Chapter 19 Ectopic Pregnancy and Abortion
This chapter deals primarily with APGO Educational Topic Area Areas:
TOPIC 15 ECTOPIC AREA PREGNANCY
TOPIC 16 SPONTANEOUS ABORTION
TOPIC 34 INDUCED ABORTION
Students should be able to outline a basic approach to evaluation and management of first-trimester bleeding.
They should be able to discuss the differential diagnosis, associated risk factors, etiologies, and complications. Finally, they should be able to counsel a patient about pregnancy options including medical and surgical terminations and associated complications. They should understand the public health impact of access to abortion.Clinical Case
A 25-year-old woman reports that she had a positive home pregnancy test last week and now has spotting and low abdominal pain of 2 days’ duration. Her last menstrual period was 6 weeks ago. Her abdomen is minimally tender in the left lower quadrant with no rebound tenderness. The pelvic examination is normal except for tenderness and a 4 cm mass in the left adnexa. Pelvic ultrasound shows an intact pregnancy consistent with her last period and a simple left ovarian cyst.
 ECTOPIC PREGNANCY
ECTOPIC PREGNANCY
An ectopic or extrauterine pregnancy is one in which the blastocyst implants anywhere other than the endometrial lining of the uterine cavity. Ectopic pregnancies account for approximately 1.5% of reported pregnancies in the United States. As shown in Figure 19.1, 98% of ectopic pregnancies implant in the fallopian tube, with 80% occurring in the ampullary segment. Other locations include, but are not limited to, the ovary, cervix, and abdomen.
In the past, ectopic pregnancy was life threatening. Currently, earlier diagnosis made possible by the ability to detect the β-subunit of human chorionic gonadotropin (hCG), combined with high-resolution transvaginal sonography (TVS), has reduced this threat.
Nevertheless, ectopic pregnancies remain an important cause of morbidity and mortality in the United States.Tubal Ectopic Pregnancy
Without intervention, the natural course of a tubal pregnancy will result in any of three outcomes: tubal abortion, tubal rupture, or spontaneous resolution. Tubal abortion is the expulsion of products of conception through the fimbriated end. This tissue can then either regress or reimplant in the abdominal cavity. Tubal rupture is associated with significant intra-abdominal hemorrhage, often necessitating surgical intervention.
Pathophysiology and Risk Factors
An appreciation of risk factors for ectopic pregnancy can lead to making a more timely diagnosis resulting in both improved maternal survival and future reproductive potential.
Inflammation resulting in tubal damage can disrupt the normal migration of a fertilized ovum through the tube, thereby predisposing to an ectopic pregnancy. Specific examples of an inflammatory process include salpingitis and salpingitis isthmica nodosa. An acute chlamydial infection causes intraluminal inflammation and subsequent fibrin deposition with tubal scarring. Despite negative cultures, persistent chlamydial antigens can trigger a delayed hypersensitivity reaction with continued scarring. Whereas endotoxin-producing Neisseria gonorrhoeae causes virulent pelvic inflammation with a rapid clinical onset, chlamydial inflammatory response is indolent and peaks at 7 to 14 days. The incidence of ectopic pregnancy has increased consistently with the rise in chlamydial infections.
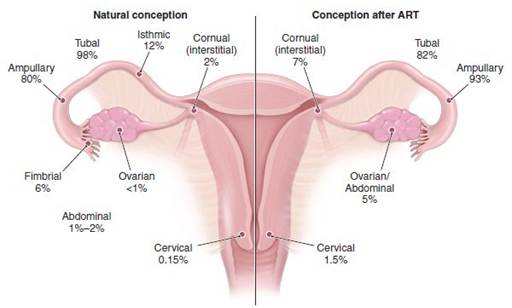
FIGURE 19.1. Incidence of types of ectopic pregnancy by location. ART, assisted reproductive technologies.
Pregnancy after tubal sterilization is rare, but, when it does occur, there is a substantial risk that the pregnancy will be ectopic due to the distorted tubal anatomy created by the tubal ligation. Previous concerns that intrauterine device use and elective pregnancy termination are predisposing risks for ectopic pregnancy have been dispelled.
