Complications of Medical and Surgical Abortion
Rosanne L. Botha, Paula H. Bednarek, Andrew M. Kaunitz, and Alison B. Edelman
EPIDEMIOLOGY AND HISTORY OF ABORTION IN THE UNITED STATES
Abortion is one of the most common medical procedures for women aged 15 to 44 years in the United States (1,2).
Each year, almost half of all pregnancies among American women are unintended, and about half of these unplanned pregnancies end in abortion. If current rates continue, it is estimated that 35% of all reproductive-age women in America will have had an abortion by the time they reach the age of 45 (3). In 2005, approximately 1.2 million abortions were performed in the United States, with nearly 90% performed in the first trimester (before 12 weeks) (3). Both medical and surgical abortions are low-risk procedures when performed early in gestation, and in a safe, legal setting. Fewer than 0.3% of abortion patients experience a complication that requires hospitalization (4). The risk of death from abortion is 1 in 100,000 or less while the risk of a woman dying from giving birth is 10 times higher (5-7).Abortion has not always been so safe. Before its legalization in the United States in 1973, many women died or had serious complications following procedures by untrained practitioners with suboptimal techniques in unsanitary conditions or after attempts to self-induce abortion using knitting needles or wire coat hangers. These practices resulted in sepsis, thrombosis of the pelvic vasculature, disseminated intravascular coagulation (DIC), and death. In countries where abortion is still illegal, unsafe abortion remains a leading cause of maternal death (8).
SURGICAL ABORTION
Over 90% of surgical abortions are performed in outpatient settings, using either electric or manual (handheld syringe) vacuum aspiration (9). Perioperative antibiotics are routinely provided to patients. Women typically experience cramping and bleeding similar to a period for a few days to several weeks following the procedure.
Regular menses usually returns in 4 to 6 weeks postprocedure.MEDICAL ABORTION
In the United States, medical abortion is offered at gestational ages 9 weeks or less using 200 mg of oral mifepristone followed by 800 μg of misoprostol vaginally or buccally 6 to 48 hours later (10). Misoprostol-alone regimens have lower rates of successful complete abortion but are still utilized by some women to self-induce abortion or in countries where mifepristone is not available (10). Patients are asked to return for an ultrasound approximately 2 weeks after their medical abortion to confirm that the procedure is complete. During the actual abortion, bleeding can be heavy and cramping may require narcotic analgesia. Both symptoms are expected to last for several hours while passing the pregnancy but usually improve within 24 hours (11). Nausea, vomiting, and diarrhea are known side effects of misoprostol and are also frequently reported (12). Symptoms of recovery following a medical abortion are similar to those with surgical abortion.
MANAGING SPECIFIC COMPLICATIONS OF ABORTION
Although first trimester medical and surgical abortions are safe with low rates of major complications, these are common procedures, and therefore it is not unusual for women with abortion complications to present for emergent care. Physicians in such settings may encounter complications such as bleeding, infection, retained products of conception, continuing pregnancy, or ectopic pregnancy. Gynecologic consultation or referral is appropriate for these patients.
Hemorrhage
Hemorrhage associated with an abortion may indicate retained pregnancy tissue; placental abnormalities (such as placenta accreta); cervical laceration; DIC; or uterine perforation, atony, or rupture. Following an abortion, patients typically have 1 to 2 weeks of bleeding that does not substantially decrease hemoglobin levels (13). For patients with ongoing heavy bleeding, suction evacuation is recommended. If the bleeding has decreased on its own and the patient is clinically stable, expectant management or medical management with misoprostol (800 μg buccally or vagi- nally) or methylergonovine (0.2 mg intramuscularly) may be considered as well.
The need for transfusion following induced abortion is rare and only seen in 0.2% of both medical and surgical cases (11,14,15). Transfusion should be considered in patients according to standard criteria used in other clinical situations, but suction evacuation is the mainstay of treating excessive vaginal bleeding.
If there is evidence of intra-abdominal free fluid on ultrasound, then uterine perforation or ruptured ectopic pregnancy should be considered in the differential diagnosis, and further surgical intervention may be necessary.
