Drug Therapy in Pregnancy
Thanh T. Hogan, Kristina E. Ward, Andrea L. McKeever, William Renfro, and Linda Hastings
Ethical and legal limitations preclude drug studies in pregnant women, leaving the health care provider with little reliable information to base clinical decisions of drug use during pregnancy.
As a result, some clinicians practice “therapeutic nihilism” where nothing is prescribed for the pregnant patient (1,2). However, avoiding medication use during pregnancy at all cost is not necessarily desirable. If left untreated, many conditions may jeopardize the health of the mother and/or the fetus. This chapter reviews the relative safety of common medications prescribed during pregnancy.FOOD AND DRUG ADMINISTRATION PREGNANCY CATEGORIES
During the 1960s and 1970s, the tragedy of thalidomide use, which resulted in thousands of babies being born with severe limb defects, heightened awareness of medication use in pregnant women.
In 1980, the Food and Drug Administration (FDA) required that the labeling of prescription drugs include information about the use in pregnancy. Five categories were established to indicate a drug’s potential for causing birth defects. The category is assigned upon the drug’s initial approval by the FDA. As a result, information available to categorize the drugs is usually limited human data and animal studies. This information can be found in the precautions section of the package insert. A description of the current categories is summarized in Table 17.1 (3).
This classification system was an important step for assisting the clinician in identifying potential teratogenic prescription drugs. However, the categories lack specific details to assist clinicians in prescribing to pregnant women and does not address timing of pregnancy, appropriate dosage of the drugs, or use during lactation. Additionally, health care professionals often mistakenly believe that there is a gradation of risk across the categories, assuming that a drug in category B is safer than one in category C which is safer than one in category D.
However, by definition, category C drugs generally have the least data (Table 17.2) and can represent risks of unknown magnitude. A new labeling system has been under development at the FDA since 1977. However, the proposed regulation, which would provide more information on fertility, pregnancy, and breastfeeding, has not yet been finalized. In the meantime, health care professionals cannot assume relative safety for category C drugs. All available information must be carefully reviewed and the risks and benefits of each drug evaluated.TERATOGENESIS
Although initially designed to provide guidance, the current labeling system is often used to estimate teratogenic risk. Teratogenesis is defined as the dysgenesis of fetal organs as evidenced either structurally or functionally (e.g., brain functions) (4). Whether a given agent can induce congenital malformations in animals or humans is based on three fundamental principles of teratogenesis first described in 1959 (5). These include the particular dose of the substance, the susceptibility of the species, and the embryo’s stage of development at the time of exposure.
TIH FDA Pregnancy Categories (3)
Category A
Adequate, well-controlled studies in pregnant women have not shown an increased risk of fetal abnormalities.
Category B
Animal studies have revealed no evidence of harm to the fetus; however, there are no adequate and well-controlled studies in pregnant women.
or
Animal studies have shown an adverse effect, but adequate and well-controlled studies in pregnant women have failed to demonstrate a risk to the fetus.
Category C
Animal studies have shown an adverse effect and there are no adequate and well-controlled studies in pregnant women.
or
No animal studies have been conducted, and there are no adequate and well-controlled studies in pregnant women.
Category D
Studies, adequate, well-controlled, or observational, in pregnant women have demonstrated a risk to the fetus.
However, the benefits of therapy may outweigh the potential risk.Category X
Studies, adequate, well-controlled, or observational, in animals or pregnant women have demonstrated positive evidence of fetal abnormalities. The use of the product is contraindicated in women who are or may become pregnant.
TABLE
Animal and Human Risk Exposure and Pregnancy Categories
| Pregnancy Category | Animal Exposure | Human Exposure |
| A | - | - |
| B | + | - |
| - | Unknown | |
| C | + | Unknown |
| Unknown | Unknown | |
| D (benefit may outweigh risk) | + | + |
| X (contraindicated) | + | + |
Note: -, no risk; +, known risk.
The timing of fetal exposure is the most important determinant of teratogenesis. There are four critical periods in human development in which drugs may adversely affect the fetus (6). Days 0 to 7 represent the preimplantation phase, in which fertilization and zygote formation occur. Exposure to teratogens during this period usually results either in death of the embryo or in replacement of damaged cells by undifferentiated cells that go on to develop normally. During organogenesis (days 14 to 60), the embryo is at its peak sensitivity to teratogens. Most morphologic congenital abnormalities are thought to be produced during this interval. As organogenesis ends, susceptibility to anatomic abnormalities declines. Minor structural malformation may still occur throughout histogenesis. Exposures during the fetal development period are associated with a much lower risk of major birth defects because most major organ systems are well developed by this time (7,8). Problems that do occur usually involve growth or functional deviations.
PREGNANCY REGISTRIES
Beyond the current pregnancy categories, relevant clinical data on medications during pregnancy are found through a modest group of anecdotal case reports, case studies, observational studies, and retrospective chart reviews.
Despite this lack of information about the effects of medications on the fetus, medication use during pregnancy appears to be increasing. A study conducted by the FDA in 1995 found that women under 35 years of age consumed on average three prescriptions during the course of their pregnancy (9). For those over 35 years of age, the number of prescriptions increased to five. A 2003 study estimates 80% of pregnant women taking some over-the-counter (OTC) or prescription medications (10). Known use of prescription and OTC medications in pregnant women, along with inadvertent exposures to medications during pregnancy (i.e., woman is unaware she is pregnant while taking a medication), provide another opportunity to collect relevant clinical data, through pregnancy registries.A pregnancy registry is a surveillance study that enrolls pregnant women after they have been exposed to a medication and follows the women until the birth of the baby (11). Although regulations continue to be reviewed, pregnancy registries are currently voluntary with most administered through pharmaceutical companies and a few administered through specific organizations (i.e., hospitals, universities). Data from babies born to women taking a particular medication are compared to those born to women not taking the medicine. Patients may enroll directly to some but the majority require physician enrollment. A listing of available pregnancy registries is available on the FDA webpage.
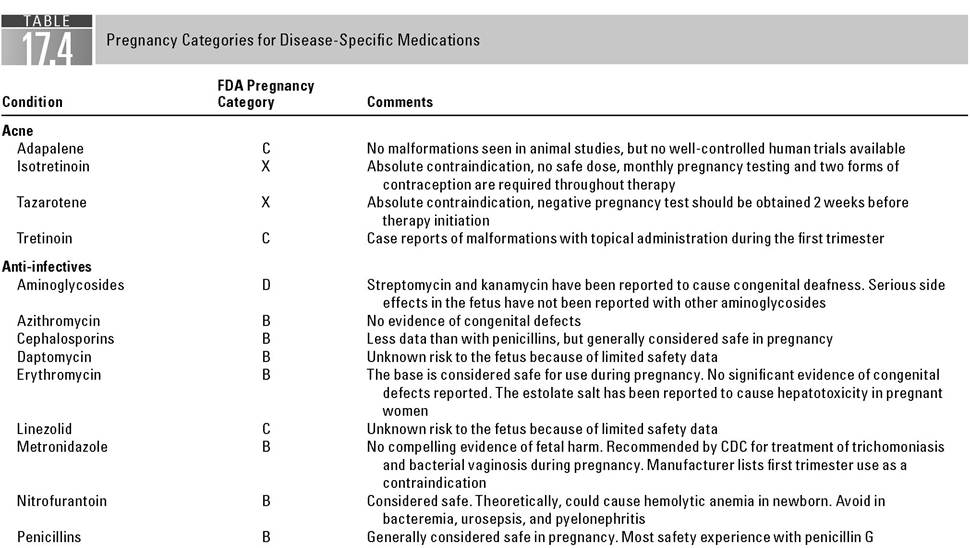
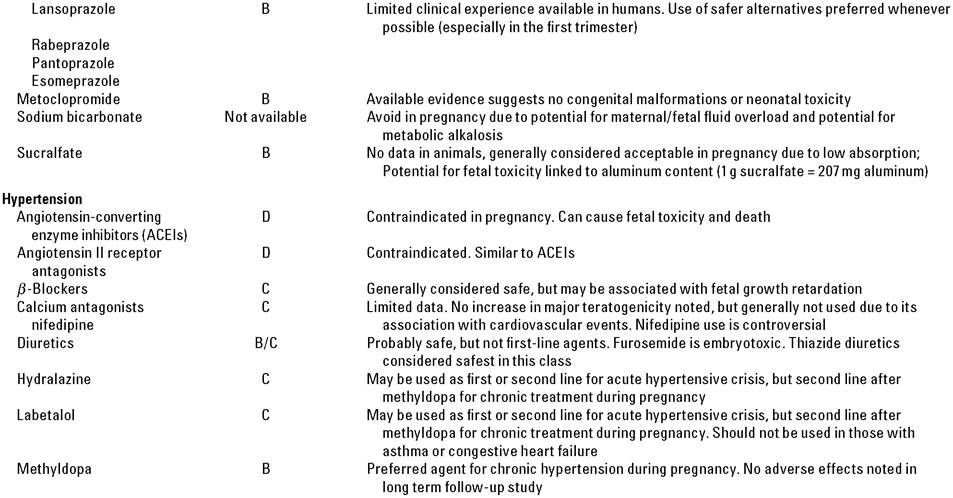
To date, very few drugs are known to cause fetal harm (Table 17.3). Nonetheless, it is virtually impossible to prove drugs safe for use in pregnancy because no well-designed long-term studies can be ethically conducted. This leaves a huge void between known teratogenesis and known safety. Although this void is difficult to fill with our current labeling system and available literature, some clinically relevant conclusions can be reached (Table 17.4).
Anti-infectives
Although penicillins and penicillin derivatives cross the placenta, they are considered safe for use in the nonallergic patient during pregnancy (12-14).
