Chapter 5 Maternal–Fetal Physiology
This chapter deals primarily with APGO Educational Topic Areas:
TOPIC 8 MATERNAL–FETAL PHYSIOLOGY
TOPIC 13 POSTPARTUM CARE
Students should be able to discuss the normal maternal physiologic and anatomic changes in pregnancy and the postpartum as well as normal fetal physiology.
They should understand how these affect common laboratory and radiologic studies.Clinical Case
You are providing prenatal care for a young couple’s first pregnancy that has proceeded without complication through 38 weeks of gestational age. They come to your office for urgent consultation, fearful for the mother’s life because of her newly diagnosed heart disease. They request prompt referral to a good cardiologist. Upon taking a careful history, you learn they had traveled to a nearby mountain resort for the weekend, 2,000 feet higher above sea level than here at home. Upon arriving, she had experienced new and very disturbing dyspnea and had been seen in an Urgent Care Clinic where a normal electrocardiogram was obtained, but a chest x-ray was reported as grossly abnormal, with her heart “seriously enlarged and deviated from its normal position” consistent with new, severe heart disease.
 MATERNAL PHYSIOLOGY
MATERNAL PHYSIOLOGY
Cardiovascular System
The earliest and most dramatic changes in maternal physiology are cardiovascular. These changes improve fetal oxygenation and nutrition.
Anatomic Changes
During pregnancy, the heart is displaced upward and to the left and assumes a more horizontal position as its apex is moved laterally (Fig. 5.1). These position changes are the result of diaphragmatic elevation caused by displacement of abdominal viscera by the enlarging uterus. In addition, ventricular muscle mass increases and both the left ventricle and atrium increase in size parallel with an increase in circulating blood volume.
Pregnancy-associated changes in the cardiac position on a chest x-ray may be confused with cardiac pathology until the pregnancy is recognized.Functional Changes
The primary functional change in the cardiovascular system in pregnancy is a marked increase in cardiac output. Overall, cardiac output increases from 30% to 50%, with 50% of that increase occurring by 8 weeks of gestation. In the first half of pregnancy, cardiac output rises as a result of increased stroke volume and, in the latter half of pregnancy, as a result of increased maternal heart rate, whereas the stroke volume returns to near-normal, nonpregnant levels. These changes in stroke volume are due to alterations in circulating blood volume and systemic vascular resistance. Circulating blood volume begins increasing by 6 to 8 weeks of gestation and reaches a peak increase of 45% by 32 weeks of gestation. Systemic vascular resistance decreases because of a combination of the smooth muscle–relaxing effect of progesterone, increased production of vasodilatory substances (e.g., prostaglandins, nitric oxide, and atrial natriuretic peptide), and arteriovenous shunting to the uteroplacental circulation.
However, late in pregnancy, cardiac output may decrease when venous return to the heart is impeded because of vena caval obstruction by the enlarging gravid uterus. At times, in term pregnancy, nearly complete occlusion of the inferior vena cava occurs, especially in the supine position, with venous return from the lower extremities shunted primarily through the dilated paravertebral collateral circulation.
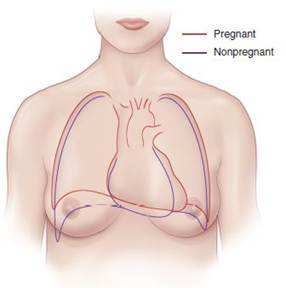
FIGURE 5.1. Changes in the outline of the heart, lungs, and thoracic cage. (Adapted from Bonica JJ, McDonald JS, eds. Principles and Practice of Obstetric Analgesia and Anesthesia. 2nd ed. Baltimore, MD: Williams & Wilkins; 1995:47, Fig. 2.)
The distribution of the enhanced cardiac output varies during pregnancy.
The uterus receives about 2% of the cardiac output in the first trimester, increasing to up to 20% at term, mainly by means of a relative reduction of the fraction of cardiac output that goes to the splanchnic bed and skeletal muscle. Thus, about one-fifth of the cardiac output goes through the uterus at term increasing the risk from postpartum hemorrhage substantially.However, the absolute blood flow to these areas does not change, because of the increase in cardiac output that occurs in late pregnancy. During pregnancy, arterial blood pressure follows a typical pattern. When measured in the sitting or standing position, diastolic blood pressure decreases beginning in the 7th week of gestation and reaches a maximal decline of 10 mm Hg from 24 to 26 weeks. Blood pressure then gradually returns to nonpregnant values by term. Resting maternal pulse increases as pregnancy progresses, increasing by 10 to 18 bpm over the nonpregnant value by term. Physiologic changes in blood pressure in midpregnancy may be misunderstood as hypotension unless allowance for gestational age is made.