A history of infertility, independent of tubal disease, and ovulation induction also appear to be risk factors in ectopic pregnancy. Additional risk factors include prior ectopic pregnancy, smoking, prior tubal surgery, diethylstilbestrol exposure, and advanced age.
Symptoms
With the availability of early pregnancy testing, the ability to diagnose ectopic pregnancy before rupture—even before the onset of symptoms—is not unusual. The classic symptoms associated with ectopic pregnancy are amenorrhea followed by vaginal bleeding and abdominal pain on the affected side; however, there is no constellation of symptoms that are diagnostic. Normal pregnancy symptoms, such as breast tenderness, nausea, and urinary frequency, may accompany more ominous findings. These include shoulder pain worsened by inspiration and caused by phrenic nerve irritation from subdiaphragmatic blood as well as vasomotor disturbances, such as vertigo and syncope from hemorrhagic hypovolemia.
As long as placental hormones are produced, there is usually no vaginal bleeding. Irregular vaginal bleeding results from the sloughing of the decidua from the endometrial lining. Vaginal bleeding in patients with an ectopic gestation may range from little or none to heavy, menstrual-like flow. In some patients, the entire “decidual cast” is passed intact, simulating a spontaneous abortion. Histologic evaluation of this tissue confirms whether placental villi are present. In any pregnant patient with no histopathologic confirmation of chorionic villi within the uterus, an ectopic implantation should be assumed to be present until proven otherwise.
Many women with a small unruptured ectopic pregnancy may have unremarkable clinical findings. Nevertheless, the diagnosis should be considered strongly when any of the above symptoms are reported by reproductive age women, especially those with risk factors for an extrauterine pregnancy.
Clinical Findings
Abdominal and pelvic findings are notoriously scant in many women before tubal rupture.
Prior to rupture, the diagnosis of an ectopic pregnancy is primarily based on laboratory and ultrasound findings. With rupture, however, nearly three fourths of women will have marked tenderness on both abdominal and pelvic examination, and pain is aggravated with cervical manipulation. A pelvic mass, including fullness posterolateral to the uterus, can be palpated in about 20% of women. Initially, the ectopic pregnancy may feel soft and elastic, whereas extensive hemorrhage produces a firmer consistency. Many times, discomfort precludes palpation of the mass. Not performing a pelvic examination may actually help avert iatrogenic rupture. Given the available technology and the natural course of an ectopic pregnancy, the role of physical examination in the diagnosis of this condition is minimal.Fever is not expected, although a mild elevation in temperature in response to intraperitoneal blood may occur. A temperature of 38°C may suggest an infectious cause of a patient’s symptoms. Abdominal distention and tenderness, with or without rebound, rigidity, or decreased bowel sounds may be seen in cases of intra-abdominal bleeding. Abdominal tenderness is present in 50% to 90% of patients with ectopic pregnancies. Cervical motion tenderness caused by intraperitoneal irritation and adnexal tenderness are commonly found. An adnexal mass is present in roughly one third of cases, but its absence does not rule out the possibility of an ectopic implantation. The uterus may enlarge and soften throughout the first trimester, thus simulating an intrauterine pregnancy. A slightly open cervix with blood or decidual tissue may be found and mistaken for a threatened and/or spontaneous abortion.
Differential Diagnosis
Symptoms of ectopic pregnancy can mimic multiple entities. Early pregnancy complications (threatened, incomplete, or missed abortion), placental polyp, and hemorrhagic corpus luteal cyst are difficult to differentiate from ectopic pregnancy. Since early bleeding occurs in up to 20% of women with normal, intact pregnancies, the physician must take care to avoid any action that might compromise a possible ongoing pregnancy.
A number of nonpregnancy-related disorders, such as appendicitis and renal calculi, can also mimic ectopic pregnancy.The rapid and accurate diagnosis of ectopic pregnancy is imperative to reduce the risk of serious complications or death. Up to half of the women who have died as a result of ectopic pregnancy had a lag in treatment because of delayed or inaccurate diagnoses. Any sexually active woman in the reproductive age group who presents with pain, irregular bleeding, and/or amenorrhea should have ectopic pregnancy as a part of the initial differential diagnosis.
