Chapter 20 Endocrine Disorders
This chapter deals primarily with APGO Educational Topic Area:
TOPIC 17 MEDICAL AND SURGICAL COMPLICATIONS OF PREGNANCY
Students should be able to identify how pregnancy affects the natural history of various endocrine disorders and how a preexisting endocrine disorder affects maternal and fetal health.
They should be able to outline a basic approach to evaluation and management of endocrine disorders in pregnancy.Clinical Case
A 22-year-old primigravida is in your office for her initial obstetric visit. Her menstrual history suggests that she is about 12 weeks’ pregnant. In reviewing her history, you find that she was diagnosed with diabetes 6 years ago and has been taking insulin twice daily since then. She checks her blood glucose values “every now and then” and reports them to be in the 150 to 180 range. She has not had regular diabetic care. In looking over her laboratory reports from studies done 2 days ago, you note that her HgbA1c is elevated at 9.5. How do you counsel her about this HgbA1c result as well as overall obstetric care in a patient with diabetes?
Maternal medical or surgical conditions can complicate the course of a pregnancy and can be affected by pregnancy. Physicians providing obstetric care must have a thorough understanding of the effect of pregnancy on the natural course of a disorder, the effect of the disorder on a pregnancy, and the change in management of the pregnancy and disorder caused by their coincidence.
 DIABETES MELLITUS
DIABETES MELLITUS
Approximately 7% of pregnancies are complicated by diabetes that either develops during pregnancy (gestational diabetes) or was antecedent to pregnancy (pregestational diabetes mellitus). In either case, diabetes has significant implications for the mother and fetus during pregnancy, and conversely, pregnancy significantly affects diabetes.
Whether diabetes is newly diagnosed or long standing, intense management may be stressful, and all those involved with obstetric care should be mindful of the extra emotional attention many of these patients need.Classification of Diabetes in Pregnancy
The American Diabetes Association (ADA) identifies three forms of glucose intolerance:
• Type 1 diabetes mellitus refers to diabetes diagnosed in childhood. It is thought to be caused by immunologic destruction of cells of the pancreas, resulting in necessary insulin replacement. Diabetic ketoacidosis (DKA) is more common in patients with this type of diabetes.
• Type 2 diabetes mellitus is adult-onset glucose intolerance. Patients with type 2 diabetes mellitus are frequently overweight, and the disease can often be controlled with weight control and a carefully followed diet. This type of diabetes is thought to result from insulin resistance and exhaustion of the cells, rather than their destruction.
• Gestational diabetes mellitus (GDM) refers to glucose intolerance identified during pregnancy. In most patients, it subsides postpartum, although glucose intolerance in subsequent years occurs more frequently in this group of patients.
Physiology of Glucose Metabolism in Pregnancy
Dietary habits frequently change during pregnancy. Food intake may decrease early in pregnancy because of nausea and vomiting, and food preferences may change later in pregnancy. Several pregnancy-associated hormones also have a major effect on glucose metabolism. Most notable of these is human placental lactogen (hPL), which is produced in abundance by the enlarging placenta. hPL affects both fatty acid and glucose metabolism. It promotes lipolysis with increased levels of circulating free fatty acids and causes a decrease in glucose uptake. In this manner, hPL can be thought of as an anti-insulin. The increasing production of this hormone as pregnancy advances generally requires ongoing changes in insulin therapy to adjust for this effect.
Other hormones that have demonstrated lesser effects include estrogen and progesterone, which interfere with the insulin–glucose relationship, and insulinase, which is produced by the placenta and degrades insulin to a limited extent. These effects of pregnancy on glucose metabolism make the management of pregnancy-associated diabetes difficult. DKA, for example, is more common in pregnant patients.
With increased renal blood flow, the simple diffusion of glucose in the glomerulus increases beyond the ability of tubular reabsorption, resulting in the normal glucosuria of pregnancy, commonly of approximately 300 mg/day. In patients with diabetes, this glucosuria may be much greater, but, because of the poor correlation of pregnancy glucosuria values and simultaneous blood glucose concentrations, using urinary glucose levels is of little value in glucose management during pregnancy.