Infection
Endometritis occurs in including in vitro fertilization, heterotopic pregnancies are becoming more common. In women presenting for emergent care following an abortion, a pelvic ultrasound can evaluate for evidence of retained tissue or signs of ectopic pregnancy, such as an adnexal mass or intra-abdominal free fluid.
Occasionally, when a pregnancy continues following an attempted abortion, a patient may decide to continue the pregnancy. Misoprostol is a known teratogen, but mifepristone alone has unknown risks to the pregnancy (26-28). There is less concern about the teratogenicity of medications used in surgical abortion, but instrumentation of the uterine cavity may increase the risk of infection or other complications for an ongoing pregnancy. Patients who are considering continuing a pregnancy following a failed abortion should be counseled about these risks.
Hematometra (blood clots accumulating in the uterus)
Uterine perforation
Cervical laceration
Abortion in the Second Trimester
Cervical dilation and/or softening can be accomplished with mechanical osmotic dilators (e.g., laminaria) and/or misoprostol 1 to 2 days prior to a second trimester abortion. Occasionally following this cervical preparation, patients can develop heavy bleeding or symptoms of labor and may present to the emergency department prior to their scheduled abortion.
In this setting, delivery of the fetus may occur with or without the delivery of the placenta. Retained placenta in this situation usually requires urgent surgical evacuation of the uterus to minimize bleeding.CONTRACEPTION FOLLOWING ABORTION
Ovulation can occur as early as 2 to 3 weeks following first trimester abortion (29), so it is recommended to start birth control as soon as possible after an abortion is completed. Immediate initiation of contraception including the insertion of an intrauterine device (IUD) or subdermal implant during the same visit as a surgical abortion is a safe and effective practice that is becoming more common in the United States. Patients who have an IUD in place following their abortion may suffer the same complications as other abortion patients, but pain, irregular or heavy bleeding, and infection are unlikely to be specifically caused by the IUD. For this reason, it is not usually necessary or helpful to remove the IUD while these complications are being evaluated and treated. An IUD does not need to be removed in the setting of endometritis unless the patient does not show clinical improvement with the use of antibiotics (30,31).
SUMMARY
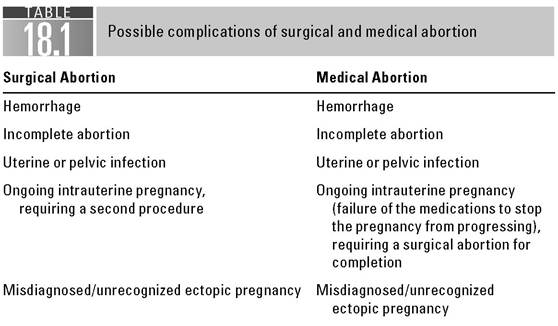
Although an induced abortion is safe, the fact that this procedure is common means that women presenting with complications will be encountered in the emergency department. The recommendations described in this chapter will help clinicians provide timely, appropriate, and effective treatment for women experiencing these complications (Table 18.1).
References
1. Owings MF, Kozak LJ. Ambulatory and inpatient procedures in the United States, 1996. Vital Health Stat. 1998;13(139):1-119.
2. Judge DE. Reported voluntary abortions: numbers inch downward. J Watch Women Health. 2009;14;11-12.
3. Finer LB, Henshaw SK. Disparities in rates of unintended pregnancy in the United States, 1994 and 2001. Perspect Sex ReprodHealth. 2006;38(2):90-96.
4. Henshaw SK. Unintended pregnancy and abortion: a public health perspective.
In: Paul M, et al., ed. A Clinician’s Guide to Medical and Surgical Abortion. New York, NY: Churchill Livingstone; 1999:11-22.5. Grimes DA. Risks of mifepristone abortion in context. Contraception. 2005;71(3):161.
6. Bartlett L, Berg C, Shulman H, et al. Risk factors for legal induced abortion-related mortality in the United States. Obstet Gynecol. 2004;103(4):729-737.
7. Christiansen LR, Collins KA. Pregnancy-associated deaths: a 15-year retrospective study and overall review of maternal pathophysiology. Am J Forensic Med Pathol. 2006;27(1):11-19.