Diagnostic Procedures
TVS and serial serum β-hCG measurements are the most valuable diagnostic aids to confirm a suspicion of ectopic pregnancy. The initial assessment in the otherwise hemodynamically stable patient must include a pregnancy test. A negative pregnancy test excludes the possibility of ectopic pregnancy. Urinary pregnancy tests, which detect hCG levels to 20 IU/L, are now commonly available. These tests detect hCG as early as 14 days after conception and are positive in more than 90% of cases of ectopic pregnancy. Serum assays can detect the presence of hCG as early as 5 days after conception, that is, before the missed menstrual cycle; however, because they require additional time and expertise to perform, they are often not utilized in a potentially emergent clinical setting.
Serum Human Chorionic Gonadotropin Levels
If a positive pregnancy test is found when ectopic pregnancy is suspected, the remainder of the workup should focus on evaluating the viability and location of the pregnancy. In normal pregnancies, serum β-hCG levels rise in a log-linear fashion until 60 or 80 days after the last menses, at which time levels plateau at about 100,000 IU/L. During this early phase of pregnancy, a 53% or greater increase in serum β-hCG levels should be observed every 48 hours. A rise of hCG levels less than this should raise suspicion for an abnormal gestation, either intrauterine or ectopic.
Complicating this scenario is the recognition that approximately 15% of normal intrauterine pregnancies are associated with less than a 53% increase in hCG, and 17% of ectopic pregnancies have normal hCG doubling times. Although inappropriately rising serum β-hCG levels suggest (but do not diagnose) an abnormal pregnancy, they do not identify its location.Transvaginal Ultrasonography
A key adjunct to serial quantitative levels of hCG is transvaginal pelvic ultrasonography (Fig. 19.2). Using TVS, a gestational sac is usually visible between 4½ and 5 weeks from the last menstrual period (LMP). The yolk sac appears between 5 and 6 weeks, and a fetal pole with cardiac activity is first detected at 5½ to 6 weeks. With transabdominal sonography, these structures are visualized slightly later. Each institution must define a β-hCG discriminatory value (i.e., the lower limit of serum hCG at which a TVS can reliably visualize pregnancy). It is not uncommon for TVS to demonstrate an intrauterine pregnancy by the time the hCG level is 1,000 to 2,000 IU/L. Transabdominal ultrasonography should be able to identify an intrauterine gestation by the time the hCG level reaches 5,000 to 6,000 IU/L. The absence of an intrauterine pregnancy with β-hCG levels above the discriminatory value signifies an abnormal pregnancy—ectopic, incomplete abortion, or resolving completed abortion. Care must be taken to differentiate between a uterine gestation and a pseudogestational sac. This one-layer sac is the result of an intracavitary fluid collection caused by sloughing of the decidua typically situated in the midline of the uterine cavity, whereas a normal gestational sac is eccentrically located (Fig. 19.3).

FIGURE 19.2. Ectopic pregnancy with an extrauterine gestational sac containing a live embryo. (A) Coronal transvaginal view of the right adnexa demonstrates an extrauterine sac (arrows) containing an embryo (calipers). (B) Sagittal transvaginal view of the uterus reveals no evidence of a gestational sac. (From Doubilet PM, Benson CB. Atlas of Ultrasound in Obstetrics and Gynecology. Philadelphia, PA: Lippincott Williams & Wilkins; 2003:319.)
Serum Progesterone Level
Serum progesterone concentration has also been used as a screening test for ectopic pregnancy. There is minimal variation in serum progesterone concentration between 5 and 10 weeks of gestation; thus a single value is sufficient. A serum progesterone level of 20 ng/mL has a sensitivity of 95%, with a specificity of approximately 40% to identify a healthy pregnancy. Serum progesterone values cannot differentiate between an ectopic and an intrauterine pregnancy.

FIGURE 19.3. Pseudogestational sac. Sagittal transabdominal view of the uterus demonstrates a pseudogestational sac, a collection of fluid within the uterus. (From Doubilet PM, Benson CB. Atlas of Ultrasound in Obstetrics and Gynecology. Philadelphia, PA: Lippincott Williams & Wilkins; 2003:320.)