A large study involving 3,546 fetal exposures to penicillin derivatives (primarily penicillin G) during the first trimester of pregnancy found no link to major or minor malformations (15). Other reports and the wide use of this class of drugs during pregnancy support this finding (14,16). Data on the newer penicillins (i.e., ticar- cillin and piperacillin) are lacking. However, the FDA places each of these agentsMedications Absolutely Contraindicated in Pregnancy (Category X)
Acetretin
Androgens
Estrogens
Dihydroergotamine
Finasteride
Goserelin
HMG-CoA Reductase Inhibitors
(Atorvastatin, Fluvastatin, Lovastatin, Pravastatin, Simvastatin)
Leuprolide
Megestrol
Progesterone
Ribavirin
Thalidomide
Warfarin
Yohimbine
in risk category B with the other penicillins. It is known that ticarcillin and piperacillin rapidly cross the placenta, but no reports of congenital defects with these agents have been located (14). Beta-lactamase inhibitors (i.e., clavulanate, sulbactam, tazobactam) are added to penicillin derivatives to broaden their spectrum of activity. Several studies have failed to find a teratogenic effect associated with exposure to clavulanate; however, the Michigan Medicaid Surveillance Study found a possible association with spina bifida (14,17-19). Limited data exist regarding sulbactam and tazobactam; however, available data suggest no evidence for concern (14,20).
The majority of cephalosporins readily cross the placenta and have pharmacokinetic parameters very similar to the penicillins. In the retrospective Michigan Medicaid Surveillance Study, increased numbers of birth defects were found for cefaclor, cephalexin, and cephradine, but not other cephalosporins (14,19). However, a large, population-based, case-control study assessing the incidence of birth defects with seven cephalosporins found no association (21). Generally, the cephalosporins are considered safe for use during pregnancy and are the preferred alternative in patients with nonanaphylactic penicillin sensitivity (14,20,21).
Where it covers the appropriate microbial spectrum, erythromycin base should be used in penicillin-allergic patients demonstrating immediate-type sensitivity.The macrolide, erythromycin, has been used during pregnancy with no known increased risk to the mother or the fetus (14,20). Although the drug crosses the placenta, plasma levels are low in the fetus (22). One salt of erythromycin, the estolate form, is considered contraindicated during pregnancy because of a reported 10% reversible incidence of hepatotoxicity (increases in serum aspartate
| QuinupristinZdaIfopristin | C | Unknown risk to the fetus due to limited safety data |
| Quinolones | C | Avoid use during pregnancy. Have been associated with arthropathies in animals and children |
| Tetracyclines | D | Avoid if possible, especially during last half of pregnancy |
| Trimethoprim/ | C | Trimethoprim inhibits folic acid synthesis. Sulfonamides can induce kernicterus in the |
| Sulfamethoxazole | newborn if used late in pregnancy | |
| Vancomycin | C | Generally not thought to be teratogenic. Linksto ototoxicity and nephrotoxicity not established |
| Analgesia | ||
| Acetaminophen | B | Analgesic and antipyretic of choice in pregnancy |
| Aspirin | C | May produce adverse effects in the mother and the fetus. Can inhibit labor if used late in pregnancy. Avoid if possible |
| Codeine | C/D | High doses or long term use is not recommended. Likelyto cause neonatal respiratory depression and withdrawal if used near term |
| Nonsteroidal anti | B/C/D | No association to date with congenital malformations. Cantheoretically inhibit labor if used |
| inflammatories | late in pregnancy. May cause constriction or closure of the ductus arteriosus if used near term | |
| Hydromorphone | B/D | Not associated with congenital defects. High doses or long-term use is not recommended. Likely to cause neonatal respiratory depression and withdrawal if used near term |
| Fentanyl | C/D | Not associated with congenital defects. Likely to cause neonatal respiratory depression and withdrawal if used near term |
| Morphine | C/D | Not associated with congenital defects. High doses or long-term use is not recommended. Likely to cause neonatal respiratory depression and withdrawal if used near term |
| Oxycodone | B/D | Not associated with teratogenic effects. High doses or long-term use is not recommended. Likely to cause neonatal respiratory depression and withdrawal if used near term |
/continued)
/continued)
aminotransferase) occurring in the mother (14,20). Less evidence is available for clarithromycin and azithromycin. While teratogenic in animals, clarithromycin has, thus far, failed to demonstrate birth defects in small, epidemiologic studies of human pregnancy (14,23-25). Similar rates of major malformations and spontaneous abortions were observed with azithromycin and matched controls in a small study (26).
Tetracyclines are known to cause numerous potential problems to the mother and the fetus and should be avoided during pregnancy (14,20). Nearly all tetracyclines readily cross the placenta (14). Tetracycline is well-known to cause yellow-brown discoloration of the teeth after in utero exposure because of its ability to chelate calcium orthophosphate, which becomes incorporated into bones and teeth during calcification (14,20). Severe dysplasia of the teeth and inhibition of bone growth also have been demonstrated. These effects are more common when the drug is taken in the second and the third trimesters, when bone mineralization occurs (14,20). Tetracycline has also been reported to induce limb anomalies, inguinal hernia, and hypospadias (14). Potentially fatal maternal liver and renal toxicities, although rare, have been attributed to tetracycline (14,20).
Sulfonamides cross the placenta and accumulate in significant quantities in the fetus (14,20). Teratogenicity has been shown in some animal species, but a link to human malformations has not been demonstrated even in large trials
(15.19). Sulfonamides should not be administered close to delivery as they can cause jaundice and kernicterus in the newborn through displacement of bilirubin from albumin-binding sites. Earlier in pregnancy, the placenta is capable of clearing the free unconjugated bilirubin; however, the clearing mechanism is no longer available at birth (14). Hemolysis may occur in the fetus or neonate because of relative deficiencies in glucose-6-phosphate dehydrogenase (G-6-PD)
(14.20).
Trimethoprim used alone or in combination with sulfonamides should be avoided during pregnancy. The drug is a folic acid antagonist, a group of agents known to be potentially teratogenic. The Michigan Medicaid Surveillance Study and other retrospective reviews have suggested an increase in incidence of birth defects (cardiovascular and oral clefts) potentially up to twofold to threefold (14). Recent evidence suggests an association between trimethoprim and neural tube defects, congenital heart defects, and oral clefts (27-30).
Nitrofurantoin is not associated with an increased risk of birth defects in the neonate; however, administration of the drug close to delivery theoretically may cause hemolytic anemia in the newborn because of G-6-PD and glutathione deficiencies (14,19,20). Nitrofurantoin is popular for the treatment and prophylaxis of urinary tract infections in pregnancy but should not be used when bacteremia or urosepsis is suspected because of low therapeutic serum concentrations or in pyelonephritis because of inadequate tissue penetration (14,29,31).
Metronidazole crosses the placenta and appears in maternal and cord blood in equal amounts. Because the drug is mutagenic in bacteria and carcinogenic in rats, some recommend avoiding it in pregnancy (14). However, there are no good human data implicating metronidazole as a teratogen or a carcinogen. One human study reported 31 first-trimester exposures leading to four cases of birth defects (15). However, several more recent studies suggest that metronidazole does not adversely affect the fetus (32-35). Metronidazole has been recommended for the treatment of bacterial vaginosis and trichomoniasis (36). To date, the relative risk of metronidazole’s use in pregnancy is unknown, and its use in pregnancy is controversial.
The aminoglycosides are frequently used to treat serious infections during pregnancy and have not caused fetal malformation (13,37). However, ototoxicity and deafness have been reported in infants exposed to streptomycin and kanamycin in utero (14,37). Gentamicin, amikacin, and tobramycin all cross the placenta and appear in the fetal circulation. Highest fetal concentrations are found in the kidneys and urine. Pharmacokinetics of aminoglycosides are usually significantly altered in pregnant women. Careful maternal serum level monitoring is required to limit fetal exposure yet assure therapeutic concentrations in the mother.
The fluoroquinolones distribute well to bone tissue and cartilage and have been associated with arthropathies in animals and in human children (14,31). However, some available data have failed to find this effect in the children of the women exposed to fluoroquinolones during pregnancy (20,38-40). Because of the availability of safer alternatives, fluoroquinolones should generally be avoided in pregnancy.
Vancomycin is not thought to be teratogenic (14). Vancomycin was present in significant amounts in the cord blood of a mother who received vancomycin (41). Ototoxicity and nephrotoxicity are potential problems, and a few cases have been reported; however, the relationship of these defects to vancomycin therapy has not been clearly established (14).
Limited data are available regarding the safety of Iinezolid, daptomycin, and quinupristin/dalfopristin in pregnant women. Linezolid has a low molecular weight; therefore, distribution across the placenta is likely. Animal studies have shown toxicity (i.e., total litter loss, decreased fetal weight, increased fusion of costal cartilage) at doses 6.5 times the expected human exposure and maternal toxicity (reduced body weight gain) at doses 0.64 times the expected human exposure (42). The manufacturer reports three cases of women found to be pregnant after linezolid study enrollment (two patients had spontaneous abortions and one delivered a healthy infant). Because of the unknown safety profile of lin- ezolid in pregnancy, use should be considered only if the potential benefit to the patient outweighs the potential risks. In animals, quinupristin/dalfopristin was not teratogenic or embryotoxic or fetotoxic (14). No case reports of use in pregnant women are published. Two case reports of daptomycin use during the third trimester are published (43,44). In both reports, no adverse neonatal outcomes were reported.
Analgesia
Although it crosses the placenta, acetaminophen has been widely used during pregnancy and is not teratogenic. Because acetaminophen does not affect platelet function or prostaglandin synthesis, short-term use of acetaminophen at therapeutic doses is considered the analgesic and antipyretic of choice in pregnant women (14,45,46). Aspirin is more controversial. The Collaborative Perinatal Project failed to associate 14,864 first-trimester fetal exposures to aspirin with malformations (15). Use in the first trimester has not been associated with birth defects, low birth weight, or still birth (47,48). However, aspirin can result in a narrowing of the ductus arteriosus when used in the third trimester (14). Women taking aspirin also run the risk of maternal and newborn bleeding through platelet inhibition, inhibition of uterine contractions, and prolonged labor through prostaglandin inhibition (47,49). Aspirin should be avoided, especially late in pregnancy.
