Syncope
GENERAL PRINCIPLES
Syncope is a common clinical problem. Primary goal of evaluation is to determine whether the patient is at increased risk of SCD.
Definition
Sudden, self-limited loss of consciousness and postural tone caused by transient global cerebral hypoperfusion, followed by spontaneous, complete, and prompt recovery.
Classification
Four major categories based on etiology28
• Neurocardiogenic (most common): vasovagal, carotid sinus hypersensitivity, and situational.
• Orthostatic hypotension: hypovolemia, medication-induced (iatrogenic), and autonomic dysfunction.
• Cardiovascular
î Arrhythmogenic: sinus node dysfunction, AV block, pacemaker malfunction, VT/VF, SVT (rare).
î Mechanical: HCM, valvular stenosis, aortic dissection, myxomas, pulmonary embolism, pulmonary HTN, acute MI, subclavian steal, etc.
• Miscellaneous (not true syncope): seizures, stroke/TIA, hypoglycemia, hypoxia, psychogenic, etc.
° Atherosclerotic cerebral artery disease is a rare cause of true syncope; the exception is severe obstructive four-vessel cerebrovascular disease (expect focal neurologic findings prior to syncope).
Epidemiology
• Common in general population: 6% of medical admissions and 3% of emergency room visits.29
• Incidence is similar among men and women; one of the largest epidemiologic studies revealed an 11% incidence during an average follow-up of 17 years, with sharp rise after age 70 years.29
Pathophysiology
• Two components of neUrocardiogenic syncope are described as cardioinhibitory, in which bradycardia or asystole results from increased vagal outflow to the heart, and vasodepression, where peripheral vasodilation results from sympathetic withdrawal to peripheral arteries. Most patients have a combination of both components as mechanism.
• Specific stimuli (e.g., micturition, defecation, coughing, swallowing) may evoke a neurocardiogenic mechanism, leading to situational syncope.
Risk Factors
• Cardiovascular disease, history of stroke or TIA, and HTN have been shown to predispose patients to syncope.30
• Low body mass index (BMI), increased alcohol intake, and diabetes are also associated with syncope.30
DIAGNOSIS
Clinical Presentation
HISTORY
• Meticulous history and physical examination are vital to accurate diagnosis of etiology of syncope. In
40% of episodes, the mechanism of syncope remains unexplained.31,32
• Special attention should be focused on symptoms that precede and follow syncopal episode, eyewitness accounts during the event, time course of loss and resumption of consciousness (abrupt vs. gradual), and patient's medical history.
• Characteristic prodrome of nausea, diaphoresis, visual changes, or flushing suggests neurocardiogenic syncope.
î Identification of emotional or situational trigger and post-episode fatigue are also clues to neurocardiogenic/situational cause of syncope.
• Alternatively, unusual sensory prodrome, incontinence, or a decreased level of consciousness that gradually clears suggests a seizure as a likely diagnosis.
• With transient ventricular arrhythmias, abrupt loss of consciousness with rapid recovery may occur.
• Syncope with exertion concerning for structural heart disease, pulmonary HTN, and/or CAD.
PHYSICAL EXAMINATION
• Cardiovascular and neurologic examinations are primary focus of initial evaluation.
• Orthostatic vital signs aid in the diagnosis of orthostatic hypotension. Patients should have blood pressure checked in both arms.
• Cardiac examination findings may detect valvular heart disease, LV dysfunction, pulmonary HTN, etc.
• Neurologic findings are often absent but, if present, may point to a neurologic etiology.
• Carotid sinus massage for 5-10 seconds with reproduction of symptoms and consequent ventricular pause >3 seconds is considered positive for carotid sinus hypersensitivity. Take proper precautions of telemetry monitoring, availability of bradycardia treatments, and avoidance of the maneuver in patients with known or suspected carotid disease.
Diagnostic Testing
• Presence of known structural heart disease, abnormal ECG, age >65 years, focal neurologic findings, and severe orthostatic hypotension suggest more ominous etiology of a syncopal event.
These patients should be admitted for further workup to avoid delay and adverse outcomes.• After history and physical examination, ECG is the most important diagnostic tool in the evaluation of syncope. It will be abnormal in 50% of cases but alone will yield a diagnosis in only 5% of these patients.
• If no history of heart disease or baseline ECG abnormalities, tilt table testing has been used to evaluate hemodynamic response during transition from supine to an upright state to precipitate a neurocardiogenic response. In an unselected population, the predictive value of this test is low.
• Refer to Figure 7-7 for the diagnostic approach to syncope.