Endometrial Curettage
Curettage of the uterine cavity can also help rule out ectopic pregnancy but should only be undertaken after the possibility of interrupting an intact pregnancy has been considered. Although intrauterine and ectopic pregnancies can exist simultaneously in rare cases (heterotopic pregnancy), identification of chorionic villi in tissue samples identifies an intrauterine location of the pregnancy and essentially rules out ectopic pregnancy. The presumptive diagnosis of ectopic pregnancy is reportedly inaccurate in nearly 40% of cases without histologic exclusion of a spontaneous pregnancy loss. The Arias-Stella reaction, a hypersecretory endometrium of pregnancy seen on histologic examination, occurs with both ectopic and intrauterine pregnancies and, therefore, is not useful in identifying an ectopic pregnancy.
Culdocentesis
Culdocentesis can identify hemoperitoneum (blood in the peritoneal cavity), which may indicate a ruptured ectopic pregnancy, although it is also consistent with other causes, such as a ruptured corpus luteum cyst. An 18G needle is inserted posterior to the cervix, between the uterosacral ligaments, and into the cul-de-sac of the peritoneal cavity (Fig. 19.4). Aspiration of clear peritoneal fluid (negative culdocentesis) indicates no hemorrhage into the abdominal cavity but does not rule out an unruptured ectopic pregnancy. Aspiration of blood that clots can indicate either penetration of a vessel or such rapid blood loss into the peritoneal cavity that the blood clot has not had time to undergo fibrinolysis. Aspiration of nonclotting blood is evidence of hemoperitoneum (positive culdocentesis), in which the blood clot has undergone fibrinolysis. If nothing is aspirated (equivocal or nondiagnostic culdocentesis), no information is obtained. Purulent fluid suggests a number of infection-related causes, such as salpingitis and appendicitis. Because none of the possible findings on culdocentesis can definitively confirm the presence or absence of ectopic pregnancy, its use in clinical practice is limited. When used, the principal useful result is that a positive culdocentesis identifies blood in the peritoneal cavity and confirms the need for further evaluation to identify the source of the bleeding. With the availability of other diagnostic technology, in many regions the use of culdocentesis has become almost obsolete.

FIGURE 19.4. Culdocentesis.
Laparoscopy
The most accurate technique of identifying an ectopic pregnancy is by direct visualization, which is done most commonly via laparoscopy. Even laparoscopy, however, has a 2% to 5% misdiagnosis rate. For example, an extremely early tubal gestation may not be identified because it may not distend the fallopian tube sufficiently to be recognized as an abnormality (false negative). Conversely, a false-positive diagnosis may result from a hematosalpinx (blood in the fallopian tube) being misinterpreted as an unruptured ectopic pregnancy or tubal abortion.
Management
Management may be either surgical or medical, depending on a variety of factors. In any individual case, surgery can be a simple procedure, but it can also be far more extensive, depending on the location of the ectopic pregnancy, whether or not it is ruptured, the gestational age of the pregnancy, and the patient’s desire for future fertility. Due to the inherent risks of each, medical therapy is preferred over surgery in appropriate patients.
Medical Management
Methotrexate is the medical treatment usually used as an alternative to surgical therapy. Methotrexate is a folic acid antagonist that competitively inhibits the binding of dihydrofolic acid to dihydrofolate reductase, which, in turn, reduces the amount of the active intracellular metabolite, folinic acid. It stops the growth of rapidly dividing placental, embryonic, and fetal cells.
An appropriate candidate for medical therapy is the woman who is asymptomatic, motivated, and has resources to be compliant with follow-up. Relative and absolute contraindications for medical management are listed in Box 19.1.
Factors that can be assessed in predicting the success of medical therapy include the initial β-hCG level, the size of ectopic pregnancy as determined by TVS, and presence or absence of fetal cardiac activity. The initial serum β-hCG level is the best prognostic indicator of treatment success in women managed with a single-dose methotrexate protocol. An initial serum value 15,000 IU/L has a success rate of 68%. Ectopic pregnancy size also appears to have an effect on methotrexate success rates. Success rates are reported as high as 93% in cases with ectopic masses 3.5 cm and the presence of cardiac activity are considered relative contraindications to medical management because these findings are associated with a lower success rate.