During labor, at the time of uterine contraction, cardiac output increases approximately 40% above that in late pregnancy, and mean arterial pressure increases by approximately 10 mm Hg. A decline in these parameters following administration of an epidural anesthetic suggests that many of these changes are the result of pain and apprehension. Cardiac output increases significantly immediately after delivery, because venous return to the heart is no longer blocked by the gravid uterus impinging on the vena cava and because extracellular fluid is quickly mobilized.
Symptoms
Although most women do not become overtly hypotensive when lying supine, perhaps 1 in 10 has symptoms that include dizziness, light-headedness, and syncope. These symptoms, often termed the inferior vena cava syndrome, may be related to ineffective shunting via the paravertebral circulation when the gravid uterus occludes the inferior vena cava.
Physical Findings
The cardiovascular system is in a hyperdynamic state during pregnancy. Normal physical findings on cardiovascular examination include an increased second heart sound split with inspiration, distended neck veins, and low-grade systolic ejection murmurs, which are presumably associated with increased blood flow across the aortic and pulmonic valves. Many normal pregnant women have an S3 gallop, or third heart sound, after midpregnancy. Diastolic murmurs should not be considered normal in pregnancy. Some systolic murmurs may be normal in pregnancy, but diastolic murmurs should always engender evaluation for cardiac pathology.
Diagnostic Tests
Serial blood pressure assessment is an essential component of each prenatal care visit. Blood pressure recordings during pregnancy are influenced by maternal position; therefore, a consistent position should be used during prenatal care, facilitating the recognition of trends in blood pressure during pregnancy and their documentation. Measured blood pressure is highest when a pregnant woman is seated, somewhat lower when supine, and lowest while lying on the side. In the lateral recumbent position, the measured pressure in the superior arm is about 10 mm Hg lower than that simultaneously measured in the inferior arm. Blood pressures higher than the nonpregnant values for a particular patient should be presumed abnormal pending evaluation.
The normal anatomic changes of the maternal heart in pregnancy can produce subtle, but insignificant, changes in chest radiographs and electrocardiograms (ECGs). In chest radiographs, the cardiac silhouette can appear enlarged, causing a misinterpretation of cardiomegaly. In ECGs, a slight left-axis deviation may be apparent.
Respiratory System
The changes that occur in the respiratory system during pregnancy are necessitated by the increased oxygen demand of the mother and fetus. These changes are primarily mediated by progesterone.
Anatomic Changes
The maternal thorax undergoes several morphologic changes due to pregnancy.
The diaphragm is elevated approximately 4 cm by late pregnancy due to the enlarging uterus. Additionally, the subcostal angle widens as the chest diameter and circumference increase slightly (see Fig. 5.1).
FIGURE 5.2. Pulmonary volumes and capacities in the nonpregnant state and in the gravida at term. Values are given in cubic centimeters (cc). (Adapted from Bonica JJ, McDonald JS, eds. Principles and Practice of Obstetric Analgesia and Anesthesia. 2nd ed. Baltimore, MD: Williams & Wilkins; 1995:49, Figs. 2–4.)
Functional Changes
Pregnancy is associated with an increase in total body oxygen consumption of approximately 50 mL O2/minute, which is 20% greater than nonpregnant levels. Approximately 50% of this increase is consumed by the gravid uterus and its contents, 30% by the heart and kidneys, 18% by the respiratory muscles, and the remainder by the mammary tissues.
Functional adaptations in the pulmonary system enhance oxygen delivery to the lungs. Figure 5.2 lists respiratory volumes and capacities associated with pregnancy. The consequence of diaphragmatic elevation is a 20% reduction in the residual volume and functional residual capacity plus a 5% reduction in total lung volume. Although the maternal respiratory rate is essentially unchanged, there is a 30% to 40% increase in tidal volume due to a 5% increase in inspiratory capacity, resulting in a 30% to 40% increase in minute ventilation.
