:1, 4:1, etc.) with enhanced sympathetic input localizes site of block more distally (Mobitz type II mechanism).
î Third-degree (complete) AV block—all atrial impulses fail to conduct to ventricles. Complete dissociation between the atria and ventricles (“A > V” rates). Should be distinguished from dissociation with competition at AV node (“V > A” rates).
î Advanced or high-degree AV block—more than one consecutive atrial depolarization fails to conduct to the ventricles (i.e., 3:1 block or greater).
On ECG, consecutive P waves seen without associated QRS complexes. However, there will be demonstrable P:QRS conduction somewhere on the record to avoid a “third-degree” designation (Figure 7-5).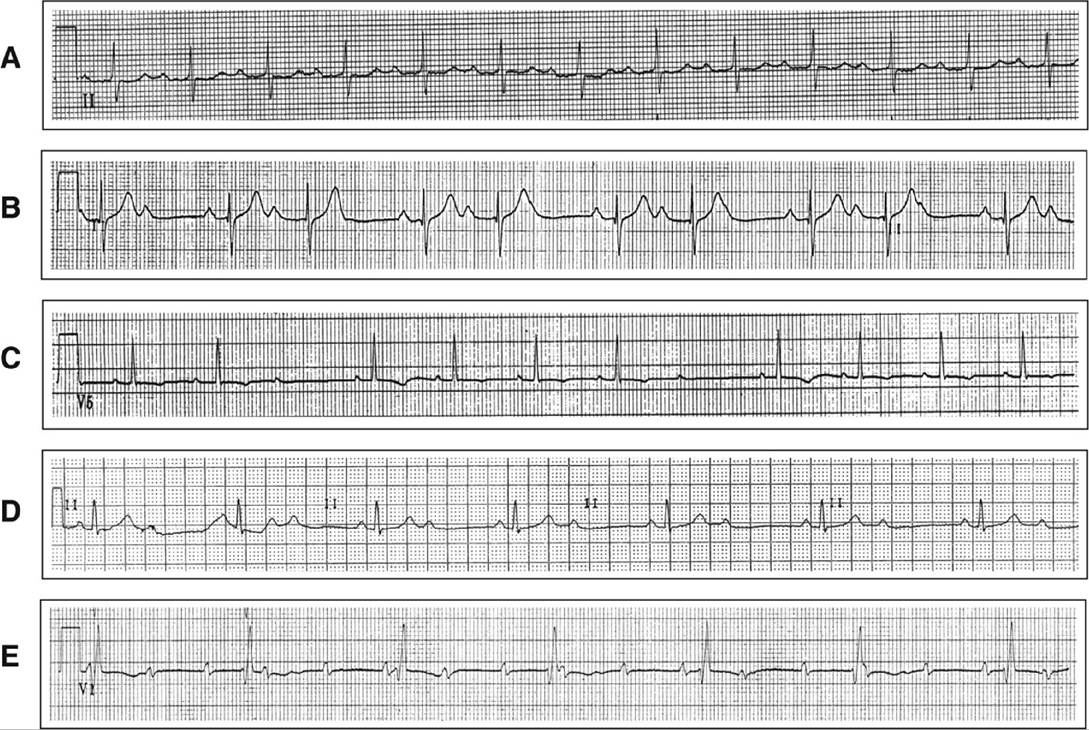
Figure 7-5 Examples of atrioventricular block (AVB).A, First-degree AVB. There are no dropped beats, and the PR interval is >200 ms. B, 3:2 second-degree AVB—Mobitz I. Note the “group beating” and the prolonging PR interval prior to the dropped beat. The third P wave in the sequence is subtly inscribed in the T wave of the preceding beat. C, Second-degree AVB—Mobitz II. Note the abrupt atrioventricular conduction block without evidence of progressive conduction delay. D, 2:1 AVB. This pattern makes it difficult to distinguish between Mobitz I versus II type mechanisms of block. Note the narrow QRS complex, which supports a more proximal origin of block (type I mechanism). A wider QRS (concomitant bundle branch or fascicular block) would suggest a type II mechanism. E, Complete heart block. Note the independent regularity of both the atrial and ventricular rhythms (junctional escape) with no clear association with each other throughout the rhythm strip.(Reprinted with permission from Fansler D, Chen J. Bradyarrhythmias and permanent pacemakers. In: Cuculich PS, Kates AM, eds. The Washington Manual Cardiology Subspecialty Consult. 3rd ed. Lippincott, Williams & Wilkins; 2014.)
IMAGING
• Presence or absence of structural heart disease should be initially evaluated by TTE.
• Further imaging should be obtained based on suspected etiology.
TREATMENT
Pharmacologic Therapy
• Bradyarrhythmias leading to significant symptoms and hemodynamic instability should be managed emergently as outlined in ACLS guidelines (see Appendix C).
• Atropine, an anticholinergic agent given in doses of 0.5-2.0 mg IV is cornerstone pharmacologic agent for emergent bradycardia treatment.