BOX 19.1 Contraindications to Medical Therapy for Ectopic Pregnancy
Absolute
• Breastfeeding
• Overt or laboratory evidence of immunodeficiency
• Alcoholism, alcoholic liver disease, or other chronic liver diseases
• Preexisting blood dyscrasias, such as bone marrow hypoplasia, leukopenia, or thrombocytopenia, or significant anemia
• Known sensitivity to methotrexate
• Active pulmonary disease
• Peptic ulcer disease
• Hepatic, renal, or hematologic dysfunction
Relative
• Gestational sac greater than 3.5 cm
• Embryonic cardiac motion
American College of Obstetricians and Gynecologists. Medical Management of Ectopic Pregnancy, Practice Bulletin No. 94. Washington, DC: American College of Obstetricians and Gynecologists; June 2008.
The most common side effects of methotrexate include nausea, vomiting, diarrhea, gastric distress, dizziness, and stomatitis. Intramuscular methotrexate given as part of a single-dose protocol has been the most widely used medical treatment of ectopic pregnancy. Close monitoring is imperative. A serum β-hCG level is determined before administering methotrexate and is repeated on days 4 and 7 following injection. Levels may continue to rise until day 4. Comparison is then made between the day 4 and the day 7 serum values. If there is a decline by 15% or more, serum β-hCG levels are measured weekly until they are undetectable. If the β-hCG level does not decline, the patient may require either surgery or a second dose of methotrexate if no contraindications exist. Surgical intervention may be required for patients who do not respond to medical therapy.
During the first few days following methotrexate administration, up to half of women experience abdominal pain that can be controlled with nonsteroidal anti-inflammatory drugs. This pain presumably results from tubal distention, tubal abortion, and/or hematoma formation.
Methotrexate given in a multidose protocol has also been used successfully, but the single-dose protocol described appears to reduce the amount of potential complications while achieving similar success rates. Other medical treatments that have been used include hyperosmolar glucose, potassium chloride, prostaglandins, and the progesterone receptor antagonist mifepristone (formerly referred to as RU-486). In some cases, an agent may be administered systemically, but sometimes it may be injected directly into the ectopic pregnancy.
Surgical Management
Women who are hemodynamically stable and in whom there is a small ectopic diameter, no fetal cardiac activity, and serum β-hCG concentrations with type 1 diabetes, the degree of metabolic control in early pregnancy has been found to be related to an increased risk of spontaneous abortion and major congenital malformation.
Environmental Factors
The abortion risk increases in a linear fashion with the number of cigarettes smoked per day. Both spontaneous abortion and fetal anomalies may result from frequent, high doses of alcohol during the first 8 weeks of pregnancy. Radiation administered at therapeutic doses to treat cancer may be an abortifacient. However, exposure to most diagnostic procedures that expose the patient to less than 5 rads does not increase the risk of miscarriage. The rates of spontaneous abortion and birth defects increase when the pregnancy is exposed to over 20 rads.
Immunologic Factors
There are a number of genetic disorders of blood coagulation that may increase the risk of both arterial and venous thrombosis. Some of the better studied thrombophilias are caused by mutations of the gene for factor V Leiden, prothrombin G20210A mutation, antithrombin III, proteins C and S, and methylene tetrahydrofolate reductase (hyperhomocysteinemia). These are most commonly associated with recurrent miscarriage.
Uterine Factors
Large and multiple uterine leiomyomas are common, and they may cause miscarriage. In most instances, their location is more important than their size, with submucous leiomyomata playing a more significant role than others, presumably because of their effect on implantation. In utero exposure to diethylstilbestrol has been associated with abnormally shaped uteri and cervical insufficiency, both of which can lead to spontaneous abortion, usually during the second trimester. Intrauterine synechiae (Asherman syndrome), a condition that is caused by uterine curettage with subsequent destruction and scarring of the endometrium, may also be a cause of spontaneous abortion. A uterine septum can similarly cause spontaneous abortion.
