Role of Imaging Modalities in Obstetric Emergencies
Lama L. Tolaymat and Gwyn Grabner
Imaging has assumed a key role in the management of obstetric patients. Depending upon the patient population and clinical problem, a variety of imaging modalities are available for use, some more appropriate than others.
Some women are exposed to x-rays before the diagnosis of pregnancy is known. Occasionally, x-ray procedures may be indicated during the pregnancy. To understand which modality to use for a specific concern, all imaging modalities must be reviewed with emphasis on the method of generating an image, common uses in pregnancy, and the associated risk with use. Table 16.1 summarizes the different modalities and the associated fetal exposure of radiation.RADIATION EXPOSURE IN PREGNANCY
There has been a growing concern about radiation exposure in the case of pregnant women who undergo radiological examinations. Lack of knowledge may result in unnecessary patient anxiety. Teratogenic effects have developed in animals exposed to large doses of radiation (up to 200 rad). The main effects of radiation on the human embryo and the fetus are prenatal death, growth restriction, congenital malformations, and mental retardation. Based on data from the atomic bomb survivors, it appears that the risk of central nervous system effects is greatest with exposures at 8 to 15 weeks of gestation (1,2). Prenatal doses from properly performed diagnostic procedures present no significant increased risk of prenatal death, malformation, or impairment of mental development over the background incidence of these entities. Rare consequences of prenatal radiation exposure include a slight increase in the incidence of childhood leukemia and, possibly, a very small change in the frequency of genetic mutations. Such exposure is not an indication of pregnancy termination. In 1977, the National Council on Radiation Protection and Measurement issued a report stating that “The risk [of abnormality] is considered to be negligible at 50 mGy [=5 rad] or less when compared to other risks of pregnancy, and the risk of malformation is significantly increased above control levels only at doses above 150mGy [=15 rad].
Therefore, exposure of the fetus to radiation arising from diagnostic procedures would very rarely be the cause for terminating a pregnancy” (3). The accepted safe cumulative dose of ionizing radiation during pregnancy is 5 rad (0.05 Gy). The American College of Radiology established that “The interruption of pregnancy is rarely justified because of radiation risk to the embryo or fetus from a radiologic examination” (4). The most sensitive time period for central nervous system teratogenesis is between 10 and 17 weeks of gestation. Nonurgent radiologic testing should be avoided during this time.Risk Related to Gestational Age (5)
1. Fetal exposure prior to 2 weeks post-conception to 10 rad may lead to the death of the embryo.
2. Fetal exposure at 2 to 7 weeks post-conception to 5 to 50 rad leads to an increase in the risk of major malformations and growth restriction. An exposure to >50 rad leads to a substantial risk of malformations, growth restriction, and miscarriages.

Diagnostic Imaging Procedures and the Estimated Average Associated Fetal Exposure
| Study | Approximate Fetal Exposure |
| Dental x-ray | 0.006 mrad |
| Chest AP and lateral | 0.02-0.07 mrad |
| Hip x-ray | 200 mrad |
| IVP | ≥1 rad |
| Mammogram | 7-20 mrad |
| Head CT | 16.1), can be seen by endovaginal ultrasound. Normal gestational sac can be demonstrated when the hCG level is ≥1,800 mIU/ mL (11). The second sign of pregnancy, the yolk sac, can be seen by endovaginal ultrasound at about 5.5 weeks. Its presence confirms that an intrauterine pregnancy is present (Fig. 16.2). The number of yolk sacs equals the number of amnions; accordingly, in twin gestations, the number of yolk sacs can be counted to determine if it is monoamniotic or diamniotic. The fetal pole is seen as a focal thickening on the yolk sac, hence the “diamond ring” sign. A distinct embryo will be identified adjacent to the yolk sac at 6 to 6.5 weeks with cardiac activity when the BhCG level is approximately 10,800 mIU/mL (11). A fetal pole of 5 mm is the discriminatory value for the presence of heart beat, although recent data
FIGURE 16.1 Endovaginal image of an early intrauterine pregnancy demonstrating gestational sac.