The nonsteroidal anti-inflammatory drugs (NSAIDs) have not been linked with congenital malformations and have been used during pregnancy (47,50-53). Like aspirin, NSAIDs are prostaglandin inhibitors; therefore, they can prolong labor when used late in pregnancy and cause constriction or early closure of the ductus arteriosus (54,55). NSAIDs can cause oligohydramnios from decreased fetal urine output and renal dysfunction (47,51,56).
For severe pain, opioid analgesics have been used and are not associated with any major or minor malformations (14,15,57). Opioids may cause neonatal respiratory depression and withdrawal when used near delivery. Use for prolonged periods or in high doses at term is not recommended.
Asthma
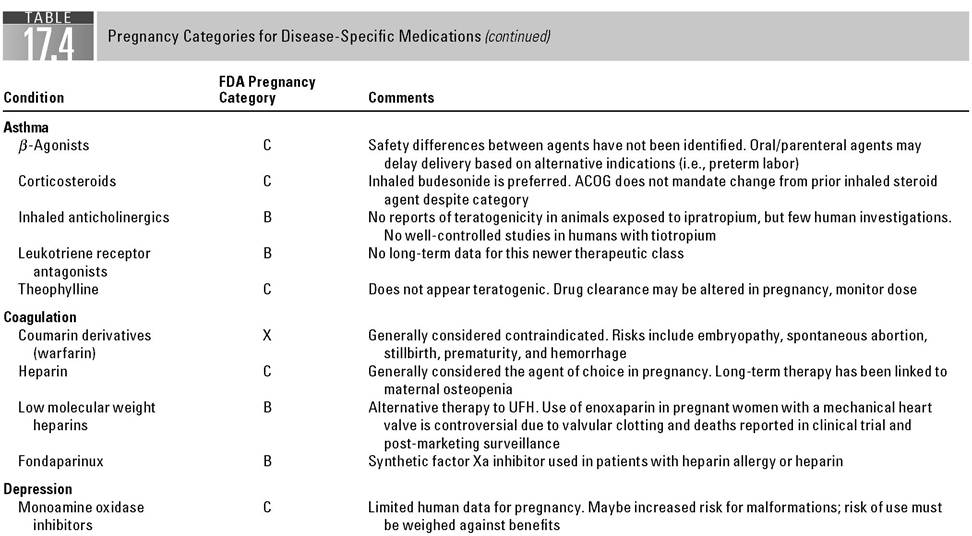
For most patients, the management of asthma is much the same during pregnancy as it is in the nonpregnant state. When left untreated, severe persistent asthma has the potential to lead to serious complications for both the mother and the child (58). In general, the inhalation route is preferred over oral or parenteral administration to limit localized absorption of the agent to the lungs.
Short-acting, beta-agonists, such as albuterol, are considered first-line therapy for patients with mild to moderate disease. There appears to be no safety differences between available inhaled beta-agonists; however, the use of the oral or parenteral route should be avoided because of limited safety data and the potential to delay delivery (terbutaline is used for tocolysis). Inhaled corticosteroids are a major component of asthma therapy for all patients, including those who may be pregnant. Budesonide is the preferred inhaled corticosteroid; however, the American College of Obstetricians and Gynecologists (ACOG) states that inhaled corticosteroids other than budesonide may be continued if symptoms were well-controlled prior to pregnancy (58).
Cromolyn is not known to be teratogenic (59,60). Nedocromil is not expected to be teratogenic (14). Both have minimal systemic absorption and associated adverse effects. The leukotriene receptor agonists zafirlukast and montelukast are not teratogenic in animals (14). However, there are limited safety data in humans. These agents may be considered alternative add-on controller medications in patients with moderate persistent asthma not stabilized on low-dose inhaled corticosteroids (58).
There are limited data for the use of ipratropium during pregnancy; however, animal models have shown no resulting fetal malformation during exposure (14). Compared to beta-agonists, ipratropium provides no significant benefit when safety data are considered, and as such, it is not considered first-line therapy during pregnancy (58,61). Theophylline does not appear to cause adverse fetal outcomes; however, use of theophylline in pregnancy should be undertaken with caution because theophylline pharmacokinetics change during pregnancy (60,62). Serum concentrations should be monitored frequently and doses adjusted accordingly.
Emergency management is the same as for nonpregnant patients because of the overwhelming benefits for the mother and the fetus and should consist of oxygen administration, use of nebulized beta-agonists and ipratropium, oral or intravenous corticosteroids, and intravenous agents when indicated (61).
Coagulation
Thromboembolism is a serious complication of pregnancy occurring in 1 to 2 per 1,000 gestations and accounts for about 10% of deaths during gestation. About 65% of thromboembolic events occur during the antepartum period, and this risk continues with an incidence of 35% until about 6 weeks postpartum. Most emboli (80%) are venous in nature deep vein thrombosis (DVT) with the remaining 20% occurring as pulmonary emboli. Risk factors for venous thromboembolism (VTE) during normal pregnancy include increases in normal endogenous clotting factors, increased venous pooling, and compression of the iliac vein. Additive risk factors are age >35 years, prior history of VTE, obesity, genetic thrombophilia (factor V Leiden deficiency, antithrombin deficiency), preeclampsia, smoking, diabetes, anemia, Lupus, coronary disease, multiple gestation, hyperemesis, fluid/electrolyte imbalance, sickle cell disease, recent surgery, and prolonged immobility (63,64).
Based on the American College of Chest Physicians (ACCP), thromboembolism should be managed by using these comorbid factors (65,66):
1. Pregnant women with previous VTE prior to pregnancy require prophylactic unfractionated heparin (UFH) or low molecular weight heparin (LMWH) such as dalteparin, enoxaparin, or tinzaparin. Aspirin should be discontinued. Additionally, graduated elastic compression stockings (GECS) can be used as prophylaxis (67).
2. Women on warfarin for VTE who become pregnant should discontinue warfarin and begin treatment with UFH or LMWH in doses described below.
3. Women on anticoagulation for prosthetic heart valves should receive treatment with adjusted dose of UFH or LMWH.
4. Pregnant women with high-risk valves (older generation valve in the mitral position or history of thromboembolism) should consider therapy with oral anticoagulants instead of heparin.
5. Pregnant women with VTE during pregnancy should receive adjusted UFH as a bolus and then continuous infusion or UFH every 12 hours to achieve target activated partial thromboplastin time (PTT) values for at least 5 days and continue the same until delivery.
6. Pregnant women with prosthetic valves and high risk of VTE and/or preeclampsia should receive adjusted dose UFH or LMWH plus aspirin 75 to 100 mg per day.
The pharmacokinetics of heparin is altered in pregnancy to the point that significant increases in doses or frequency are required to keep aPTT values therapeutic. Therapeutic ranges for aPTT vary with the testing procedure run at different institutions (66,68). Women in labor should receive UFH instead of LMWH due to its longer duration and lack of a reversal agent (63). Protamine is the reversal agent for bleeding from heparin therapy. Approximately 1 mg of protamine reverses 100 units of heparin. In calculating the total dose ofprotamine required for reversal, only consider the amount of heparin given in the last several hours, as the duration of heparin is only 4 to 6 hours (64,66).
For women who develop adverse reactions to UFH or LMWH, the options are limited. Fondaparinux, a selective antifactor Xa, has limited and conflicting information in pregnancy but may be considered the treatment of choice if heparin products are not advised (allergy to heparin or heparin induced thrombocytopenia) (3,67,69,70).
Postpartum management should resume 12 hours after epidural or 24 hours after cesarean section. GECS devices should remain in place. If warfarin is indicated for continued treatment, it may be restarted 2 weeks after delivery and continued for 3 to 6 months after delivery (63,67).