Classification and Differential Diagnosis of Spontaneous Abortions
Because the differential diagnosis of bleeding in the first trimester of pregnancy includes a wide range of possibilities, including ectopic pregnancy, hydatidiform mole, cervical polyps, cervicitis, and neoplasm, the patient should be examined whenever there is bleeding in early pregnancy.
Types of Spontaneous Abortion
Threatened abortion is characterized by bleeding in the first trimester without loss of fluid or tissue. About half of women with a threatened abortion proceed to spontaneous abortion. Those who carry a pregnancy complicated by threatened abortion to viability are at greater risk for preterm delivery and an infant of low birth weight. There does not, however, appear to be a higher incidence of congenital malformations in these newborns. Some patients describe bleeding at the time of their expected menses, sometimes referred to as implantation bleeding, which may be related to implantation of the pregnancy in the endometrium.
In cases of miscarriage, bleeding usually begins first, and cramping abdominal pain follows a few hours to several days later. The pain may present as anterior rhythmic cramps; as a persistent low backache, associated with a feeling of pelvic pressure; or as a dull, midline, suprapubic discomfort. The combination of persistent bleeding and pain usually indicates a poor prognosis for pregnancy continuation. Ectopic pregnancy should always be considered in the differential diagnosis of threatened abortion.
An inevitable abortion is vaginal bleeding and/or the gross rupture of the membranes in the presence of cervical dilation. Typically, uterine contractions begin promptly, resulting in expulsion of the products of conception. It is unusual for a pregnancy to successfully reach viability in this circumstance. Conservative management (i.e., nonintervention in an attempt to prolong the pregnancy in these patients) significantly increases the risk of maternal infection.
In an incomplete abortion, the internal cervical os opens and allows passage of blood and some tissue. In some cases, retained placental tissue remains in the cervical canal, allowing easy extraction from an exposed external os with ring forceps. If needed, a suction curettage is used to remove remaining products of conception from the uterine cavity.
Complete abortion refers to a documented pregnancy that spontaneously passes all of the products of conception. Before 10 weeks of gestation, the fetus and placenta are commonly expelled together.
A missed abortion is the retention of a failed intrauterine pregnancy for an extended period, usually defined as more than two menstrual cycles. These patients have an absence of uterine growth and may have lost some of the early symptoms of pregnancy. Many women have no symptoms during this period except persistent amenorrhea. If the missed abortion terminates spontaneously, and most do, the process of expulsion is the same as in any abortion.
Recurrent Pregnancy Loss
Recurrent pregnancy loss is a term that has historically been applied when a patient has had more than two consecutive pregnancy losses. There is also support for applying the term to cases in which the patient has lost only two pregnancies. The timing of the pregnancy losses may provide a clue to their cause. Genetic and autoimmune factors most frequently result in early embryonic losses, whereas anatomic abnormalities are more likely to result in second-trimester losses.
First-Trimester Pregnancy Loss
Karyotyping is recommended for both parents when recurrent early abortion occurs, because there is a 3% chance that one parent is an asymptomatic carrier of a genetically balanced chromosomal translocation. The immune system also has a role in up to 20% of early recurrent pregnancy loss. Antiphospholipid antibodies are a family of autoantibodies that bind to negatively charged phospholipids. Lupus anticoagulant and anticardiolipin antibody have been linked with excessive pregnancy wastage. Treatment may include low-dose aspirin along with unfractionated heparin. This therapy, begun when pregnancy is diagnosed, may be continued until delivery. Other immunologic defects associated with recurrent miscarriage are factor V Leiden defect and prothrombin gene mutation.
Intrauterine synechiae associated with Asherman syndrome may occur after a curettage procedure has denuded the endometrium past the layer of the basalis, which promotes the formation of webs of scar tissue to develop within the uterine cavity. Asherman syndrome and other anatomic abnormalities account for approximately 10% of early recurrent pregnancy losses. Asherman syndrome can be associated with not only early recurrent pregnancy loss but also amenorrhea, hypomenorrhea, cyclic pain, and infertility. The diagnosis is confirmed by a hysterogram that shows the characteristic webbed pattern or by hysteroscopy. Treatment involves lysis of the synechiae and postoperative treatment with high doses of estrogen to facilitate endometrial proliferation, leading to the reestablishment of a normal endometrial layer.