FIGURE 16.2 Endovaginal image of an intrauterine gestational sac with a yolk sac visualized within it. suggest that the cutoff should be lowered to 3mm (12). Correlation of serum levels and endovaginal ultrasound findings are key when patients are being evaluated for pain or bleeding (13). It is important to keep in mind that these parameters depend largely on the operator’s experience and the instrumentation used. VAGINAL bleeding in pregnancy Vaginal bleeding occurs in about 20% to 30% of all confirmed pregnancies in the first 20 weeks; about 50% of these end in spontaneous abortions (14). Disorders that commonly cause abnormal bleeding include ectopic (ruptured/unruptured) pregnancy, spontaneous abortion (to include complete, missed, inevitable, incomplete, blighted ovum, and threatened abortion), gestational trophoblastic disease, placenta previa/vasa previa, and placental abruption. Readers may also wish to consult Chapter 8. First Trimester Bleeding Implantation bleeding: This term refers to a transient spotting associated with the normal implantation of the embryo into the uterine wall. Bleeding is usually minimal and is no cause for concern. Endovaginal ultrasound demonstrates a hypoechoic cleft in the decidua (endometrium thickened) near the sac.Threatenedmiscarriage/abortion: This diagnosis refers to early pregnancies complicated by bleeding and/or cramping, while with endovaginal ultrasound, the fetal pole is visualized and fetal cardiac activity is present (Fig. 16.3). Contributing factors may include abnormal karyotype, infection, dehydration,
FIGURE 16.3 Endovaginal image of a first trimester fetus. Measurement of the crown-rump length (CRL; calipers).
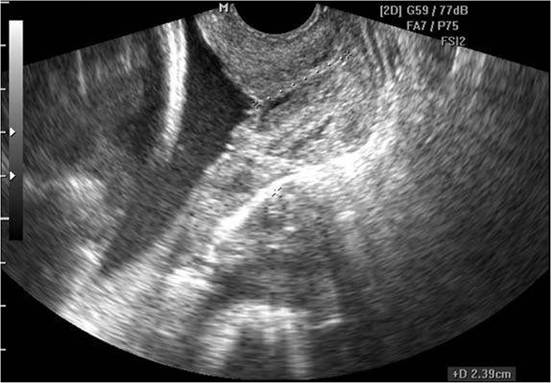
FIGURE 16.4 Endovaginal image of a retroplacental hematoma (the hypoechoic region measured). physical trauma, or use of drugs or medications. In many cases of threatened miscarriage, no contributing factors are identified. Occasionally, a retroplacental hematoma is seen (Fig. 16.4), and 25% of these pregnancies will miscarry, while without a hematoma, the risk of loss is 7% (15). Spontaneous (Complete)Abortion', This term refers to heavy bleeding and cramping (in women with previously documented intrauterine pregnancy), and endovaginal ultrasound shows an empty endometrial cavity. Incomplete Abortion: Partial expulsion of products of conception from the uterus with some retained products, usually clots and placental tissue. Sometimes the cervix appears to be open when inspected by speculum examination. Ultrasound may reveal the presence of tissue within the endometrial cav it y. Blighted ovum (anembryonic): This terminology refers to pregnancies in the embryo that have failed to develop appropriately. The discriminatory criterion for anembryonic pregnancy by endovaginal ultrasound is a mean gestational sac diameter (MGSD) of >10mm without a yolk sac or a MGSD >18mm without a fetal pole. By transabdominal ultrasound, MGSD cutoffs of 20 mm without a yolk sac and 25 mm without embryo fetal pole are used (13). The accuracy of these parameters depends largely on the operator’s experience and the instrumentation used.Ectopic pregnancy: An ectopic pregnancy occurs when a fertilized ovum implants at a site other than the endometrial lining of the uterus. Diagnosis is often made by a pelvic examination and a combination of serum BhCG and endovaginal ultrasound. The sonographic identification of an intrauterine gestational sac with yolk sac essentially excludes an ectopic pregnancy. An intrauterine pregnancy should always be visualized at a BhCG level of 2,000 IU/L by endovaginal ultrasound and at a 6,500 IU/L by transabdominal ultrasound. An adnexal mass, in a patient with a BhCG level the cervical length (CL) is obtained by measuring the endocervical canal from the internal cervical os to the external os (Fig. 16.8). Endovaginal approach is a more accurate method since it does not have the distortion associated with the transabdominal approach. Because of the dynamic nature of the cervical canal and lower uterine segment throughout pregnancy, the normal length of a competent cervix falls within a wide range (0.5 to 5 cm) (17). Consequently, the sonographic assessment of the cervix requires attention to the temporal changes of the CL during every examination. Furthermore, the Valsalva maneuver or manual compression of the uterine fundus may corroborate the sonographic diagnosis of cervical incompetence. The sonographic determination of the residual closed length of the cervix may be used as a prognostic indicator of the risk of preterm labor progressing into preterm delivery. A cervical cerclage is a surgical procedure performed before 24 weeks that presents an option for women with cervical incompetence (18). Placenta previa: This term refers to implantation of the placenta over or near the internal cervical os. It can be termed complete, partial, marginal or low- lying depending on its location relative to the internal os. Bleeding is usually bright red and painless. Since a pelvic digital examination is contraindicated in placenta previa, endovaginal ultrasound has been established as a safe assessment tool (19). Endovaginal ultrasound gives clear views of the cervical os and
FIGURE 16.7 Endovaginal ultrasound image of an incompetent cervix. Funneling indicates that the internal cervical os is dilated, allowing the amniotic sac to enter into the endocervical canal. Residual CL is measured with calipers.