î Dysfunction localized more proximally in conduction system (i.e., symptomatic sinus bradycardia, first-degree AV block, Mobitz I second-degree AV block) tends to be responsive to atropine.
î Distal disease is not responsive and can be worsened by atropine.
î Reversible causes of bradyarrhythmias should be identified, and any agents (digoxin, calcium channel blockers, β-adrenergic blockers) that caused or exacerbated the underlying dysrhythmia should be withheld.
Nonpharmacologic Therapies
• For bradyarrhythmias that have irreversible etiologies or that are secondary to medically necessary pharmacologic therapy, pacemaker therapy should be considered.
î Temporary pacing indicated for symptomatic second- or third-degree heart block caused by transient drug intoxication or electrolyte imbalance and complete heart block or Mobitz II second-degree AV block in the setting of an acute MI.
î Sinus bradycardia, AF with a slow ventricular response, or Mobitz I second-degree AV block should be treated with temporary pacing only if significant symptoms or hemodynamic instability is present.
î Temporary pacing is achieved preferably via insertion of a TVP. Transthoracic external pacing can be used, although the lack of reliability of capture and patient discomfort make this a second-line modality.
• Once hemodynamic stability has been established, attention turns to the indications for PPM placement. î In symptomatic patients, key determinants include potential reversibility of causative factors and
temporal correlation of symptoms to the arrhythmia.
î In asymptomatic patients, key determinant based on whether discovered conduction abnormality has natural history of progression to higher degrees of heart block that portends poor prognosis.
• Permanent pacing
î Permanent pacing involves placement of anchored, intracardiac pacing leads for the purpose of maintaining heart rate sufficient to avoid symptoms and hemodynamic instability. Current devices, through maintenance of AV synchrony and rate-adaptive programming, more closely mimic normal physiologic heart rate behavior.
■ Class I and IIa indications for permanent pacing are listed in Figure 7-3.
■ Pacemakers are designed to provide an electrical stimulus to the heart whenever the rate drops below a preprogrammed lower rate limit. Therefore, the ECG appearance of a PPM varies depending on the heart rate and state of AV conduction.
■ Pacing spikes produced by modern pacemakers are low amplitude, sharp, and immediately preceding the generated P wave or QRS complex indicating capture of the chamber. Figure 7-6 illustrates some common ECG appearances of normally and abnormally functioning pacemakers.
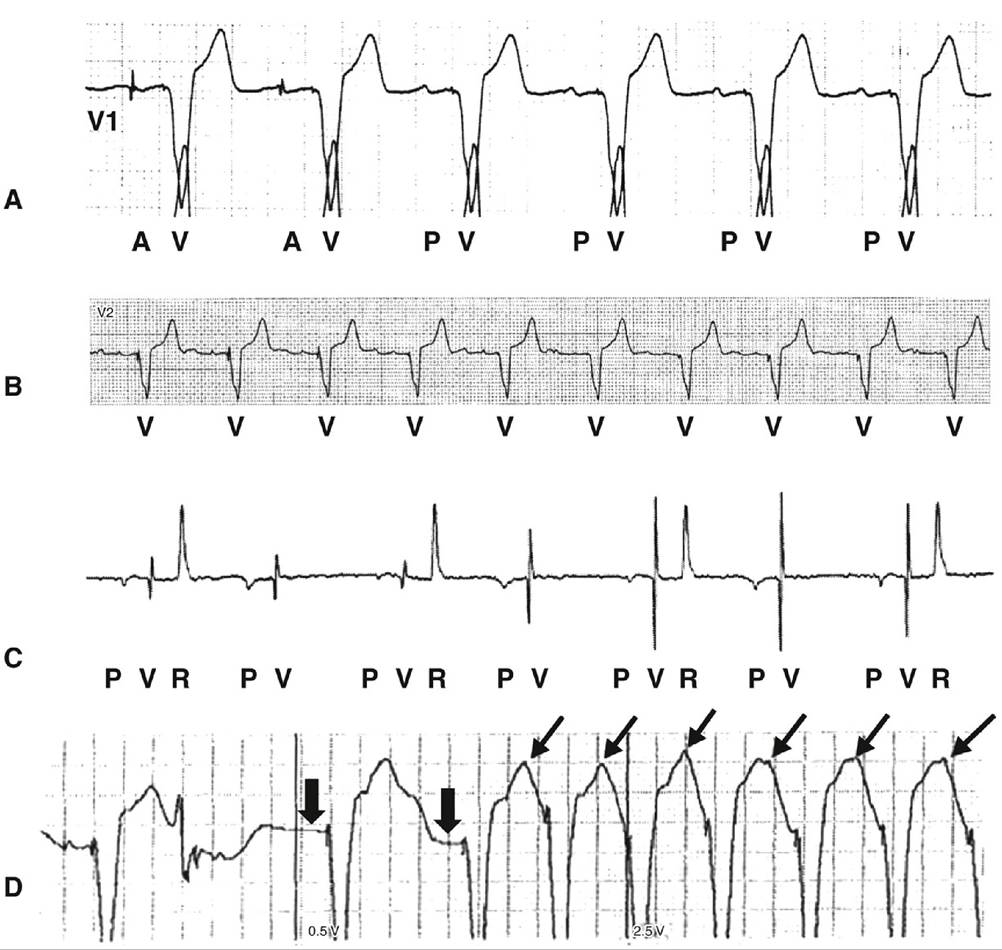
Figure 7-6 Pacemaker rhythms.A, Normal dual-chamber device (DDD) pacing. First two complexes are atrioventricular (AV) sequential pacing, followed by sinus with atrial sensing and ventricular pacing. B, Normal singlechamber (VVI) pacing. The underlying rhythm is atrial fibrillation (no distinct P waves), with ventricular pacing at 60 bpm. C, Pacemaker malfunction. The underlying rhythm is sinus (P) at 80 bpm with 2:1 heart block and first-degree AV block (long PR). Ventricular pacing spikes are seen (V) after each P wave, demonstrating appropriate sensing and tracking of the P waves; however, there is failure to capture. D, Pacemaker-mediated tachycardia. A, paced atrial events; P, sensed atrial events; R, sensed ventricular events; V, paced ventricular events.(Reprinted with permission from Fansler D, Chen J. Bradyarrhythmias and permanent pacemakers. In: Cuculich PS, Kates AM, eds. The Washington Manual Cardiology Subspecialty Consult. 3rd ed. Lippincott, Williams & Wilkins; 2014.)