Second-Trimester Pregnancy Loss
Recurrent pregnancy losses that occur later than the first trimester are typically caused by anatomic abnormalities, such as septate uteri or fibroids. In these cases, management including hysterography, operative hysteroscopy, and/or laparoscopy may be required to correct the problem. If leiomyomata are felt to be the causative factor of recurrent second-trimester pregnancy loss, myomectomy is appropriate. Similarly, reconstructive surgery of the uterus may be necessary for congenital uterine malformations.
Recurrent pregnancy loss in the second trimester can also be caused by cervical insufficiency, a condition in which the increasing pressure within the uterus causes a weakened cervix to efface and dilate painlessly. Predisposing factors include uterine anomalies as well as previous trauma to the cervix including mechanical dilation or history of conization. Cervical cerclage is used to tie the cervix closed during the early second trimester if cervical insufficiency is deemed the etiology of recurrent second-trimester loss.
Treatment
No intervention is necessary for patients with threatened abortion even if the bleeding is accompanied by low abdominal pain and cramping. If there is no evidence of significant abnormality on ultrasound evaluation, and if the pregnancy is found to be intact, the patient can be reassured and allowed to continue normal activities. In cases of complete abortion, the uterus is small and firm, the cervix is closed, and ultrasound identifies an empty uterus. No further intervention is needed.
For incomplete, inevitable, or missed abortions, treatment may be expectant, medical, or surgical. Surgical treatment is definitive and predictable but is invasive and not necessary for all women. Expectant or medical management using prostaglandins may obviate curettage, but both approaches are associated with unpredictable bleeding, with some women still requiring surgery to empty the uterus. In cases of significant pain, hemorrhage, or infection, prompt completion of abortion is warranted.
In such cases, immediate considerations include control of bleeding, prevention of infection, pain relief, and emotional support. Bleeding is controlled by ensuring that the products of conception have been expelled from the uterus. The use of ultrasound to evaluate the uterus helps to determine whether surgical intervention is needed. If tissue remains in the uterus, curettage is typically used to remove the remaining products of conception. Hemostasis is enhanced through uterine contraction stimulated by oral methylergonovine. Removal of the products of conception and vaginal rest (no tampons, douches, or intercourse) decreases the risk of infection. A mild analgesic may be required and should be offered. Rh-negative mothers should receive Rh immunoglobulin (RhoGAM). Chromosomal evaluation of spontaneous abortions is not recommended, unless there is a history of recurrent abortion.
Emotional support is important for both the short- and long-term well-being of both the patient and her partner. No matter how well-prepared a couple is for the possibility of pregnancy loss, the event is a significant disappointment and cause of stress. When appropriate, the couple should be reassured that the loss was not precipitated by anything that they did or did not do and that there was nothing that they could have done to prevent the loss.
Follow-Up
A follow-up office visit is generally scheduled for 2 to 6 weeks after the loss of a pregnancy. This is an appropriate time to evaluate uterine involution, assess the return of menses, and discuss reproductive plans. The causes (or lack of causes) of the pregnancy loss should also be reiterated. The impact of this loss on future childbearing should be discussed. A single pregnancy loss does not significantly increase the risk of future losses. Multiple pregnancy losses carry an increased risk of future pregnancies and warrant further evaluation for treatable etiologies.
 INDUCED ABORTION
INDUCED ABORTION
Termination of an intact pregnancy before the time of viability can be done to safeguard the health of the mother; because of severe fetal abnormality; or on an elective, that is, voluntary basis. Elective abortion has been legal in the United States since the 1973 Supreme Court decision of Roe v. Wade. Since that time, various local and state laws have been proposed to significantly limit access to elective abortion. The health care provider should maintain a nonjudgmental position in treating women who may be considering elective termination of pregnancy.