FIGURE 16.8 Sagittal view of the maternal cervix with endovaginal ultrasound showing a normal endocervical canal. CL is measured from the internal os to the external os (calipers). lower uterine segment, even at full term; therefore, it is used to improve the accuracy of diagnosis of placenta previa (Fig. 16.9). Vasa Previa: This term refers to an obstetric complication when fetal vessels traverse the fetal membranes over the internal cervical os. These vessels may be from either a velamentous insertion of the umbilical cord or may be joining an accessory placental lobe (succenturiate) to the main lobe of the placenta. If these fetal vessels rupture, the bleeding is from the fetoplacental circulation, and fetal exsanguination will rapidly occur, leading to fetal death. Vasa previa must be ruled out in all cases of bilobed, succenturiate, and low-lying placentas; pregnancies resulting from in vitro fertilization; and multiple pregnancies. Endovaginal ultrasound in combination with color Doppler is the most effective tool in antenatal diagnosis of vasa previa (20). Placental abruption: Abruption describes the condition which occurs when the placenta separates from the wall of the uterus prematurely and blood collects in that space between the two. On ultrasound examination, one may see a fluid collection of varying echogenicity based on the age of the hemorrhage with or without a connection to the placenta. Uterine Rupture: Uterine rupture may be associated with acute, potentially catastrophic complication which may result in maternal and perinatal mortality. It is defined as a full-thickness separation of the uterine wall and the overlying serosa. Uterine rupture is associated with clinically significant uterine bleeding; fetal distress; expulsion or protrusion of the fetus, placenta, or both into the abdominal cavity; and the need for prompt surgical intervention for delivery, uterine repair, or hysterectomy. Prior cesarean delivery is the most common risk factor. With complete wall disruption, protrusion of the amniotic sac beyond the uterus may be seen, as well as intraperitoneal or extraperitoneal hemorrhage.
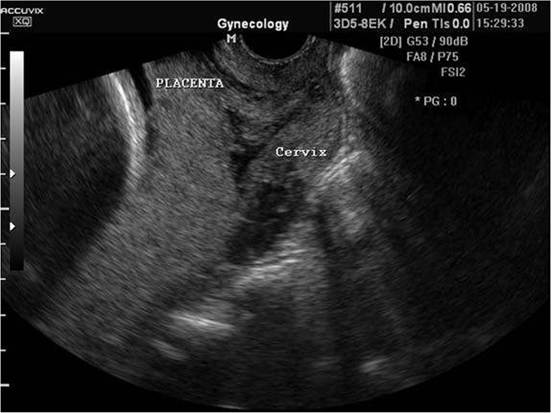
FIGURE 16.9 Endovaginal image of the uterine cervix demonstrating a complete placenta previa (the placenta completely covers the internal os). TRAUMA IN PREGNANCY Trauma and accidental injuries complicate 6% to 7% of all pregnancies (21) and are usually due to motor vehicle accidents, domestic abuse or assaults, and falls. Once fetal heart tones are confirmed, two patients exist and both require assessment and treatment. The anatomic and the physiologic changes of pregnancy make the trauma assessment more difficult. Readers may also wish to consult Chapter 4. The cardinal principle in the management of trauma in pregnancy is that there can be no fetal survival without maternal survival, with the rare exception of the gravely injured mother late in pregnancy where urgent cesarean delivery may allow for fetal survival. With pregnancy, there is an increased risk of internal hemorrhage, and identification of bleeding is more difficult. Common adverse consequences to abdominal trauma in pregnancy include uterine contractions, preterm labor or delivery, and placental abruption. In many cases, external fetal monitoring and ultrasound may be adequate for assessment of the placenta, uterus, and fetal well-being. Obstetric and emergency department clinicians should recognize that even minor trauma in the pregnant woman can cause fetal demise (22). From an imaging perspective, ultrasound is an excellent tool for initial evaluation of the trauma pregnant patient, but CT is the preferred modality when clinical or ultrasound findings suggest visceral injuries unaccompanied by intraperitoneal hemorrhage or injuries of the bones, chest, mediastinum, aorta, spine, retroperitoneum, bladder, and bowel. MRI is not a practical option for rapid evaluation of all these body parts in an unstable patient after trauma. Placental abruption typically appears on CT as a single avascular area of varying size that extends from the placental base to the placental surface. High attenuation in the nonplacental portion of the uterus indicates contusion, tear, or partial uterine disruption. Loss of amniotic fluid into the maternal peritoneum or free fetal parts in the maternal abdomen may indicate uterine rupture. But it may be difficult to determine if free intraperitoneal fluid is amniotic fluid or hemorrhage from a maternal visceral injury. In general, ultrasound may be sufficient for the initial imaging evaluation of a pregnant patient who has sustained trauma, but CT should be performed if a serious injury is suspected. References 1. Hall EJ. Scientific view of low-level radiation risks. Radiographics. 