î Pacemaker generator is commonly placed subcutaneously in pectoral region on the side of the nondominant arm. The electronic lead(s) is/are placed in the cardiac chamber(s) via central veins. Complications of placement include pneumothorax, device infection, bleeding, and, rarely, cardiac perforation with tamponade.
■ Before implantation, patient must be free of any active infections, and anticoagulation issues must be carefully considered. Hematomas in the pacemaker pocket develop most commonly in patients who are receiving IV heparin or SC low-molecular-weight heparin.
■ Following implant, posteroanterior and lateral CXR are obtained to confirm appropriate lead placement. Pacemaker is interrogated at appropriate intervals—typically, before discharge, 2-6 weeks following implantation, and every 6-12 months thereafter.
î Pacing modes—classified by sequence of three to five letters. Most pacemakers are referred to by the three-letter code alone.
■ Position I denotes the chamber that is paced: A for atria, V for ventricle, or D for dual (A + V).
■ Position II refers to the chamber that is sensed: A for atria, V for ventricle, D for dual (A + V), or O for none.
■ Position III denotes the type of response the pacemaker will have to a sensed signal: I for inhibition, T for triggering, D for dual (I + T), or O for none.
■ Position IV is used to signify the presence of rate-adaptive pacing (R) in response to increased metabolic need.
î The most common pacing systems used today include VVI, DDD, or AAI.
■ AAI systems used only for sinus node dysfunction in the absence of any AV conduction abnormalities.
■ Presence of AV nodal or His-Purkinje disease makes a dual-chamber device (i.e., DDD) more appropriate.
■ Patients in permanent AF warrant a single ventricular lead with VVI programming.
î Modern-day pacemakers also have the capability of mode switching.
■ Useful in patients with DDD pacers who have concurrent paroxysmal atrial tachyarrhythmias. When an atrial arrhythmia faster than a programmed mode switch rate develops, the device will change to a mode (i.e., VVI) that does not track atrial signals. It will return to DDD when the tachyarrhythmia resolves.
■ Another common mode switch setting is used in patients with low-grade or intermittent high-grade AV conduction disease to minimize ventricular pacing. The device will attempt to stay in AAI and switch to DDD only when conduction through the AV node fails. This allows for preferential conduction to the ventricles through the native conduction system as much as possible and reduces the chance for pacemaker-mediated cardiomyopathy.
î Although infrequent, pacemaker malfunction is potentially life-threatening, particularly for patients who are pacemaker dependent. The workup of suspected malfunction should begin with a 12-lead ECG.
■ If no pacing activity is seen, place a magnet over the pacemaker to assess for output failure and ability to capture. Application of the magnet switches the pacemaker to an asynchronous pacing mode. For example, VVI mode becomes VOO (ventricular asynchronous pacing) and DDD mode becomes DOO (asynchronous AV pacing).
■ If malfunction is obvious or if the ECG is unrevealing and malfunction is still suspected, then formal interrogation of the device should be performed. Patients are given a card on implantation that will identify the make and model of the device to facilitate this evaluation.
■ Two view CXR should also be obtained to assess for evidence of overt lead abnormalities (dislodgement, fracture, migration, etc.).
î General categories of pacemaker malfunction include failure to pace (output failure), failure to capture, failure to sense (undersensing), and pacemaker-mediated dysrhythmias.
More on the topic Bradyarrhythmias:
- Transplacental therapy
- Macrovascular Complications of Diabetes Mellitus
- Cardiopulmonary Resuscitation
- Index
- INDEX
- Oncologic Emergencies