Induced abortion is the medical or surgical termination of pregnancy typically before the time of fetal viability. In 2007, approximately 827,000 legal induced abortions were reported to the Centers for Disease Control. The abortion rate was 16.0 abortions per 1,000 women ages 15 to 44 years, and the abortion ratio was 231 abortions per 1,000 live births. The number of abortions and the rate and ratio all represent a 2% to 3% decrease from the year before, reflecting a downward trend in elective abortions over the past decade. Medical and/or surgical complications are associated with all choices, with the fewest complications related to elective abortion in the first trimester.
The most common form of suction curettage for first-trimester abortions, vacuum aspiration, requires a rigid cannula attached to an electric-powered vacuum source. Alternatively, manual vacuum aspiration uses a similar cannula that attaches to a handheld syringe for its vacuum source. Second-trimester abortions are most commonly performed through the cervix, using suction or extraction forceps, or by the use of prostaglandins, as in the form of intra-amniotic injections or vaginal suppositories.
Outpatient medical abortion is an acceptable alternative to surgical abortion in appropriately selected women with pregnancies less than 49 days of gestation (calculated from the first day of the LMP). Beyond this point, surgical abortion is the preferred method of early abortion. Three medications for early medical abortion have been widely studied and used: the antiprogestin mifepristone (RU-486), the antimetabolite methotrexate, and the prostaglandin misoprostol. These agents cause abortion by increasing uterine contractility either by reversing the progesterone-induced inhibition of contractions—mifepristone and methotrexate, or by stimulating the myometrium directly—misoprostol. Abortion with this medical method is not always complete. As a result, the patient should be made aware that suction curettage may be required.
Complications
The most common complications associated with an induced abortion include uterine perforation, cervical laceration, hemorrhage, incomplete removal of the products of conception, and infection. In cases of postabortal infection, the patient usually presents with fever, pain, a tender uterus, and mild bleeding. Oral antibiotics and antipyretics are typically sufficient to manage these mild infections. If tissue remains in the uterus (incomplete abortion), a repeat suction curettage is necessary. The second most common complication following induced abortion is bleeding. Risk of death from abortion during the first 2 months of pregnancy is less than 1 per 100,000 procedures, with increasing rates as pregnancy progresses (vs. 7.7 maternal deaths per 100,000 live births).
Septic Abortion
An infected abortion, either complete or incomplete, is known as a septic abortion. Patients may present with sepsis, shock, hemorrhage, and, possibly, renal failure. It rarely occurs as a complication of a legal abortion but is more commonly associated with criminal abortions, that is, those done illegally, under unsterile conditions, by persons who may have little or no knowledge of medicine or anatomy. Broadspectrum parenteral antibiotics, intravenous fluid therapy, and prompt evacuation of the uterus are indicated. A careful evaluation for trauma, including perforation of the uterus, vagina, or intra-abdominal structures, should also be carried out.
Postabortal Syndrome
Postabortal syndrome develops when the uterus fails to remain contracted after spontaneous abortion (with or without suction curettage) or elective/therapeutic abortion. The patient presents with cramping pain and/or bleeding and is found to have an open cervix, bleeding, and a large, “softer-than-expected” uterus, a result of the collection of blood in the uterus (hematometra). The clinical presentation is often indistinguishable from incomplete abortion. Suction curettage is the treatment for both conditions. Postevacuation treatment with an ergot derivative and an antibiotic reduces the risk of postabortal syndrome, further bleeding, and infection.
Clinical Follow-Up
Bleeding can occur with both an ongoing pregnancy (threatened abortion) and a nonviable pregnancy (incomplete, complete, or missed abortion). Determining whether the pregnancy is intrauterine or extrauterine is of immediate concern because of the potential need for emergent treatment of an ectopic pregnancy. Ultrasound is useful to identify both the location of an early pregnancy and whether or not it is intact. The ovarian cyst is most likely a corpus luteum of pregnancy. No treatment for this patient is indicated at this time because both the intrauterine pregnancy and the corpus luteum cyst are normal at this time.
thePoint Visit http://thepoint.lww.com/activate for an interactive USMLE-style question bank and more!