1991;11:509-518. 2. Schull WJ. The children of atomic bomb survivors: a synopsis. J Radiol Prot. 2003; 23:369-384. 3. National Council on Radiation Protection and Measurements. Medical radiation exposure of pregnant and potentially pregnant women. NCRP report no. 54. Bethesda, MD: National Council on Radiation Protection and Measurement-; 1977. 4. American College of Radiology. A CoR 04-05 bylaws. Reston, VA: American College of Radiology, 2005. 5. Center for Disease Control Radiation Emergencies. Prenatal radiation exposure: a fact sheet for physicians. Available at: http://www.bt.cdc.gov/radiation/prenatal- physician.asp accessed March12, 2009. 6. Ginsberg JS, HirshJ, Rainbow AJ, Coates G. Risks to the fetus of radiologic procedures used in the diagnosis of maternal venous thromboembolic disease. Thromb Haemost. 1989;61:189-196. 7. International Society for Ultrasound in Obstetrics and Gynecology. Safety statement, 2000 (confirmed 2002). Ultrasound Obstet Gynecol. 2000;16:594-596. 8. Malinger G, Ben-Sira L, Lev D, et al. Fetal brain imaging: a comparison between magnetic resonance imaging and dedicated neurosonography. Ultrasound Obstet Gynecol. 2004;23(4):333-340. 9. Bertrand G, Le Ray C, Simard-Emond L, Dubois J, Leduc L. Imaging in the management of abdominal pregnancy: a case report and review of the literature. J Obstet Gynaecol Can. 2009;31(1):57-62. 10. American College of Obstetricians and Gynecologists. Guidelines for diagnostic imaging during the pregnancy. ACOG Committee Opinion. Number 299, 2004. 11. Nyberg DA, Mack LA, Laing FC, et al. Early pregnancy complications: Endovaginal sonographic findings correlated with human chorionic gonadotropin levels. Radiology. 1988;167:619-622. 12. Abaid LN, As-Sanie S, Wolfe HM. Relationship between crown-rump length and early detection of cardiac activity. JReprodMed. 2007;52:375-378. 13. Nyberg DA, Laing FC, Filly RA. Threatened abortion: sonographic distinction of normal and abnormal gestation sacs. Radiology. 1986;158:393-396. 14. Everett C. Incidence and outcome of bleeding before the 20th week of pregnancy: a prospective study from general practice. Br MedJ. 1997;315:32-34. 15. Poulose T, Richardson R, Ewings P, Fox R. Probability of early pregnancy loss in women with vaginal bleeding and a singleton live fetus at ultrasound scan. J Obstet Gynecol. 2006;26(8):782-784. 16. Levine D. Ectopic pregnancy. Radiology. 2007;245(2):385-397. 17. Salomon LJ, Diaz-Garcia C, Bernard JP, Ville Y. Reference range for cervical length throughout pregnancy: non-parametric LMS-based model applied to a large sample. Ultrasound Obstet Gynecol. 2009; published on line by Wiley Interscience ahead of press. 18. Cunningham FG, Gant NF, Leveno KJ, Gilstrap LC III, Hauth JC, Wenstrom KD. General considerations and maternal evaluation. In: Williams obstetrics. 21st Ed. New York, NY: McGraw-Hill; 2001:1143-1158. 19. Timor-Tritsch IE, Yunis RA. Confirming the safety of transvaginal sonography in patients suspected of placenta previa. Obstet Gynecol. 1993;81(5):742-744. 20. Oyelese KO, Turner M, Lees C, Campbell S. Vasa previa: an avoidable obstetric tragedy. Obstet Gynecol Survey. 1999;54(2):138-145. 21. American College of Obstetricians and Gynecologists. Obstetric aspects of trauma management. ACOG Educational Bulletin. Number 251, 1998. 22. Weiss HB, Sauber-Schatz EK, Cook LJ. The epidemiology of pregnancy-associated emergency department injury visits and their impact on birth outcomes. Accid Anal Prev. 2008;40(3):1088-1095.
More medical literature on Medic.Studio
More on the topic Role of Imaging Modalities in Obstetric Emergencies:
-
Infectious diseases -
Internal diseases -
Obstetrics and Gynaecology -
Pediatrics -
Veterinary medicine -
-
Conflictology -
Ecology -
Economy -
Finance -
History -
Law -
Medicine -
Philosophy -
Religious studies -
|