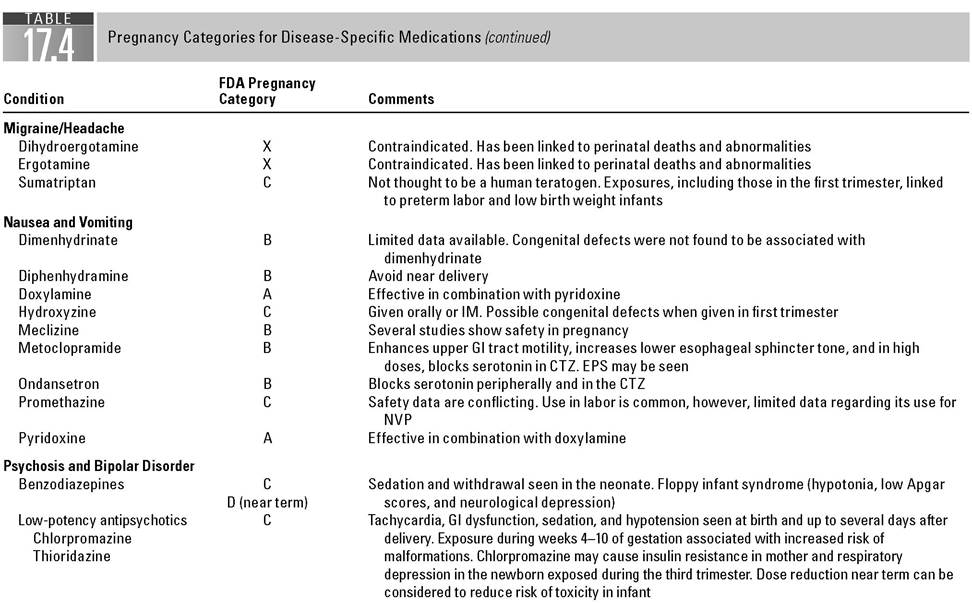
Depression
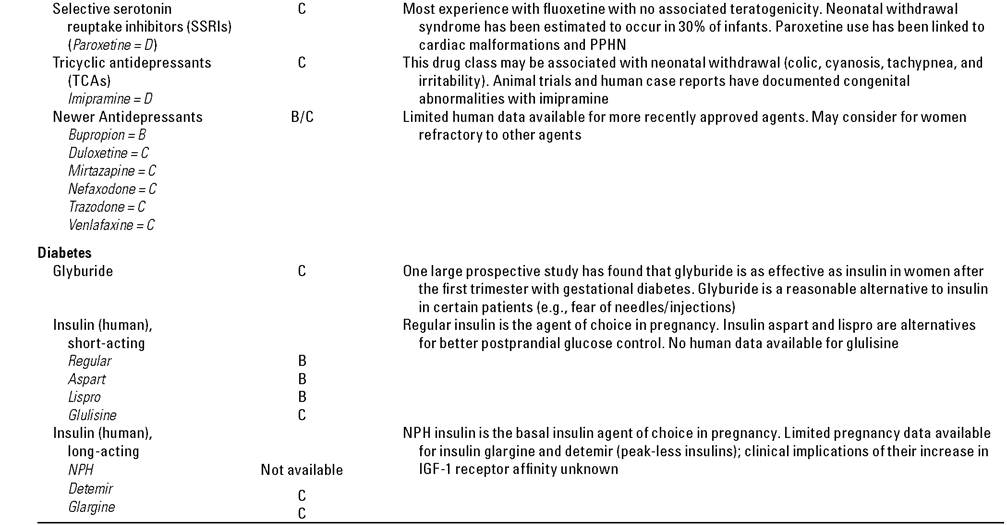
Recent data indicate that as many as 19% of women will have a major depressive episode at some point during pregnancy or the postpartum period (71). Untreated depression during pregnancy is associated with poor outcomes including low birth weight infants, preterm delivery, lower Apgar scores, poor prenatal care, and an increased risk of fetal abuse, neonaticide, or suicide (72,73). Treatment of maternal depression during pregnancy and the postpartum period is recommended, despite the potential risks to the fetus and the newborn (72,74). Selective serotonin reuptake inhibitors (SSRIs) have replaced tricyclic antidepressants (TCAs) as first-line treatment for depression in the
general population (75). Of the SSRIs, fluoxetine has been the most commonly used and studied in pregnancy. Others are paroxetine, sertraline, citalopram, escitalopram, and fluvoxamine, as well as serotonin norepinephrine reuptake inhibitors (SNRIs) such as venlafaxine and duloxetine. The use of SSRI and SNRI drugs during gestation does not appear to be associated with an increased risk of major fetal anomalies (75,76).
Nevertheless, the safety of SSRIs is now in question with an emerging picture of neonatal problems such as neonatal behavioral syndrome, congenital heart disease, and persistent pulmonary hypertension (PPHN). Exposure to SSRIs in late pregnancy is associated with a threefold increased risk of neonatal behavioral syndrome, also termed neonatal abstinence syndrome (75,77). Signs and symptoms of this behavioral syndrome include jitteriness, poor muscle tone, tachycardia, hypoglycemia, hypothermia, respiratory distress, weak or absent cry, low Apgar scoring, and desaturation during feeding (75,77,78). This has been estimated to occur in approximately 30% of infants exposed to SSRIs in utero (75,77).
In December 2005, the FDA issued a public health advisory regarding the potential risk of ventricular septal defects (VSDs) in fetuses exposed to paroxetine in the first trimester (79). There are two reports from GlaxoSmithKline based on a Swedish national registry and a U.S. insurance claims database that have raised concerns about a one-and-a-half- to twofold increased risk of congenital cardiac malformations (atrial and ventricular septal defects) associated with first-trimester paroxetine exposure (79). As a result, the manufacturer changed the pregnancy category rating from C to D. More recently, the cardiovascular teratogenic effect of SSRI use during the first trimester of pregnancy was examined in two large studies (73,80). These studies found no increase in cardiovascular defects associated with paroxetine use.
In July 2006, FDA issued another public health advisory regarding SSRI use in pregnancy and the potential risk of PPHN in newborns (81). One study that FDA cites found that PPHN was six times more likely in neonates whose mothers took an SSRI after the 20th week of pregnancy (82). A more recent study has found no evidence of an increase in the risk for PPHN associated with SSRI use (83).
The atypical antidepressants include bupropion, duloxetine, mirtazapine, nefazodone, and venlafaxine. Information on the use of these medications in pregnancy is limited (72).
Diabetes
Diabetes during pregnancy has the potential to cause complications, such as macrosomia, hyperbilirubinemia, increased risk for cesarean delivery, and birth trauma to the fetus (84-87). The initial management of pregestational and gestational diabetes is diet and exercise. Drug therapy may be warranted if inadequate blood glucose control occurs. Based on the recommendations from the ACOG, the drug of choice for the treatment of pregestational and gestational diabetes is exogenous human insulin. Insulin does not cross the placenta unless bound to IgG antibody or forced through the placenta by high perfusion (e.g., fast infusion rate); therefore, fetal exposure is minimized (88). Traditionally, regular human insulin has been used to manage blood glucose levels with the addition of NPH human insulin (isophane suspension) as a longer acting basal source. Newer rapid acting insulins (e.g., insulin aspart and lispro) have been evaluated and appear to be safe for pregnant patients in place of regular insulin; these insulin analogs may be beneficial if better postprandial glucose control is desired. Limited pregnancy data are available for the newer peak-less, long-acting insulins (e.g., insulin glargine and detemir); the clinical implications of their increase in insulin-like growth factor-I (IGF-1) receptor affinity are unknown and warrant further evaluation before routine use in pregnancy.
Sulfonylureas stimulate insulin secretion from pancreatic islet β-cells to lower serum glucose levels (86,87,89). Animal and human models document placental transport of first-generation sulfonylureas (i.e., chlorpropamide, tolbutamide, tolazamide). Their low molecular weight (270 to 277) facilitates the placental transport and results in fetal hyperinsulinemia, which can be profound and prolonged; therefore, their use in pregnancy is contraindicated. Documentation of second-generation sulfonylurea’s (i.e., glyburide, glipizide) use in pregnancy is primarily with glyburide (glibenclamide). Placental transport of glyburide in humans is minimal because of its significant plasma protein binding (95% to 99%) and relatively larger molecular weight (494). Results of a large randomized controlled study of 404 pregnant women post 11 weeks’ gestation and diagnosed with gestational diabetes suggest glyburide is a clinically effective alternative to insulin; additionally, the incidence of complications (e.g., macrosomia) and adverse events (e.g., hypoglycemia, fetal anomalies) is similar between these therapies (90). A secondary analysis of the study population further substantiates the previously stated findings and concludes that glyburide and insulin are equally effective for all levels of gestational diabetes severity (91). Therefore, glyburide is a reasonable therapeutic alternative to insulin (e.g., patients fearful of injections) for the treatment of gestational diabetes.
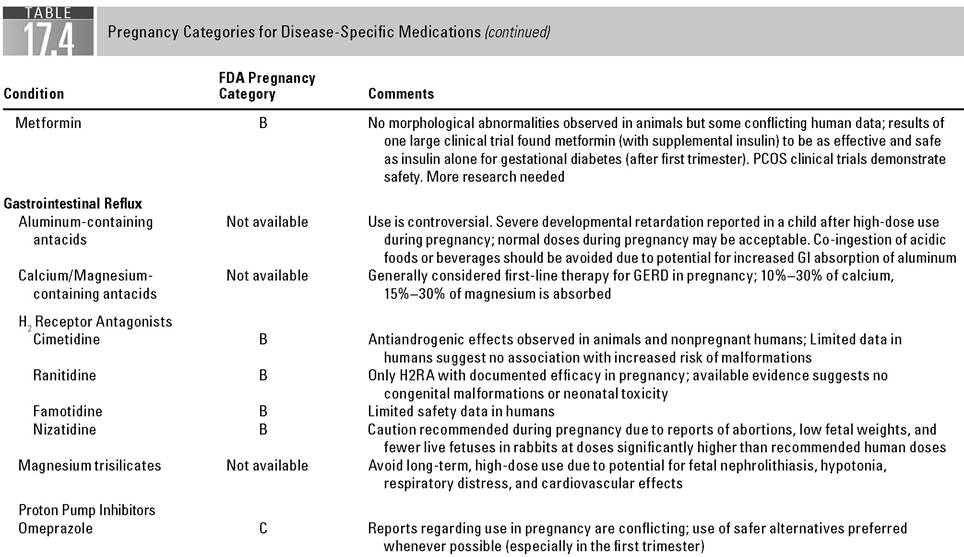
Biguanides (i.e., phenformin, metformin) decrease serum glucose levels by reducing hepatic glucose production, decreasing intestinal glucose absorption, and increasing peripheral tissue glucose uptake and utilization (86,87,89). Phenformin, metformin’s predecessor, was problematic because of its propensity to cause lactic acidosis in patients. Additionally, mouse embryo studies with phenformin documented fetal death and malformations (e.g., neural tube defect, craniofacial hypoplasia) at serum concentrations consistent with clinical use. Although metformin can cause lactic acidosis if used inappropriately (e.g., patients with severe renal insufficiency), it does not appear to be a major teratogen based on animal models. Animals exposed to metformin have experienced delayed closure of the neural tube; however, it has not translated into morphological abnormalities. One clinical trial comparing metformin, sulfonylureas, and insulin suggests that metformin may increase the occurrence of preeclampsia and perinatal death, but the investigators state these events could be attributed to other factors (e.g., obesity, metabolic syndrome) present in the metformin subjects (92). A more recent open-label study of 751 patients with gestational diabetes between 20 and 33 weeks’ gestation demonstrates that metformin (with supplemental insulin if needed) is as effective and safe as insulin therapy alone; the composite endpoint of neonatal hypoglycemia, respiratory distress, need for phototherapy, birth trauma, 5-minute Apgar score caffeinated and carbonated beverages late in the day, elevating the head of the bed, and not smoking. Drug therapies for gastroesophageal reflux disease (GERD) include antacids, sucralfate, histamine-2 receptor blockers, prokinetic agents, and proton pump inhibitors.