This significant increase in minute ventilation during pregnancy is associated with important changes in the acid–base equilibrium. Progesterone causes increased central chemoreceptor sensitivity to CO2, which results in increased ventilation and a reduction in arterial pco2. The respiratory alkalosis that results from a decreased arterial pco2 in pregnancy is compensated for by increased renal excretion of bicarbonate, yielding the lower bicarbonate levels normally seen in pregnancy, which means that maternal arterial pH is normal.
Symptoms
Although airway conductance and total pulmonary resistance are reduced in pregnancy, dyspnea is common in pregnant women. Dyspnea of pregnancy is believed to be a physiologic response to a low arterial pco2. Dyspnea during pregnancy may be “physiologic” but still requires evaluation insofar as it may represent respiratory or cardiac illness.
Allergy-like symptoms or chronic colds are also common. Mucosal hyperemia associated with pregnancy results in marked nasal stuffiness and an increased amount of nasal secretions.
Physical Findings
Despite the anatomic and functional changes in the respiratory system during pregnancy, no significant changes in the pulmonary examination are apparent.
Diagnostic Tests
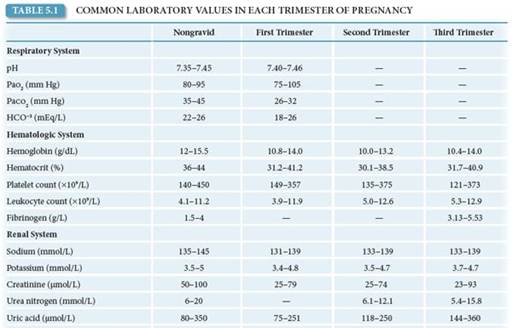
Arterial blood gas assessment during pregnancy normally shows a compensated respiratory alkalosis. Arterial pco2 levels of 27 to 32 mm Hg and bicarbonate levels of 18 to 31 mEq/L should be considered normal. Maternal arterial pH is maintained at normal levels of 7.40 to 7.45 (Table 5.1).
During normal pregnancy, chest radiography may demonstrate prominent pulmonary vasculature due to the increased circulating blood volume.
Hematologic System
The physiologic adaptations in the maternal hematologic system maximize the oxygen-carrying capacity of the mother to enhance oxygen delivery to the fetus. In addition, they minimize the effects of impaired venous return and blood loss associated with labor and delivery.
Anatomic Changes
The primary anatomic adaptation of the maternal hematologic system is a marked increase in plasma volume, red cell volume, and coagulation factors. Maternal plasma volume begins to increase as early as the sixth week of pregnancy and reaches a maximum at 30 to 34 weeks of gestation, after which it stabilizes. The mean increase in plasma volume is approximately 50% in singleton gestations and greater in multiple gestations. Red cell volume also increases during pregnancy, although to a lesser extent than plasma volume, averaging about 450 mL. Maternal blood volume increases 35% by term.
Adequate iron availability is essential to the increase in maternal red cell volume during pregnancy. The normal pregnant patient requires a total of 1,000 mg of additional iron: 500 mg is used to increase maternal red cell mass, 300 mg is transported to the fetus, and 200 mg is used to compensate for normal iron loss. Because iron is actively transported to the fetus, fetal hemoglobin (Hgb) levels are maintained regardless of maternal iron stores. Supplemental iron use in pregnancy is intended to prevent iron deficiency in the mother not to prevent either iron deficiency in the fetus or to maintain maternal Hgb concentration. To meet maternal iron needs in a woman who is not anemic, 60 mg of elemental iron is recommended daily.
Because iron from dietary sources may not be sufficient, the National Academy of Sciences recommends an iron supplement of 27 mg (present in most prenatal vitamins). In the form of ferrous sulfate, 60 mg of iron is a dosage of 300 mg. Patients who are anemic should receive 60 to 120 mg of iron. Leukocyte count and platelet counts may vary during pregnancy. White blood cell counts typically increase slightly in pregnancy, returning to nonpregnant levels during the puerperium. During labor, the white blood cell count may further increase, primarily from increased granulocytes, presumably linked with stress-associated demargination rather than a true disease-associated inflammatory response. Platelet counts may decline slightly but remain within the normal, nonpregnant range.