Fetal Morbidity and Mortality
Congenital Anomalies
Infants of mothers with diabetes are at a sixfold increased risk for congenital anomalies over the 1% to 2% baseline risk of all patients. The most commonly encountered anomalies are cardiac, central nervous system (CNS), renal, and limb deformities. Sacral agenesis is a unique but rare anomaly for this group (Fig. 20.1). The risk of congenital anomalies increases with increasing glycosylated hemoglobin levels (HgbA1c) when entering pregnancy. Levels of 5% to 6% are associated with a fetal malformation rate of 2% to 3%, which is close to the rate in normal pregnancies, whereas HgbA1c levels >9.5% are associated with a malformation rate of 22% or higher.
Spontaneous Abortion and Stillbirth
The risk of spontaneous abortion is similar in patients with well-controlled diabetes and in patients without diabetes. However, the risk of spontaneous abortion is significantly increased for patients with diabetes if glucose control is poor when entering pregnancy. There is also an increased risk of intrauterine fetal demise and stillbirth, especially when diabetic control is inadequate.
Because of this potentially devastating outcome, beginning at approximately 32 to 34 weeks of gestation, various antepartum fetal tests may be initiated to monitor fetal health (see Sections “Antepartum Fetal Monitoring”).
FIGURE 20.1. Infant born to a diabetic mother with poor glycemic control. Hypoplastic lower extremities and lack of lumbosacral spine are evident. (From Gabbe SG, Graves CR. Management of diabetes mellitus complicating pregnancy. Obstet Gynecol. 2003;102(4):857–868.)
Macrosomia
Excessive fetal growth, or macrosomia (usually defined as a fetal weight in excess of either 4,000 or 4,500 g), is more common in pregnant patients with diabetes because of the fetal metabolic effects of increased glucose transfer across the placenta. However, intrauterine growth restriction can also occur due to uteroplacental insufficiency. For these reasons, serial ultrasonography is often performed to follow fetal growth. When the estimated fetal weight by ultrasound late in pregnancy is greater than 4,500 g, cesarean delivery is often recommended to avoid the risk of fetopelvic disproportion, shoulder dystocia, and other birth trauma associated with large infants, insofar as these risks are increased even further in the setting of diabetes.
Polyhydramnios
Another complication of pregnancy in patients with diabetes is an increase in amniotic fluid volume greater than 2,000 mL, a condition known as hydramnios or polyhydramnios. Encountered in approximately 10% of mothers with diabetes, the increases in amniotic fluid volume and uterine size are associated with an increased risk of placental abruption and preterm labor as well as postpartum uterine atony. This condition is monitored while serial ultrasonography is performed for fetal growth, at which time the amount of amniotic fluid can be evaluated.
Other Complications
Neonatal hypoglycemia is often encountered in infants of women with diabetes.
It results from the sudden change in the maternal–fetal glucose balance, in which an increased maternal glucose crossing the placenta is countered by an increase in fetal production of insulin. However, when the maternal supply of glucose is removed, this higher level of insulin can cause significant neonatal hypoglycemia. In addition, these newborns are subject to an increased incidence of neonatal hyperbilirubinemia, hypocalcemia, and polycythemia.Infants of mothers with diabetes also tend to have an increased frequency of respiratory distress syndrome. The usual tests of lung maturity may be less predictive for these infants.
Pregestational Diabetes
Approximately 2% of all pregnant patients are diabetic before pregnancy. Type 2 pregestational diabetes mellitus is most common. Although 90% of diabetes cases encountered during pregnancy are GDM, more than one half of these eventually develop type 2 pregestational diabetes mellitus later in life.
Antepartum Fetal Monitoring
Women with pregestational diabetes should receive an ultrasound examination early in pregnancy to check for fetal viability and accurately date the gestational age. At 18 to 20 weeks of gestation, an ultrasound examination that focuses on identification of congenital anomalies, especially those of the CNS, genitourinary system, heart and great vessels, is indicated. Echocardiography may also be done if there are suspected cardiac defects or when the fetal heart and great vessels could not be visualized by ultrasonography.
Antepartum fetal monitoring, including fetal movement counting, the nonstress test, biophysical profile, and contraction stress test, performed at appropriate intervals, is a valuable approach and can be used to monitor women with pregestational diabetes. This testing is usually initiated at 32 to 34 weeks of gestation but can be undertaken earlier if other high-risk conditions such as fetal growth restriction exist.