Antacids are considered first-line agents in managing GERD symptoms, neutralizing gastric acid to prevent esophageal damage and discomfort. Calcium and magnesium containing antacids are preferred, whereas aluminum-based antacids are controversial due to aluminum’s association with fetal neurological effects; however, systemic absorption of antacids is not significant. Likewise, magnesium trisilicate containing antacids (e.g., Gaviscon) should be avoided, as they have been associated with fetal complications such as nephrolithiasis, hypotonia, respiratory distress, and cardiovascular effects.
Like antacids, sucralfate is a first-line medication for GERD and is not generally systemically absorbed. It adheres to exposed mucosal lesions within the gastrointestinal tract until healing occurs and inhibits pepsin activity. Since sucralfate is an aluminum salt of a sulfated disaccharide (1 g sucralfate = 207 mg of aluminum), its use in pregnancy is controversial. Human fetal toxicity has not been reported, as findings of the Michigan Medicaid Surveillance Study of 229,101 pregnancies expected eight birth defects when only five were reported.
Histamine-2 receptor blockers are second tier therapeutic options, working to decrease gastric acid production. Of these agents, ranitidine is preferred, as available evidence suggests no congenital malformations or neonatal toxicity. Cimetidine’s antiandrogen activity as well as its hepatotoxicity, as substantiated by a case report of hepatitis in a newborn, limits its clinical utility in pregnancy. Animal studies with nizatidine are conflicting. One rabbit pregnancy study involving nizatidine reports abortions, low fetal weights, and fewer live fetuses at doses significantly larger than human doses; however, other animal studies do not substantiate these findings. Famotidine is a pregnancy category B but limited human pregnancy data exist.
Metoclopramide is a prokinetic agent that increases lower esophageal sphincter (LES) tone and gastric motility. Animal studies do not demonstrate teratogenic effects, whereas human evidence conflicts. Of the 192 first-trimester pregnancy exposures documented in the Michigan Medicaid Surveillance Study, 10 cases (5.2%) of major birth defects occurred as compared to the eight expected; however, this does not establish a causal relationship between metoclopramide and birth defects.
Proton pump inhibitors block potassium-hydrogen-ATPase and inhibit the secretion of gastric acid. Limited safety data in pregnancy are available for proton pump inhibitors, limiting their use to severe and refractory cases. All of the proton pump inhibitors are classified as pregnancy category B, except omeprazole which is category C. Initial omeprazole animal studies demonstrated embryonic and fetal toxicity at clinical doses. Subsequent prospective human pregnancy studies suggest that omeprazole is not a teratogen. A 2002 metaanalysis evaluated all major malformations among the proton pump inhibitors, which revealed a nonsignificant relative risk of 1.18 (95% CI: 0.72 to 1.94; p = 0.7) despite maternal use in the first trimester. Judicious use of proton pump inhibitors and avoidance during the first trimester minimize these potential risks.
Hypertension
Hypertension in pregnancy can lead to serious morbidity and mortality for the mother and fetus (97-101). Initial treatment options are lifestyle modifications such as restriction of activity, alcohol, tobacco products, and sodium intake. Close monitoring is essential to determine the response to interventions or the progression to severe hypertension (i.e., preeclampsia, eclampsia). If drug therapy is determined to be necessary, a few antihypertensive medications’ use in pregnancy have been documented.
Methyldopa is the preferred oral agent based on long-term follow-up studies and supporting safety data (97-101). Its pharmacologic action arises from the drug’s metabolism to alpha-methylnorepinephrine, which stimulates central inhibitory alpha-adrenergic receptors to lower arterial pressure; secondarily, methyldopa is believed to reduce plasma renin activity. Methyldopa is effective at controlling maternal blood pressure without adversely affecting uteroplacental or fetal blood flow. Additionally, a 7.5 year follow-up study found no adverse effects in children exposed to the drug in utero.
Labetalol has traditionally been reserved as a second-line therapy; however, prospective studies suggest similar efficacy and safety to methyldopa (97-101). Labetalol is a nonselective β-adrenergic blocker and a selective ^ι-adrenergic blocker; it reduces systemic vascular resistance and heart rate without decreasing peripheral, cerebral, coronary, or renal blood flow. Other β-adrenergic blockers (e.g., metoprolol) may be acceptable alternatives for moderate hypertension with close monitoring of fetal effects if patient response is inadequate to first-line therapies. Use of atenolol in the first and the second trimesters has been associated with fetal growth retardation and is not recommended. Likewise, angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin receptor blockers (ARBs) have been linked to fetal deaths and are contraindicated during pregnancy.
Historically, hydralazine has been the most commonly prescribed vasodilator for acute hypertension in pregnant women; however, a published metaanalysis suggests intravenous labetalol may be preferred over hydralazine for hypertensive emergencies (i.e., preeclampsia, eclampsia) (97-103). Results of the meta-analysis, including other anecdotal reports, reveal a higher incidence of adverse effects (e.g., placental abruption, increased caesarean sections, maternal oliguria, lower Apgar scores) with hydralazine. Therefore, practitioners are recommending labetolol as a first-line therapy and reserving hydralazine as a second-line therapy in acute, severe hypertension. Other agents for severe preeclampsia are available but fetal risk may be potentially greater. For example, esmolol is associated with fetal distress and bradycardia; thiazide diuretics may cause reduced placental perfusion.
Migraines
Migraines and headache do not appear to negatively impact pregnancy outcomes. Studies of migraine in pregnancy have found no increased incidence of preterm labor, low birth weights, or congenital anomalies (104,105). On the other hand, pregnancy predisposes women to several potentially life-threatening conditions such as preeclampsia, stroke, and cerebral venous thrombosis which can present with headache. Therefore, careful diagnosis and treatment of headache during pregnancy are crucial.
Non-pharmacologic therapies such as relaxation, biofeedback, massage, and stress management have been shown to be highly effective in patients with recurring headaches (104-106). If drug therapy is necessary, acetaminophen is often recommended first. The NSAIDs, ibuprofen and naproxen, have a category B rating for use in the first trimester of pregnancy. NSAID use in the third trimester, however, is known to cause premature closure of the ductus arteriosus in utero resulting in fetal pulmonary hypertension. Therefore, NSAIDs carry a category D rating in the third trimester (104). Ergotamine and dihydroergotamine are rated category X and are contraindicated in pregnancy. These ergot alkaloids are known to cause vasospasm and a prolonged and marked increase in uterine tone. This, in turn, causes an impaired placental blood flow leading to spontaneous abortion and fetal distress.
The serotonin 5-HT1 agonists (triptans) are very effective in the treatment of migraine headache in the general population and are considered relatively safe for the treatment of migraine in pregnancy (106,107). Current evidence from the sumatriptan and naratriptan registry in pregnancy suggests that sumatriptan does not carry a risk to either the fetus or the mother (107). Data regarding the other drugs in this class (zolmitriptan, naratriptan, almotrip- tan, eletriptan, frovatriptan, rizatriptan) are insufficient to draw the same conclusion.
Nausea/Vomiting
Nausea and vomiting of pregnancy (NVP) is the most common complication of pregnancy affecting up to 85% of patients. The range of this condition includes a mild course of morning sickness to the rare (0.3% to 2.3%) but severe form of nausea-hyperemesis gravidarum (HG). Duration of symptoms may resolve by the 3rd month of pregnancy or may last until delivery (108,109). The exact etiology of NVP is not known but may involve rapid changes of hormones in the mother. In all forms/extent of NVP, protection of the mother and the fetus from the deleterious effects of nutrition depletion secondary to inadequate intake or excessive loss of nutrients is the most important goal of therapy. One example is neural tube defects secondary to folate deficiency. Pharmacologic measures should also demonstrate safety to the fetus as many agents pass the placenta and could affect normal fetal development, including teratogenicity.
Therapy of NVP includes many non-pharmacologic lifestyle interventions including avoidance of noxious smells or foods, smaller portions of tolerable foods eaten at shorter intervals, small feeding before arising in the morning, and avoidance of spicy or fatty foods. Pharmacologic therapy should be considered if these measures are not effective, other diseases causing nausea and vomiting are ruled out, or symptoms are severe (109).
Only two pharmacologic therapies for NVP are considered safe during pregnancy, the antihistamine, doxylamine, and pyridoxine or vitamin B6. Prior to market withdrawal in 1983, these medications were available in the United States as a combination medication called Bendectin. Today, they are only available as single entities. These agents should be considered as first- line therapy as soon as other lifestyle interventions fail. Doses of doxylamine range from 12.5 to 25 mg twice daily or 12.5 mg twice a day with 25 mg at bedtime. Pyridoxine dose range from 10 to 25 mg three to four times daily (109,110). Higher doses have been studied, but they do not improve NVP and were associated with a higher hospitalization rates for rehydration (110). Preemptive antinausea medication has been reported to be more efficacious than therapy after symptoms of NVP (111). Other antihistamines such as dimenhydramine, diphenhydramine, and meclizine are considered as either replacement or additive for doxylamine. However, hydroxyzine, promethazine, and ranitidine should only be considered in more severe recalcitrant cases (109,112). Warnings of severe effects in children under 2 years of age were posted by the FDA in 2006 concerning the use of promethazine in infants (113). Coupled with the fact that promethazine achieves similar fetal and maternal levels, there is some concern for the continued use of promethazine for NVP or HG.