The concentration of numerous clotting factors is increased during pregnancy. Fibrinogen (factor I) increases by 50%, as do fibrin split products and factors VII, VIII, IX, and X. Prothrombin (factor II) and factors V and XII remain unchanged. In contrast, the concentration of key inhibitors of coagulation, activated protein C and protein S, decreases.
Functional Changes
During pregnancy, functional adaptations in maternal erythrocytes enable enhanced oxygen uptake in the lungs, allowing increased oxygen delivery to the fetus and promoting CO2 exchange from fetus to mother. The increase in oxygen delivery to the lungs and the amount of Hgb in the blood result in a significant increase in the total oxygen-carrying capacity. In addition, the compensated respiratory alkalosis of pregnancy causes a shift in the maternal oxygen dissociation curve to the left, via the Bohr effect. In the maternal lungs, Hgb affinity for oxygen increases, whereas in the placenta, the CO2 gradient between fetus and mother is increased, which facilitates transfer of CO2 from fetus to mother. See pp. 55-57 for further discussion.
The risk of thromboembolism doubles during pregnancy, which is considered a hypercoagulable state, and increases to 5.5 times the normal risk during the puerperium.
Symptoms and Physical Findings
Some edema is normal in pregnancy, and swelling of the hands, face, legs, ankles, and feet may occur. This tends to be worse late in pregnancy and during the summer.
Diagnostic Tests
Pregnancy results in alterations in the normal ranges of several hematologic indices. The disproportionate increase in plasma volume, compared with red cell volume, results in a decrease in Hgb concentration and hematocrit during pregnancy, often referred to as a physiologic anemia. At term, the average Hgb concentration is 12.5 g/dL, compared with approximately 14 g/dL in the nonpregnant state. Values less than 11.0 g/dL are usually due to iron deficiency, but such values should prompt investigation for other kinds of anemia that may occur simultaneously with iron deficiency anemia. Treatment of any anemia should be administered. The leukocyte count can range from 5,000 to 12,000/L and may increase to as much as 30,000/L during labor and the puerperium. Neither of these higher values is necessarily associated with infection.
The most notable alteration in the coagulation system is increased concentration of fibrinogen, which ranges from 300 to 600 mg/dL in pregnancy, compared with 200 to 400 mg/dL in the nonpregnant state. Despite the prothrombotic state of pregnancy, in vitro clotting times do not change.

Renal System
The renal system is the site of increased functional activity during pregnancy to maintain fluid, solute, and acid–base balance in response to the marked activity of the cardiorespiratory systems.
Anatomic Changes
The primary anatomic change of the renal system is enlargement and dilation of the kidneys and urinary collecting system. The kidneys lengthen by approximately 1 cm during pregnancy as a result of greater interstitial volume as well as distended renal vasculature. The renal calyces, pelves, and ureters dilate during pregnancy because of mechanical and hormonal factors. Mechanical compression of the ureters occurs as the uterus enlarges and rests on the pelvic brim. The right ureter is usually more dilated than the left, possibly due to dextrorotation of the uterus and compression from the enlarged right ovarian venous plexus. Progesterone causes relaxation of the smooth muscle of the ureters, which also results in dilation. In addition, because progesterone also decreases bladder tone, residual volume is increased. As the uterus enlarges as pregnancy progresses, bladder capacity decreases.
Functional Changes
The majority of pregnancy-associated functional changes in the renal system are a result of an increase in renal plasma flow. Early in the first trimester, renal plasma flow begins to increase, and, at term, it may be 75% greater than nonpregnant levels. Similarly, the glomerular filtration rate (GFR) increases to 50% over the nonpregnant state. This increase in GFR results in an increased load of various solutes presented to the renal system. Urinary glucose excretion increases in virtually all pregnant patients. A trace of glucose on routine prenatal colorimetric “dipstick” evaluation is normal and is usually not associated with glycemic pathology but should be watched closely for further trends into true glucosuria.
Amino acids and water-soluble vitamins, such as vitamin B12 and folate, are also excreted to a greater extent compared with the nonpregnant state. However, there is no significant increase in urinary protein loss, which means that any proteinuria that occurs during pregnancy should prompt consideration of illness. In addition, sodium metabolism remains unchanged. The potential loss of this electrolyte caused by an increased GFR is compensated for by an increase in renal tubule reabsorption of sodium.