Maternal Complications
Pregnant patients with pregestational diabetes, especially type 1 diabetes, are at higher risk for DKA, the management of which is not altered in pregnancy.
Fetal death can accompany DKA, so electronic fetal monitoring is essential until the maternal metabolic status is stabilized.Hypoglycemia may also occur periodically, especially early in pregnancy, when nausea and vomiting interfere with caloric intake. Although hypoglycemia does not have adverse effects on the fetus, patients and their families should be taught how to respond quickly and appropriately to hypoglycemia.
In addition to the added difficulties of glucose management and the increased risk of DKA during pregnancy, mothers with pregestational diabetes have a twofold increase in the incidence of pregnancy-induced hypertension, or preeclampsia, compared with patients without diabetes. Because of this increased risk of preeclampsia, 24-hour urine collections to determine the level of proteinuria and creatinine clearance are often used in pregestational diabetics. Additionally, if patients have preexisting diabetic nephropathy, manifested by prepregnancy creatinine >1.5 mg% or severe proteinuria, they are at an increased risk for progression to end-stage renal disease, and serial monitoring of renal function is warranted.
Diabetic retinopathy worsens in approximately 15% of pregnant patients with preexisting diabetes, some proceeding to proliferative retinopathy and loss of vision if the process remains untreated by laser coagulation. Therefore, women with pregestational type 1 or type 2 diabetes should have an ophthalmologic evaluation once in their first trimester if asymptomatic and as needed if symptoms arise.
Management
The patient with long-standing diabetes should realize that strict control of her glucose levels is advised during pregnancy, with greater attention to and more frequent monitoring of glucose values. For these patients, management ideally begins before conception, with the goal of optimal glucose control before and during pregnancy. Women with pregestational diabetes mellitus should be offered preconception counseling and care to reduce the risks of spontaneous abortion and congenital anomalies (see Section “Fetal Morbidity and Mortality” and Chapter 6). HgbA1c levels can be measured to reflect average glucose values over the preceding 12 weeks. These levels can then be used to monitor glucose control both before and during pregnancy and to predict the likelihood of congenital anomalies in the fetus (see Section “Fetal Morbidity and Mortality”).
Excellent glucose control is achieved using a careful combination of diet, exercise, and insulin therapy. Insulin requirements will increase throughout pregnancy, most markedly in the period between 28 and 32 weeks of gestation.
The impact of pregnancy on diabetes, and vice versa, must also be emphasized to the pregnant patient with pregestational diabetes. Patients may need to be seen every 1 to 2 weeks during the first two trimesters and weekly after 28 to 30 weeks of gestation.
Gestational Diabetes
The prevalence of GDM is estimated to be about 7%, and this rate is increasing with higher rates of obesity. GDM is usually identified by prenatal screening of pregnant patients. It may be suspected, however, in patients with known risk factors for GDM, which include age, ethnicity, past obstetric history (gestational diabetes in a previous pregnancy, a history of an infant weighing more than 4,000 g at birth, repeated spontaneous abortions, or a history of unexplained stillbirth), a strong family history of diabetes, and obesity. However, 50% of patients identified as having gestational diabetes do not have such risk factors.
Laboratory Screening
The most commonly used screening test for glucose intolerance during pregnancy is given at 24 to 28 weeks of gestation and consists of a 50-g, 1-hour oral glucose challenge. Fasting is not necessary for this test. Patients whose glucose value exceeds 140 mg/dL (some use 130 or 135 mg/dL) require a standard 3-hour glucose tolerance test using 100 g of glucose. Two or more abnormal results of the 3-hour test establish the diagnosis of gestational diabetes.
In patients lacking any risk factors, the 1-hour glucose screening is usually performed between 24 and 28 weeks of gestation because glucose intolerance is generally evident by that time. Using this screening method, approximately 15% of patients have an abnormal screening test. Of those patients who then proceed to have the standard 3-hour oral glucose tolerance test, approximately 15% are diagnosed as having GDM. Treatment of women with GDM is associated with reduced rates of maternal and fetal complications including excessive weight gain, macrosomia, preeclampsia, shoulder dystocia, and cesarean delivery. Although many practitioners choose to screen high-risk patients early in pregnancy, the benefit of early treatment of women with GDM identified early in pregnancy has not been demonstrated but, rather, has been accepted on a theoretical basis.