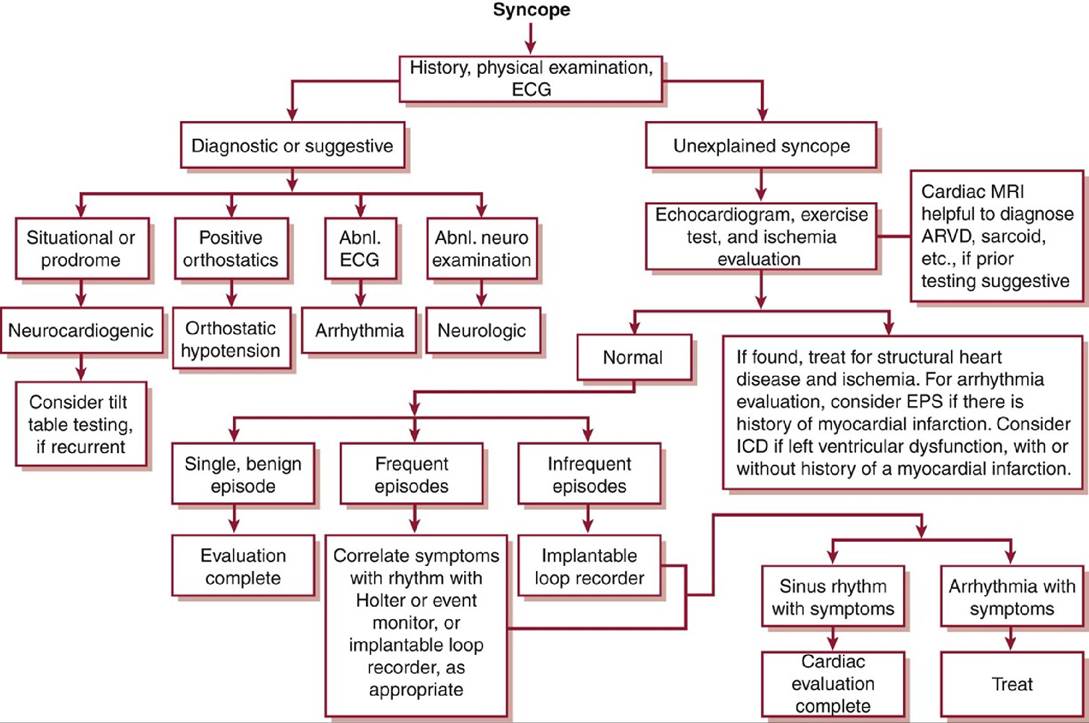
Figure 7-7 Algorithm for the evaluation of syncope.ARVD, arrhythmogenic right ventricular dysplasia; EPS, electrophysiology study; ICD, implantable cardioverter-defibrillator.(Modified from Strickberger SA, Benson DW, Biaggioni I, et al AHA/ACCF scientific statement on the evaluation of syncope from the American Heart Association Councils on Clinical Cardiology, Cardiovascular Nursing, Cardiovascular Disease in the Young, and Stroke, and the Quality of Care and Outcomes Research Interdisciplinary Working Group; and the American College of Cardiology Foundation in Collaboration with the Heart Rhythm Society. J Am Coll Cardiol. 2006;47(2):473-484. Copyright © 2006 American College of Cardiology Foundation. With permission.)
TREATMENT
• Therapy is tailored to the underlying etiology of syncope with goals of preventing recurrence and reducing risk of injury or death.
• Neurocardiogenic syncope
î Counsel patients to take steps to avoid injury by being aware of prodromal symptoms and maintaining a horizontal position at those times.
î Avoid known precipitants and maintain adequate hydration.
î Employ isometric muscle contraction during prodrome to abort a syncopal episode.
î Evidence suggests that β-adrenergic blockers are probably unhelpful; selective serotonin reuptake inhibitor antidepressants and fludrocortisone have debatable effect; midodrine (initiated at 5 mg PO tid and can be increased to 15 mg tid) is probably helpful in treatment of neurocardiogenic syncope.33-35
î In general, PPMs have no proven benefit in the management of neurocardiogenic syncope.
However, permanent dual-chamber pacemakers with hysteresis function (high-rate pacing in response to a detected sudden drop in heart rate) have been shown to be useful in highly selected patients withrecurrent neurocardiogenic syncope with a prominent Cardioinhibitory component.36
î Cardiac pacing for carotid sinus hypersensitivity is appropriate in syncopal patients.
î In general, neurocardiogenic syncope is not associated with increased risk of mortality.
• Orthostatic hypotension
î Adequate hydration and elimination of offending drugs.
î Salt supplementation, compressive stockings, and counseling on gradual position changes.
î Midodrine and fludrocortisone can help by increasing systolic BP and expanding plasma volume, respectively.
• Cardiovascular (arrhythmia or mechanical)
î Treatment of underlying disorder (valve replacement, antiarrhythmic agent, coronary revascularization, etc.)
î Cardiac pacing for sinus node dysfunction or high-degree AV block
î Discontinuation of QT-prolonging drugs
î Catheter ablation procedures in select patients with syncope associated with SVT
î ICD for documented VT without correctable cause and for syncope in the presence of significant LV dysfunction even in the absence of documented arrhythmia
More on the topic Syncope:
- Syncope
- Contraception
- Oncologic Emergencies
- I IMMUNIZATIONS ^446 ^485 ^633
- Macrovascular Complications of Diabetes Mellitus
- Treatment options: hormonal, non- hormonal, and others
- General aspects of antenatal care
- Mitral Stenosis
- Chapter 5 Maternal–Fetal Physiology
- Chapter 19 Ectopic Pregnancy and Abortion