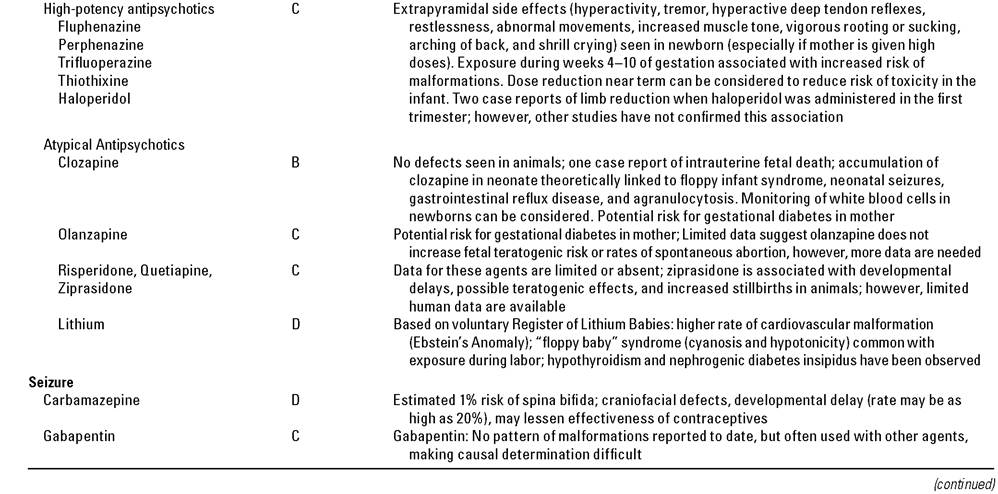
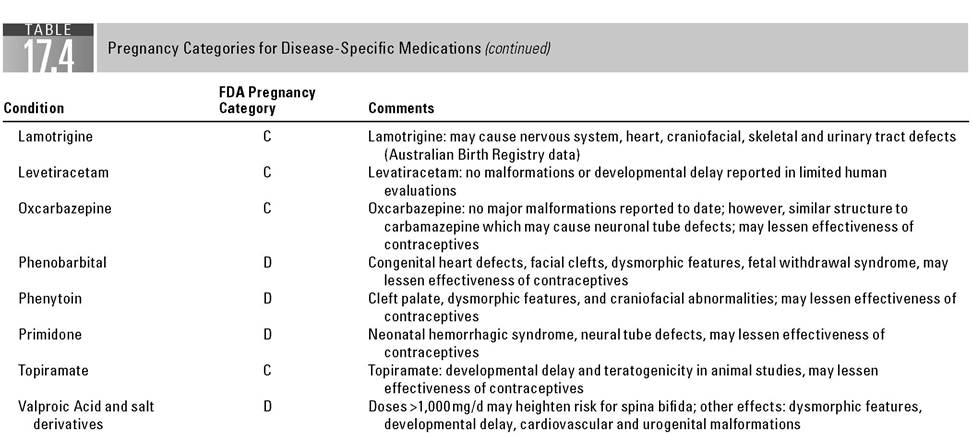
Recently, newer therapies have emerged (109,114). Both metoclopramide and ondansetron are available as oral, intravenous, or continuous subcutaneous infusions. Oral therapy with either of these medications may be added to the doxylamine/pyridoxine regimen. Metoclopramide is a dopamine and serotonin antagonist that increases upper GI tract motility and blocks receptors in the chemoreceptor zone (CTZ). The CNS effects are associated with extrapyramidal symptoms (EPS) which may limit its use. Ondansetron works through antagonism of the 5-HT3 receptor system, also blocking serotonin. Ondansetron works in the peripheral nerve receptors and also in the CTZ; however, there is no activity on peristalsis. Fatigue and headache are the most common side effects. More serious side effects, occur in lowest effective dose during pregnancy should be the first goal as polytherapy increases adverse effects on the fetus. The rate of congenital malformations in women not taking AEDs is approximately 2%. Congenital malformations increase to 4% to 9% in those taking first-generation AEDs (phenobarbital, phenytoin, valproic acid, carbamazepine, and ethosuximide). These include intrauterine growth retardation, congenital malformations, cognitive disabilities, microcephaly, and fetal demise (124,125). Valproic acid appears to be the most associated with decreased neonatal cognition and physical malformations (124-126). Newer AEDs (lamtrogine, topirimate, gabapentin, oxcarbazepine, and levetiracetam) have shown teratogenicity in animals, but human data are incomplete at this point (127). Several major countries operate registries to track and report the effects of AEDs on pregnancy, but most differ in clinical data recorded, making interpretation between them impractical (127,128). Another confounding issue is keeping AED levels consistent from pre-pregnancy until delivery. First-generation AED levels decrease 40% to 70% by the third trimester (129). Lamotrigene, levetiracetam, and oxcar- bazepine levels also decrease during pregnancy but information on other AEDs is lacking.
Seizures during labor are of particular concern for women with a generalized seizure disorder as this incidence increases sharply in women with partial disorders. During prolonged labor, oral AEDs may not be the preferred route as absorption can be erratic. Phenobarbital, phenytoin, fosphenytoin, valproic acid, and levetiracetam are alternatives available parenterally. Convulsive seizures occurring during labor should be treated aggressively with benzodiazepines. Measures to prevent hypoxia in the mother and the fetus and efforts to deliver the fetus should be instituted quickly (130).
High-dose folic acid supplementation (>4mg per day) has been recomm ended for prevention of neural tube defects in women on phenytoin, carbamazepine, phenobarbital, and primidone (124). Additionally, vitamin K supplementation should be initiated for women on certain carbamazepine, phenytoin, phenobarbital, and ethosuximide. Dose of oral vitamin K is 10mg daily beginning at 36 weeks’ gestation and continued until delivery (130).
References
1. Boothby LA, Doering PL. FDA labeling system for drugs in pregnancy. Ann Pharma- cother. 2001;35:1485-1489.
2. Doering PL, Boothby LA, Cheok M. Review of pregnancy labeling of prescription drugs: is the current system adequate to inform of risks? Am J Obstet Gynecol. 2002; 187:333-339.
3. Meadows M. Pregnancy and the drug dilemma. FDA Consumer May-June 2001. Available at: URL:http://www.fda.gov/fdac/features/2001/301_preg.html
4. Koren G, Pastuszak A, Ito S. Drugs in pregnancy. N Engl J Med. 1998;338(16): 1128-1137.
5. SchardeinJL. Chemically Induced Birth Defects. NewYork, NY: Marcel Dekker; 1985.
6. Moore KL. Causes of congenital malformations. In: The DevelopingHuma^ Clinically Oriented Embryology. 3rd Ed. Philadelphia, PA: WB Saunders; 1982.
7. Beely L. Adverse effects of drugs in the first trimester of pregnancy. Clin Obstet Gynecol. 1981;8:261.
8. Hayes DP. Teratogenesis: a review of the basic principles with a discussion of selected agents: Part I. Drug Intel Clin Pharm. 1981;15:544.
9. Henney JE. FDA/NICHD Conference. Clinical Pharmacology during pregnancy: addressing clinical needs through science. Available at: http://www.fda.gov/oc/ speeches/2000/nichdconference12-4.html (cited October 11, 2004).
10. Black RA, Hill A. Over-the counter medications in pregnancy. Am Fam Physician. 2003;67:2517-2524.
11. Information about pregnancy registries. US Food and Drug Administration. Available at: http://www.fda.gov/womens/registries/general.html (cited October 1, 2004).
12. Pacifici GM. Placental transfer of antibiotics administered to the mother: a review. IntJClinPharmacol Ther. 2006;44:57-63.
13. Nahum GG, Uhl K, Kennedy DL. Antibiotic use in pregnancy and lactation: what is and is not known about teratogenic and toxic risks. Obstet Gynecol. 2006;107: 1120-1138.
14. Briggs GG, Freeman RK, Yaffe SJ. Drugs in Pregnancy and Lactation: A Reference Guide to Fetal and Neonatal Risk. 8th Ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2008.
15. Heinonen O, Slone D, Shapiro S. Birth Defects and Drugs in Pregnancy. Littleton, MA: Publishing Sciences Group; 1977.
16. Jepsen P, Skriver MV, Floyd A, et al. A population-based study of maternal use of amoxicillin and pregnancy outcome in Denmark. Br J Clin Pharmacol. 2003;55: 216-221.
17. Berkovitch M, Diav-Citrin O, Greenberg R, et al. First-trimester exposure to amoxy- cillin/clavulanic acid: a prospective, controlled study. Br J Clin Pharmacol. 2004; 58:298-302.
18. Czeizel AE, Rockenbauer M, Sorensen HT, Olsen J. Augmentin treatment during pregnancy and the prevalence of congenital abnormalities: a population-based case-control teratologic study. Eur J Obstet Gynecol Reprod Biol. 2001;97:188-192.
19. Macejko AM, Schaeffer AJ. Asymptomatic bacteriuria and symptomatic urinary tract infections during pregnancy. Urol Clin North Am. 2007;34:35-42.
20. Einarson A, Shuhaiber S, Koren G. Effects of antibacterials on the unborn child: what is known and how should this influence prescribing. Paediatr Drugs. 2001;3: 803-816.
21. Czeizel AE, Rockenbauer M, Sorensen HT, Olsen J. Use of cephalosporins during pregnancy and in the presence of congenital abnormalities: a population-based, case-control study. Am J Obstet Gynecol. 2001;184:1289-1296.
22. Philipson A, Sabath LD, Charles D. Transplacental passage of erythromycin and clindamycin. N Engl JMed. 1973;288:1219-1221.