Antepartum Fetal Monitoring
There is currently insufficient evidence to determine the optimal antepartum testing regimen for women with relatively normal glucose levels on diet therapy and no other risk factors. Despite the lack of evidence, it is reasonable to conclude that women whose GDM is not well controlled, who require insulin, or who have other risk factors such as hypertension should receive the same antepartum testing regimen as women with pregestational diabetes. Although ultrasonography can be used to assess congenital anomalies, the reliability of ultrasonography to estimate fetal weight and predict macrosomia prior to delivery has not been established.
Management
Often overlooked or underemphasized in the overall management of a patient whose pregnancy is complicated by diabetes mellitus is the importance of patient education. The patient with newly diagnosed diabetes should receive general diabetic counseling, along with information about the unique features of the combination of diabetes and pregnancy. Home glucose monitoring is the norm, and instruction in technique should be provided.
Diet and Glucose Monitoring
The overall goal of managing GDM is to control glucose values within circumscribed limits: fasting glucose levels of less than 95 mg/dL, 1-hour postprandial levels of 130 to 140 mg/ dL, or 2-hour postprandial values less than 120 mg/dL. The mainstay of GDM management is diet. The recommended diet is about 30 kcal/kg/day of ideal body weight, composed of approximately 45% complex carbohydrates, 35% fat, and 20% protein. With careful attention to diet, many mothers with GDM do not require insulin. Current available evidence does not support a recommendation for or against moderate caloric restriction in obese women with GDM. However, if caloric restriction is used, the diet should be restricted by no more than 33% of calories.
Patients are instructed to obtain a morning fasting glucose, along with pre- and/or postprandial glucose values throughout the day and evening. The precise goals for glucose control vary, but, in general, the fasting plasma glucose should be maintained in the 90 to 100 mg/100 mL range and the postprandial values obtained throughout the day at 110–120 mg/100 mL or 2-hour postprandial glucose levels >140 mg/100 mL) may not be adequately controlled on oral hypoglycemic agents and may need to be started directly on insulin.
Patients with diabetes are monitored closely throughout pregnancy, usually at 1- to 2-week intervals. Insulin adjustments are made on the basis of the glucose logs maintained by the patient. Also, as previously described, insulin requirements of a pregnant patient are expected to increase as pregnancy advances because of the rising production of hPL by the placenta, with its insulin-resistant effect.
Infection
Infections occur more frequently in mothers with diabetes. The glucose-rich urine is an excellent environment for bacterial growth; the risk of urinary tract infection and pyelonephritis is approximately double that of nondiabetic pregnant patients. Patients should be told to promptly report any symptoms that suggest infection so that identification and treatment can be initiated.
Labor and Delivery of the Patient with Diabetes
The goal is for the patient with diabetes to deliver a healthy child vaginally. The adequacy of glucose control, the well-being of the infant, estimated fetal weight by ultrasound, presence of hypertension or other complications of pregnancy, gestational age, presentation of the fetus, and status of the cervix are all factors involved in decisions regarding delivery. In the well-controlled patient with diabetes who has no complications, induction at term (39 weeks) is often under-taken. For women with GDM or pregestational diabetes and an estimated fetal weight of 4,500 g or more, cesarean delivery may be considered. If an earlier delivery is deemed necessary for either fetal or maternal indications, fetal maturity studies may be performed on amniotic fluid obtained by amniocentesis. If antepartum steroids for fetal lung maturity become necessary (e.g., for patients with preterm labor), frequent glucose monitoring and, at times, increased doses of insulin are necessary to counter the hyperglycemic effects of corticosteroids.
Whether the patient’s labor begins spontaneously or is induced, the goal of intrapartum insulin therapy is strict glucose control. Once active labor begins or glucose levels decrease to 70 mg/dL, a constant glucose infusion of a 5% dextrose solution delivered at a rate of 100 to 150 mL/hour is administered to maintain a glucose level of 100 mg/dL. The plasma glucose level should be assessed every 1 to 2 hours. Short-acting insulin may be administered, usually by constant intravenous infusion, if glucose levels exceed 100 mg/dL. Maternal ketonuria is also monitored and can be managed during labor using the glucose-insulin infusion.