All components of the renin–angiotensin–aldosterone system increase during pregnancy. Plasma renin activity is up to 10 times that of the nonpregnant state, and renin substrate (angiotensinogen) and angiotensin increase approximately fivefold. Normal pregnant women are relatively resistant to the hypertensive effects of the increased levels of renin– angiotensin–aldosterone, whereas women with hypertensive disease and hypertensive disease of pregnancy are not.
Symptoms
The anatomic changes in the renal system result in a few common symptomatic complaints during pregnancy. Compression of the bladder by the enlarged uterus results in urinary frequency that is not associated with urinary tract or bladder infection. Although urinary frequency is a distressing normal finding as pregnancy advances, care must be taken to distinguish such changes from those associated with early urinary tract infection. In addition, 20% of women experience stress urinary incontinence, and loss of urine should be considered in the differential diagnosis when rupture of membranes is suspected. Finally, urinary stasis throughout the renal collecting system predisposes to an increased incidence of pyelonephritis in patients with asymptomatic bacteriuria.
Physical Findings
As pregnancy advances, pressure from the presenting part on the maternal bladder can cause edema and protrusion of the bladder base into the anterior vagina. No significant changes in the renal examination are apparent during pregnancy.
Diagnostic Tests
The pregnancy-associated functional changes in the renal system result in a number of alterations in common tests of renal function. Serum levels of creatinine and blood urea nitrogen (BUN) decrease in normal pregnancy. Serum creatinine values fall from a nonpregnant level of 0.8 mg/dL to pregnancy levels of 0.5 to 0.6 mg/dL by term. Creatinine clearance increases 30% above the nonpregnant norms of 100 to 115 mL/min. BUN also falls about 25% to levels of 8 to 10 mg/dL at the end of the first trimester and is maintained at these levels for the remainder of the pregnancy. Because glucosuria is common during pregnancy, quantitative urine glucose measurements are often elevated but may not signify an abnormal blood sugar. By comparison, renal protein excretion is unchanged during pregnancy, and the nonpregnant range of 100 to 300 mg per 24 hours remains valid.
If imaging of the renal system is performed during pregnancy, normal dilation of the renal collecting system resembling hydronephrosis is noted on ultrasound or intravenous pyelogram.
Gastrointestinal System
The anatomic and functional changes in the gastrointestinal (GI) system that occur during pregnancy are due to the combined effect of the enlarging uterus and the hormonal action of pregnancy. These changes produce a number of pregnancy-related symptoms that can range from mild discomfort to severe disability.
Anatomic Changes
The primary anatomic change related to pregnancy is the displacement of the stomach and intestines due to the enlarging uterus. Although the stomach and intestines change in position, they do not change in size. The liver and biliary tract also does not change in size, but the portal vein enlarges due to increased blood flow.
Functional Changes
Functional changes in the GI system are the result of the hormonal action of progesterone and estrogen. Generalized smooth muscle relaxation mediated by progesterone produces lower esophageal sphincter tone, decreased GI motility, and impaired gallbladder contractility. As a result, transit time in the stomach and small bowel increases significantly—15% to 30% in the second and third trimesters and more during labor. Additionally, the imbalance between the lower intraesophageal pressures and increased intragastric pressures, combined with the lower esophageal sphincter tone, leads to gastroesophageal reflux. However, appropriately changing the maternal recumbent position may ameliorate pregnancy-associated mild gastroesophageal reflux. Reduced gallbladder contractility, in combination with estrogen-mediated inhibition of intraductal transportation of bile acids, leads to an increased prevalence of gallstones and cholestasis of bile salts. Estrogen also stimulates hepatic biosynthesis of proteins such as fibrinogen; ceruloplasmin; and the binding proteins for corticosteroids, sex steroids, thyroid hormones, and vitamin D.