8. van Lerberghe W, ed. The World Health Report 2005: Make Every Mother and Child Count. Geneva, Switzerland: WHO; 2005.
9. Cates W Jr, et al. Legalized abortion: effect on national trends of maternal and abortion-related mortality (1940 through 1976). Am J Obstet Gynecol. 1978;132(2): 211-214.
10. Grimes DA. Medical abortion in early pregnancy: a review of the evidence. Obstet Gynecol. 1997;89(5, pt 1):790-796.
11. Spitz IM, et al. Early pregnancy termination with mifepristone and misoprostol in the United States. N Engl JMed. 1998;338(18):1241-1247.
12. Schaff EA, et al. Low-dose mifepristone 200 mg and vaginal misoprostol for abortion. Contraception. 1999;59(1):1-6.
13. Thonneau P, et al. A comparative analysis of fall in haemoglobin following abortions conducted by mifepristone (600mg) and vacuum aspiration. Hum Reprod. 1995;10(6): 1512-1515.
14. Haskell WM. Surgical abortion after the first trimester. In: Paul M, et al., ed. A Clinician’s Guide to Medical and Surgical Abortion. New York, NY: Churchill Livingstone; 1999:123-138.
15. Tietze C. InducedAbortion: A Worldwide Review. New York, NY: Guttmacher Institute; 1996.
16. Shannon C, et al. Ectopic pregnancy and medical abortion. Obstet Gynecol. 2004;104(1): 161-167.
17. Workowski KA, Berman SM. Sexually transmitted diseases treatment guidelines, 2006. MMWR Recomm Rep. 2006;55(RR-11):1-94.
18. Clostridium sordellii toxic shock syndrome after medical abortion with mifepristone and intravaginal misoprostol—United States and Canada, 2001-2005.
MMWR Morb Mortal Wkly Rep. 2005;54(29):724.19. Cohen AL, et al. Toxic shock associated with Clostridium sordellii and Clostridium perfringens after medical and spontaneous abortion. Obstet Gynecol. 2007;110(5):1027-1033.
20. Fischer M, et al. Fatal toxic shock syndrome associated with Clostridium sordellii after medical abortion. NEnglJMed. 2005;353(22):2352-2360.
21. Stubblefield PG, Grimes DA. Septic abortion. NEnglJMed. 1994;331(5):310-314.
22. Kaunitz AM. First trimester abortion technology. In: Corson S, ed. Fertility Control. Boston, MA: Little, Brown and Company; 1985:63.
23. Grimes DA, Cates W Jr. Complications from legally-induced abortion: a review. Obstet Gynecol Surv. 1979;34(3):177-191.
24. Guest J, et al. Randomised controlled trial comparing the efficacy of same-day administration of mifepristone and misoprostol for termination of pregnancy with the standard 36 to 48 hour protocol. BJOG. 2007;114(2):207-215.
25. Kaunitz AM, et al. Abortions that fail. Obstet Gynecol. 1985;66(4):533-537.
26. Gary MM, Harrison DJ. Analysis of severe adverse events related to the use of mifepristone as an abortifacient. Ann Pharmacother. 2006;40(2):191-197.
27. Sitruk-Ware R, Davey A, Sakiz E. Fetal malformation and failed medical termination of pregnancy. Lancet. 1998;352(9124):323.
28. Orioli IM, Castilla EE. Epidemiological assessment of misoprostol teratogenicity. BJOG. 2000;107(4):519-523.
29. Vorherr H. Contraception after abortion and post partum: an evaluation of risks and benefits of oral contraceptives with emphasis on the relation of female sex hormones to thromboembolism and genital and breast cancer. Am J Obstet Gynecol. 1973;117(7):1002-1025.
30. Rinehart W. WHO Updates Medical Eligibility Criteria for Contraceptives. Baltimore, MD: Johns Hopkins University; 2004.
31. World Health Organization. Improving access to quality care in family planning. 3rd Ed. Medical Eligibility Criteria for Contraceptive Use. Geneva, Switzerland: World Health Organization (WHO); 2003.