With delivery of the placenta, the source of the “anti-insulin” factors, most notably hPL, is removed. With its short half-life, the effect on plasma glucose is evident within hours. Many patients do not require any insulin for a few days postpartum. Routine management generally consists of frequent glucose assessments and a sliding-scale approach with minimal insulin injections. The goals for optimal glucose values are less stringent in the puerperium than during pregnancy. For patients with GDM, no further insulin is required postpartum. In patients with pregestational diabetes, insulin is generally resumed at 50% of the prepregnant dose once a patient is consuming a normal diet. Thereafter, insulin can be adjusted over the ensuing weeks, with requirements usually reaching the prepregnancy level.
More than 95% of mothers with gestational diabetes return to a completely normal glucose status immediately postpartum; however, approximately 50% of these women go on to develop type 2 diabetes later in life and need to be educated about the importance of maintaining a healthy diet and regular exercise program. Glucose tolerance screening is advocated 2 to 4 months postpartum to detect the 3% to 5% who remain diabetic and require treatment. Typically, such screening involves a 75-g glucose load, followed by plasma glucose determination 2 hours later. A value above 140 mg/dL requires follow-up. The ADA recommends repeat testing at least every 3 years for women who had a pregnancy affected by GDM and normal results of postpartum screening.
For contraception, barrier methods or intrauterine contraceptives are often chosen; patients who choose oral contraceptives should monitor their glucose values to identify an increase that is sometimes seen with this method (see Chapter 26).
THYROID DISEASE
As with diabetes mellitus, thyroid disease may predate pregnancy or may initially manifest during pregnancy. Obstetric conditions, such as gestational trophoblastic disease or hyperemesis gravidarum, may themselves affect thyroid function. All neonates of women with thyroid disease are at risk for neonatal thyroid dysfunction. For this reason, the neonate’s pediatrician should be informed about the maternal diagnosis.
Pathophysiology
Thyrotoxicosis is the condition that results from excess production of and exposure to thyroid hormone from any cause. Hyperthyroidism is thyrotoxicosis caused by hyperfunctioning of the thyroid gland. Graves’ disease is an autoimmune disease characterized by abnormal production of thyroidspecific immunoglobulins that either stimulate or inhibit thyroid function. Exacerbation of the signs and symptoms of hyperthyroidism is called a thyroid storm. Hypothyroidism is caused by inadequate thyroid hormone production. Postpartum thyroiditis is an autoimmune inflammation of the thyroid gland that presents as new-onset, painless hypothyroidism, transient thyrotoxicosis, or thyrotoxicosis followed by hypothyroidism within 1 year postpartum.
Levels of thyroid-binding globulin (TBG) normally increase in pregnancy. Test results that change significantly in pregnancy are those influenced by TBG concentration, including total thyroxine (TT4), total triiodothyronine (TTd), and resin triiodothyronine uptake (TR3U). A transient increase may also occur in free thyroxine (FT4) and free thyroxine index (FTI) levels in the first trimester (Fig. 20.2).
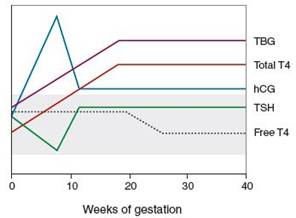
FIGURE 20.2. The pattern of changes in thyroid function and human chorionic gonadotropin (hCG) concentration according to gestational age. The shaded area represents the normal range of thyroid-binding globulin (TBG), total thyroxine (T4), thyroid-stimulating hormone (TSH), and free T4 in the nonpregnant woman. (Modified from Brent GA. Maternal thyroid function: interpretation of thyroid function tests in pregnancy. Clin Obstet Gynecol. 1997;40(1):3–15.)
Plasma iodide levels decrease during pregnancy, and this change may cause a noticeable increase in thyroid gland size (approximately 18% change) in 15% of women. However, in most women, the thyroid returns to normal size postpartum.