Symptoms
Some of the earliest and most obvious symptoms of pregnancy are noted in the GI system. Although energy requirements vary from person to person, most women increase their caloric intake by about 200 kcal/day. Nausea and vomiting of pregnancy (NVP), or “morning sickness,” typically begins between 4 and 8 weeks of gestation and abates by the middle of the second trimester, usually by 14 to 16 weeks. The cause of this nausea is unknown, although it appears to be related to elevated levels of progesterone, human chorionic gonadotropin (hCG), and relaxation of the smooth muscle of the stomach. Severe NVP, which is known as hyperemesis gravidarum, can result in weight loss, ketonemia, and electrolyte imbalance.
Many patients report dietary cravings during pregnancy. Some may be the result of the patient’s perception that a particular food may help with nausea. Pica is an especially intense craving for substances such as ice, starch, and clay. Other patients develop dietary or olfactory aversions during pregnancy. Ptyalism is perceived by the patient to be the excessive production of saliva but probably represents the inability of a nauseated woman to swallow the normal amounts of saliva that are produced.
Symptoms of gastroesophageal reflux typically become more pronounced as pregnancy advances and intra-abdominal pressure increases. Constipation is common in pregnancy and is associated with mechanical obstruction of the colon by the enlarging bowel, reduced motility as elsewhere in the GI tract, and increased water absorption during pregnancy. Generalized pruritus may result from intrahepatic cholestasis and increased serum bile acid concentrations.
Physical Findings
The two most notable GI pregnancy-related physical findings are gingival disease and hemorrhoids. Although the incidence of dental caries does not change with pregnancy, the gums become more edematous and soft during pregnancy and bleed easily with vigorous brushing. On occasion, violaceous pedunculated lesions, called epulis gravidarum, appear at the gumline. These lesions, which are actually pyogenic granulomas, sometimes bleed very easily, but usually regress within 2 months of delivery. Rarely, excessive bleeding may occur, requiring excision of the granuloma. Hemorrhoids are common in pregnancy and are caused by both constipation and elevated venous pressures resulting from increased pelvic blood flow and the effects of the enlarging uterus.
Diagnostic Tests
Some markers of hepatic function may be altered during pregnancy. Total serum alkaline phosphatase concentration is doubled, mainly due to increased placental production. Serum cholesterol levels increase during pregnancy. Although total albumin increases, serum levels of albumin are lower during pregnancy, primarily due to hemodilation. Levels of aspartate transaminase, alanine transaminase, γ-glutamyl transferase, and bilirubin are largely unchanged or slightly lower. Serum amylase and lipase concentrations are also unchanged.
Endocrine System
Pregnancy influences the production of several endocrine hormones that control the physiologic adaptations in other organ systems.
Thyroid Function
Pregnancy produces an overall euthyroid state, despite several changes in thyroid regulation. The thyroid gland enlarges moderately during pregnancy but does not produce thyromegaly or goiter. In the first trimester, hCG, which has thyrotropin-like activity, stimulates maternal thyroxine (T4) secretion and produces a transient rise in the free T4 concentration (Fig. 5.3). The decline in placental hCG production following the first trimester results in normalization of free T4 concentrations. Beginning early in pregnancy, estrogen induces hepatic synthesis of thyroxine-binding globulin (TBG), resulting in an increase in total T4 and total triiodothyronine (T3) levels. Levels of free T4 and free T3, the active hormones, are unchanged from the normal range for nonpregnant patients.

FIGURE 5.3. Changes in maternal thyroid function during pregnancy. The effects of pregnancy on the mother include a marked and early increase in hepatic production of thyroxine-binding globulin (TBG) and placental production of human chorionic gonadotropin (hCG). The increase in serum TBG, in turn, increases serum thyroxine (T4) concentrations; hCG has thyrotropin-like activity and stimulates maternal T4 secretion. The transient hCG-induced increase in the serum-free T4 level inhibits maternal secretion of thyrotropin. (Adapted from Burrow GN, Fisher DA, Larsen R. Maternal and fetal thyroid function. N Engl J Med. 1994;331(16):1072–1078.)
Adrenal Function
Although pregnancy does not alter the size or morphology of the adrenal gland, it does influence hormone synthesis. As with TBG, estrogen induces hepatic synthesis of cortisolbinding globulin, resulting in elevated levels of serum cortisol. The concentration of free plasma cortisol progressively increases from the first trimester until term. Levels of corticotropin rise in conjunction with serum cortisol. Levels of aldosterone increase markedly due to enhanced adrenal synthesis. Maternal levels of deoxycorticosterone increase as the result of estrogen stimulation of renal synthesis, rather than increased adrenal production. Maternal levels of dehydroepiandrosterone sulfate decrease due to increased hepatic uptake and conversion to estrogen.