23. Schick B HM, Librizzi R, Donnenfeld A. Pregnancy outcome following exposure to clarithromycin. Abstracts of the Ninth International Conference of the Organization of Teratology Information Services, May 2-4, 1996, Salt Lake City, Utah. Reprod Toxicol. 1996;10:162. Abstract.
24. Einarson A, Phillips E, Mawji F, et al. A prospective controlled multicentre study of clarithromycin in pregnancy. Am J Perinatol. 1998;15:523-525.
25. Drinkard CR, Shatin D, Clouse J. Postmarketing surveillance of medications and pregnancy outcomes: clarithromycin and birth malformations. Pharmacoepidemiol Drug Saf. 2000;9:549-556.
26. Sarkar M, Woodland C, Koren G, Einarson AR. Pregnancy outcome following gestational exposure to azithromycin. BMC Pregnancy Childbirth. 2006;6:18 (DOI: 10.1186/1471-2393-6-18).
27. Shepard TH, Brent RL, Friedman JM, et al. Update on new developments in the study of human teratogens. Teratology. 2002;65:153-161.
28. Hernandez-Diaz S, Werler MM, Walker AM, Mitchell AA. Folic acid antagonists during pregnancy and the risk of birth defects. NEnglJMed. 2000;343:1608-1614.
29. Hernandez-Diaz S, Werler MM, Walker AM, Mitchell AA. Neural tube defects in relation to use of folic acid antagonists during pregnancy. Am J Epidemiol. 2001; 153:961-968.
30. Czeizel AE, Rockenbauer M, Sorensen HT, Olsen J. The teratogenic risk of trimethop- rim-sulfonamides: a population based case-control study. Reprod Toxicol. 2001;15: 637-646.
31. Niebyl JR. Antibiotics and other anti-infective agents in pregnancy and lactation. Am J Perinatol. 2003;20:405-414.
32. Caro-Paton T, Carvajal A, Martin de Diego I, et al. Is metronidazole teratogenic? A meta-analysis. Br J Clin Pharmacol. 1997;44:179-182.
33. Czeizel AE, Rockenbauer M. A population based case-control teratologic study of oral metronidazole treatment during pregnancy. Br J Obstet Gynecol. 1998;105: 322-327.
34. Burtin P, Taddio A, Ariburnu O, Einarson TR, Koren G. Safety of metronidazole in pregnancy: a meta-analysis. Am J Obstet Gynecol. 1995;172(2, pt 1):525-529.
35. Piper JM, Mitchel EF, Ray WA. Prenatal use of metronidazole and birth defects: no association. Obstet Gynecol. 1993;82:348-352.
36. Workowski KA, Berman SM. Sexually transmitted diseases treatment guidelines, 2006. MMWR Recomm Rep. 2006;55(RR-11):1-94.
37. Czeizel AE, Rockenbauer M, Olsen J, Sorensen HT. A teratological study of aminoglycoside antibiotic treatment during pregnancy. ScandJ Infect Dis. 2000;32:309-313.
38. Berkovitch M, Pastuszak A, Gazarian M, Lewis M, Koren G. Safety of the new quinolones in pregnancy. Obstet Gynecol. 1994;84:535-538.
39. Loebstein R, Addis A, Ho E, et al. Pregnancy outcome following gestational exposure to fluoroquinolones: a multicenter prospective controlled study. Antimicrob Agents Chemother. 1998;42:1336-1339.
40. Schaefer C, Amoura-Elefant E, Vial T, et al. Pregnancy outcome after prenatal quinolone exposure. Evaluation of a case registry of the European Network of Teratology Information Services (ENTIS). Eur J Obstet Gynecol Repod Biol. 1996;69: 83-89.
41. Bourget P, Fernandez H, Delouis C, Ribou F. Transplacental passage of vancomycin during the second trimester of pregnancy. Obstet Gynecol. 1991;78(5, pt 2):908-911.
42. Pfizer Pharmaceuticals, Inc. Linezolid use during pregnancy and breastfeeding (written communication). October 2004.
43. Shea K, Hilburger E, Baroco A, Oldfield E. Successful treatment of vancomycin- resistant Enterococcus faecium pyelonephritis with daptomycin during pregnancy. Ann Pharmacother. 2008;42:722-725.
44. Cunha BA, Hamid N, Kessler H, Parchuri S. Daptomycin cure after cefazolin treatment failure of Methicillin-sensitive Staphylococcus aureus (MSSA) tricuspid valve acute bacterial endocarditis from a peripherally inserted central catheter (PICC) line. Heart Lung. 2005;34:442-447.
45. Rebordosa C, Kogevinas M, Horvath-Puho E, et al. Acetaminophen use during pregnancy: effects on risk for congenital abnormalities. Am J Obstet Gynecol. 2008;198: 178. e1-7.
46. Czeizel AE, Dudas I, Puho E. Short-term paracetamol therapy during pregnancy and a lower rate of preterm birth. Paediatr Perinat Epidemiol. 2005;19(2):106-111.
47. Ostensen ME, Skomsvoll JF. Anti-inflammatory pharmacotherapy during pregnancy. Expert OpinPharmacother. 2004;5:571-580.
48. Kozer E, Nikfar S, Costei A, et al. Aspirin consumption during the first trimester of pregnancy and congenital anomalies: a meta-analysis. Am J Obstet Gynecol. 2002; 187:1623-1630.
49. Kozer E, Costei AM, Boskovic R, et al. Effects of aspirin consumption during pregnancy on pregnancy outcomes: meta-analysis. Birth Defects Res B Dev Reprod Toxicol. 2003;68:70-84.
50. Ostensen M, Ramsey-Goldman R. Treatment of inflammatory rheumatic disorders in pregnancy: what are the safest treatment options? Drug Saf. 1998;19:389-410.
51. Chambers CD, Tutuncu ZN, Johnson D, Jones KL. Human pregnancy safety for agents used to treat rheumatoid arthritis: adequacy of available information and strategies for developing post-marketing data. ArthritisRes Ther. 2006;8:215 (DOI: 10.1186∕ar977).
52. Tassinari MS, Cook JC, Hurtt ME. NSAIDs and developmental toxicity. Birth Defects Res B Dev Reprod Toxicol. 2003;68:3-4.
53. Nielsen GL, Sorensen HT, Larsen H, Pedersen L. Risk of adverse birth outcome and miscarriage in pregnant users of non-steroidal anti-inflammatory drugs: population based observational study and case-control study. Br Med J. 2001;322:266-270.
54. Loe SM, Sanchez-Ramos L, Kaunitz AM. Assessing the neonatal safety of indomethacin tocolysis: a systematic review with meta-analysis. Obstet Gynecol. 2005;106: 173-179.
55. Koren G, Florescu A, Costei AM, Boskovic R, Moretti ME. Nonsteroidal antiinflammatory drugs during third trimester and the risk of premature closure of the ductus arteriosus: a meta-analysis. Ann Pharmacother. 2006;40:824-829.
56. Benini D, Fanos V, Cuzzolin L, Tato L. In utero exposure to nonsteroidal antiinflammatory drugs: neonatal renal failure. Pediatr Nephrol. 2004;19:232-234.
57. Rathmell JP, Viscomi CM, Ashburn MA. Management of nonobstetric pain during pregnancy and lactation. Anesth Analg. 1997;85:1074-1087.
58. Dombrowski MP, Schatz M. ACOG practice bulletin: clinical management guidelines for obstetrician-gynecologists number 90, February 2008: asthma in pregnancy. Obstet Gynecol. 2008;111(2, pt 1):457-464.
59. Gilbert C, Mazzotta P, Loebstein R, Koren G. Fetal safety of drugs used in the treatment of allergic rhinitis: a critical review. Drug Saf. 2005;28:707-719.
60. Gluck JC, Gluck PA. Asthma controller therapy during pregnancy. Am J Obstet Gynecol. 2005;192:369-380.
61. Liccardi G, Cazzola M, Canonica GW, et al. General strategy for the management of bronchial asthma in pregnancy. Respir Med. 2003;97:778-789.
62. Chambers C. Safety of asthma and allergy medications in pregnancy. Immunol Allergy Clin North Am. 2006;26:13-28.
63. James A. Venous thromboembolism in pregnancy. Arterioscler Thromb Vasc Biol. 2009:29:326-331.
64. Weitz J. Prevention and treatment of venous thromboembolism during pregnancy, Proceedings from the Vascular Interventional Advances 06 meeting, Las Vegas, NV, USA September 26-29, 2006.
65. Bates S, Greer I, Pabinger I, Sofaer S, Hirsh J. Venous thromboembolism, thrombophilia, antithrombotic therapy, and pregnancy. Chest. 2008;133:844S-886S.
66. Hirsh J, Bauer K, Donati M, et al. Parenteral anticoagulants. Chest. 2008:133: 141S-159S.
67. Greer I. Thromboembolism and anticoagulant therapy in pregnancy. Gend Med. 2005;2(Suppl. A):S10-S17.
68. Patel J, Hunt B. Where do we go now with low molecular weight heparin use in obstetric care? JThrombHaemost. 2008;6:1461-1467.
69. Bates S. Management of pregnant women with thrombophilia or a history of venous thromboembolism. Hematology. 2007;143-150.
70. Greer I, Hunt B. Low molecular weight heparin in pregnancy: current issues. Br JHaematol. 2004;128:593-601.
71. Gavin NI, Gaynes BN, Lohr KN, et al. Perinatal depression: a systematic review of prevalence and incidence. Obstet Gynecol. 2005;106:1071-1083.
72. Way CM. Safety of newer antidepressants in pregnancy. Pharmacotherapy. 2007; 27(4):546-552.
73. Belik J. Fetal and neonatal effects of maternal drug treatment for depression. Semin Perinatal. 2008;32:350-354.
74. Pearlstein T. Perinatal depression: treatment options and dilemmas. J Psychiatry Neurosci. 2008;33(4):302-318.
75. Davis RL, Rubanowice D, McPhillips H, et al. Risks of congenital malformations and perinatal events among infants exposed to antidepressant medications during pregnancy. PharmacoepidemiolDrug Saf. 2007;16:1086-1094.