Laboratory Screening
There is insufficient evidence to warrant routine screening of asymptomatic pregnant women for hypothyroidism. Testing should be performed in women with a prior history of thyroid disease or symptoms of thyroid disease. Thyroid function is evaluated by measuring thyroid-stimulating hormone (TSH) levels. TSH does not cross the placenta, so this test is an accurate measure of hormone function during pregnancy. In pregnant women suspected of being hyperthyroid or hypothyroid, FT4 and FTI levels should be measured in addition to TSH.
Management of Existing Thyroid Disease in Pregnancy
Hyperthyroidism
Hyperthyroidism in pregnancy is treated with thionamides, specifically propylthiouracil (PTU) and methimazole. Both drugs cross the placenta but methimazole more so than PTU, theoretically causing greater fetal thyroid suppression. Methimazole has been associated with reports of fetal scalp defects (aplasia cutis) and choanal atresia and should be avoided in the first trimester. With more recent reports of hepatotoxicity with PTU, although rare, methimazole is being used more often in pregnancy beyond the first trimester. Both drugs are considered compatible with breastfeeding. The goal of treatment during pregnancy is to maintain the FT4 or FTI in the high normal range using the lowest possible dosage of thionamides to minimize fetal exposure. Thionamide treatment for Graves’ disease in pregnancy may suppress fetal and neonatal thyroid function and has also been associated with fetal goiter. Neonatal hypothyroidism is usually transient and does not require treatment.
BOX 20.1 Symptoms of Thyroid Storm
Fever
Tachycardia out of proportion to the fever
Altered mental status (including restlessness, nervousness, confusion, and seizures)
Vomiting
Diarrhea
Cardiac arrhythmia
Thyroid Storm
Thyroid storm is a medical emergency characterized by an extreme hypermetabolic state. Although rare (it occurs in 1% of pregnant patients with hyperthyroidism), it carries a high risk of maternal heart failure. It is often precipitated by infection, surgery, labor, or delivery and is more common in women with poorly controlled hyperthyroidism. Thyroid storm must be diagnosed and treated quickly in order to prevent shock, stupor, and coma (Box 20.1). Treatment of thyroid storm consists of a standard series of drugs, each of which plays a role in suppressing thyroid function. The underlying precipitating event should also be treated. The fetus should be appropriately evaluated with ultrasonography, biophysical profile, or nonstress test, depending on the gestational age.
Hypothyroidism
Treatment of hypothyroidism in pregnant women is the same as for nonpregnant women and involves administration of levothyroxine at sufficient dosages to normalize TSH levels. Maternal thyroxine requirements increase in women with hypothyroidism diagnosed before pregnancy. Levothyroxine levels should be adjusted at 4-week intervals until TSH levels are stable. Thereafter, levels should be checked once per trimester.
Management of Thyroid Disease Diagnosed During and After Pregnancy
Biochemical Hyperthyroidism
Severe nausea and vomiting of pregnancy (hyperemesis gravidarum) may cause biochemical hyperthyroidism, in which levels of TSH are undetectable, FTI levels are elevated, or both. This condition resolves spontaneously by 18 weeks of gestation. Routine measurements of thyroid function are not recommended in patients with hyperemesis gravidarum unless other overt signs of hyperthyroidism are evident.
Postpartum Thyroiditis
Postpartum thyroiditis occurs in 5% of women who have no prior history of thyroid disease. Postpartum thyroiditis also may occur after pregnancy loss and has a 70% risk of recurrence. Almost half of women with postpartum thyroiditis have hypothyroidism, whereas the remaining women are evenly split between thyrotoxicosis and thyrotoxicosis followed by hypothyroidism. Postpartum thyrotoxicosis usually resolves on its own without treatment. Of those with hypothyroidism, approximately 40% of women require treatment for extremely high TSH levels or an increasing goiter size. Only 11% of women diagnosed with postpartum hypothyroidism develop permanent hypothyroidism.
Clinical Follow-Up
With major changes on the way, your patient manages her diabetes with frequent visits and close monitoring of her glucose values and her fetus. She delivers a healthy child vaginally at 39 weeks. If she plans to have another pregnancy in the future, she knows that preconception care and strict control of her diabetes promote another healthy infant outcome.
thePoint Visit http://thepoint.lww.com/activate for an interactive USMLE-style question bank and more!