76. Andrade SE, Raebel MA, Brown J, et al. Use of antidepressant medications during pregnancy: a multi-site study. AmJObstet Gynecol. 2008;198:194.e1-5.
77. Ter Horst PG, Jansman FG, Van Lingen RA, et al. Pharmacological aspects of neonatal antidepressant withdrawal. Obstet Gynecol Survey. 2008;63(4):267-279.
78. Food and Drug Administration. FDA public health advisory: paroxetine [electronic citation]. Available at: http://www.fda.gov/cder/drug/advisory/paroxetine200512. htm (accessed January 2009).
79. Einarson A, Pistelli A, DeSantis M, et al. Evaluation of the risk of congenital cardiovascular defects associated with use of paroxetine during pregnancy [published corrections appear in Am J Psychiatry. 2008;165(6):777 and 2008; 165(6):1208]. AmJPsychiatry. 2008;165(6):749-752.
80. Wichman CL, Moore KM, Lang TR, et al. Congenital heart disease associated with selective serotonin reuptake inhibitor use during pregnancy. Mayo Clin Proc. 2009; 84(1):23-27.
81. Food and Drug Administration. FDA public health advisory:treatment challenges of depression in pregnancy and the possibility of persistent pulmonary hypertension in newborns [electronic citation]. Available at: http://www.fda.gov/cder/drug/ advisory/SSRI_PPHN200607.htm (accessed February 2009).
82. Chambers CD, Hernandez-Diaz S, Van Marter LJ, et al. Selective serotonin- reuptake inhibitors and risk of persistent pulmonary hypertension of the newborn. NEnglJMed. 2006;354(6):579-587.
83. Andrade SE, McPhillips H, Loren D, et al. Antidepressant use and risk of persistent pulmonary hypertension of the newborn. Pharmacoepidemiol Drug Saf. 2009; 18:246-252.
84. American College of Obstetricians and Gynecologists (ACOG) Practice Bulletin Number 30. Gestational diabetes. Obstet Gynecol. 2001;98:525-538.
85. Gabbe SG, Graves CR. Management of diabetes mellitus complicating pregnancy. Obstet Gynecol. 2003;102(4):857-868.
86. Homko CJ, Reece EA. Insulins and oral hypoglycemic agents in pregnancy.JMatern Fetal Neonatal Med. 2006;19(11):679-686.
87. Nicholson W, Bolen S, Witkop CT, et al. Benefits and risks of oral diabetes agents compared with insulin in women with gestational diabetes. Obstet Gynecol. 2009; 113(1):193-205.
88. Jovanovic L, Pettitt DJ. Treatment with insulin and its analogs in pregnancies complicated by diabetes. Diabetes Care. 2007;30:S220-S224.
89. Merlob P, Levitt O, Stahl B. Oral antihyperglycemic agents during pregnancy and lactation: a review. Pediatr Drugs. 2002;4(11):755-760.
90. Langer O, Conway DL, Berkus MD, et al. A comparison of glyburide and insulin in women with gestational diabetes mellitus. NEnglJMed. 2000;343:1134-1138.
91. Langer O, Yogev Y, Xenakis EM, et al. Insulin and glyburide therapy: dosage, severity level of gestational diabetes, and pregnancy outcome. Am J Obstet Gynecol. 2005;192:134-139.
92. Hellmuth E, Damm P, Mlsted-Pedersen L. Oral hypoglycemic agents in 118 diabetic pregnancies. Diabet Med. 2000;17:507-511.
93. Rowan JA, Hague WM, Gao W, et al. Metformin versus insulin for the treatment of gestational diabetes. NEnglJMed. 2008;358(19):2003-2015.
94. Richter JE. Review article: the management of heartburn in pregnancy. Aliment Pharmacol Ther. 2005;22:749-757.
95. Broussard CN, Richter JE. Treating gastro-esophageal reflux disease during pregnancy and lactation. Drug Safety. 1998;19(4):325-337.
96. Diav-Citrin O, Arnon J, Shechtman S, et al. The safety of proton pump inhibitors in pregnancy: a multicenter prospective controlled study. Aliment Pharmacol Ther. 2005;21:269-275.
97. Sibai BM. Chronic hypertension in pregnancy. Am J Obstet Gynecol. 2002;100(2): 369-377.
98. Montan S. Drugs used in hypertensive diseases in pregnancy. Curr Opin Obstet Gynecol. 2004;16:111-115.
99. Peters RM, Flack JM. Hypertensive disorders of pregnancy. JOGNN. 2004;33: 209-220.
100. National Institutes of Health (Joint National Committee on Prevention, Detection, and Treatment of High Blood Pressure). The seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. (NIH Publication No. 04-5230). Washington, DC; 2004.
101. National Institutes of Health. Working group report on high blood pressure in pregnancy. (NIH Publication No. 00-3029). Washington, DC; 2000.
102. Magee LA, Cham C, Waterman EJ, Ohlsson A, Dadelszen PV Hydralazine for treatment of severe hypertension in pregnancy: meta analysis. Br Med J. 2003;327: 955-965.
103. McCoy S, Baldwin K. Pharmacotherapeutic options for the treatment of preeclampsia. Am J Health-Syst Pharm. 2009;66:337-344.
104. Menon R, Bushnell C. Headache and pregnancy. Neurologist. 2008;14:108-119.
105. Soldin OP, Dahlin J, O'Mara DM. Triptans in pregnancy. Ther Drug Monit. 2008; 30(1):5-9.
106. Evans EW, Lorber KC. Use of 5-HT1 agonists in pregnancy. AnnPharmacother. 2008; 42:543-549.
107. Goadsby PJ, GoldbergJ, Silberstein SD. Migraine in pregnancy. Br Med J. 2008; 336:1502-1504.
108. Tan P, Jacob R, Quek K, Omar S. Pregnancy outcome in hyperemesis gravidarum and the effect of laboratory clinical indicators of hyperemesis severity. J Obstet Gynaecol Res. 2006;33(4):457-464.
109. Sheehan P. Hyperemesis gravidarum. AustFam Physician. 2007;36(9):699-701.
110. Atanackovic G, Navioz Y, Moretti M, Koren G. The safety of higher than standard dose of doxylamine-pyridoxine for nausea and vomiting of pregnancy. J Clin Pharmacol. 2001;51:842-845.
111. Koren G, Maltepe C. Pre-emptive therapy for severe nausea and vomiting of pregnancy and hyperemesis gravidarum. J Obstet Gynaecol. 2004;24(5):530-533.
112. AGOG Issues Guidance on Treatment of Morning Sickness During Pregnancy, The American College of Obstetricians and Gynecologists news release. March 29, 2004.
113. Anon FDA. Alert for Promethazine HCL, U.S. Food and Drug Administration Bulletin, April 25, 2006.
114. Reichmann J, Kirkbride M. Nausea and vomiting of pregnancy-cost effective pharmacologic treatments. Manag Care. 2008;17:41-45.
115. Spiegel J, Kang V, Kunze L, Hess P. Ondansetron-induced extrapyramidal symptoms during cesarean section. IntJObstetAnesth. 2005;6:368-369.
116. Pasricha Pankaj J. Treatment of disorders of bowel motility and water flux and Antiemetics agents used in biliary and pancreatic disease. In: Brunton LL, Lazo JS, Parker KL. Goodman & Gilman’s the Pharmacological Basis of Therapeutics. 11th Ed. Available at: http://www.accessmedicine.com/content.aspx?aID=946551
117. Giles JJ, Bannigan JG. Teratogenic and developmental effects of lithium. Curr Pharm Des. 2006;12:1531-1541.
118. Frieder A, Dunlop AL, Culpepper L, Bernstein P. The clinical content of preconception care: women with psychiatric conditions. Am J Obstet Gynecol. 2008;199 (6 Suppl. 2):S328-S332.
119. Yonkers KA, Wisner KL, Stowe Z, et al. Management of bipolar disorder during pregnancy and the postpartum period. Am J Psychiatry. 2004;161(4):608-620.
120. Use of psychiatric medications during pregnancy and lactation. ACOG Practice Bulletin No. 92. American College of Obstetricians and Gynecologists. Obstet Gynecol. 2008;111:1001-1020.
121. Dodd S, Berk M. The safety of medications for the treatment of bipolar disorder during pregnancy and the puerperium. CurrDrug Saf. 2006;1:25-33.
122. Reis M, Kallen B. Maternal use of antipsychotics in early pregnancy and delivery outcome. J Clin Psychopharmacol. 2008;28(3):279-288.
123. Battino D, Tomson T. Management of epilepsy during pregnancy. Drugs. 2007; 67(18):2727-2746.
124. Pennell P. Antiepileptic drugs during pregnancy: what is known and which AEDs seem to be safest? Epilepsia. 2008;49(Suppl. 9):43- 55.
125. Uziel D, Rozental R. Neurologic birth defects after prenatal exposure to antiepileptic drugs. Epilepsia. 2008;49(Suppl. 9):35-42.
126. Harden C, Sethi N. Epliptic disorders in pregnancy: an overview. Curr Opin Obstet Gynecol. 2008;20:557-562.
127. Karceski S. Epilepsy and pregnancy, are seizure medications safe? Neurology. 2008;71:e32-33.
128. Meador K, Pennell P, Harden C, et al. Pregnancy registries in epilepsy, a consensus statement on health outcomes. Neurology. 2008;71:1109-1117.
129. Yerby M, Kaplan P, Tran T. Risks and management of pregnancy in women with epilepsy. Clev Clin JMed. 2004;71(Suppl. 2):S25-S37.
130. Pennell P. Pregnancy in women who have epilepsy. Neurol Clin. 2004;22:799-820.