Metabolism
Carbohydrate Metabolism
Pregnancy has a diabetogenic effect on maternal carbohydrate metabolism, characterized by reduced tissue response to insulin, hyperinsulinemia, and hyperglycemia. Insulin resistance is primarily due to the action of human placental lactogen (hPL), which increases the resistance of peripheral tissues to the effects of insulin. The hormone hPL is secreted in proportion to placental mass, resulting in increased insulin resistance as pregnancy progresses. Progesterone and estrogen may also contribute to insulin resistance. Hepatic glycogen synthesis and storage is increased, and gluconeogenesis is inhibited. The net effect of these changes is that the maternal response to a glucose load is blunted, producing postprandial hyperglycemia.
Additionally, the fetoplacental unit serves as a constant drain on maternal glucose levels. Glucose is the primary fuel for the placenta and fetus and, thus, delivery of glucose from the mother to the fetus occurs by facilitated diffusion. As a result, maternal hypoglycemia develops during periods of fasting.
Lipid Metabolism
Pregnancy causes an increase in circulating concentrations of all lipids, lipoproteins, and apolipoproteins. During early pregnancy, fat storage in central tissues predominates. Later in pregnancy, lipolysis predominates, possibly triggered by maternal fasting hypoglycemia. In the absence of glucose, increased plasma concentrations of free fatty acids, triglycerides, and cholesterol provide energy for the mother; this has been characterized as accelerated starvation. Following delivery, the concentrations of all lipids return to nonpregnancy levels, a process accelerated by breastfeeding.
Protein Metabolism
Pregnancy is characterized by the intake and utilization of approximately 1 kg of protein above the normal nonpregnant state. At term, 50% of the additional protein is used by the fetus and placenta, and the remainder is shared by the uterus, breasts, maternal Hgb, and plasma proteins.
Other Maternal Systems
Musculoskeletal
As pregnancy advances, a compensatory lumbar lordosis (anterior convexity of the lumbar spine) is apparent. This change is functionally useful because it helps keep the woman’s center of gravity over the legs; otherwise, the enlarging uterus would shift it anteriorly. However, as a result of this change in posture, virtually all women complain of low back pain during pregnancy. Increasing pressure caused by intra-abdominal growth of the uterus may result in an exacerbation of hernia defects, most commonly seen at the umbilicus and in the abdominal wall (diastasis recti, a physiologic separation of the rectus abdominis muscles). Beginning early in pregnancy, the effects of relaxin and progesterone result in a relative laxity of the ligaments. The pubic symphysis separates at approximately 28 to 30 weeks. Patients often complain of an unsteady gait and should be cautioned about the increased risk of falls during pregnancy that result both from these body habitus changes and an altered center of gravity as pregnancy progresses.
To provide for adequate calcium supplies to the fetal skeleton, calcium stores are mobilized. Maternal serum-ionized calcium is unchanged from the nonpregnant state, but maternal total serum calcium decreases. There is a significant increase in maternal parathyroid hormone, which maintains serum calcium levels by increasing absorption from the intestine and decreasing the loss of calcium through the kidney. The skeleton is well maintained despite these elevated levels of parathyroid hormones. This may be because of the effect of calcitonin. Although the rate of bone turnover increases, there is no loss of bone density during a normal pregnancy if adequate nutrition is supplied.
Skin
Pregnancy induces several characteristic changes in the appearance of the maternal skin. Although the exact etiology of these changes has not been established, hormonal influences appear to predominate.
Vascular spiders (spider angiomata) are most common on the upper torso, face, and arms. Palmar erythema occurs in more than 50% of patients. Both are associated with increased levels of circulating estrogen and regress after delivery. Striae gravidarum occur in more than half of pregnant women and appear on the lower abdomen, breasts, and thighs. Initially, striae can be either purple or pink; eventually, they become white or silvery. These striae are not related to weight gain but are solely the result of the stretching of normal skin. There is no effective therapy to prevent these “stretch marks,” and, once they appear, they cannot be eliminated.
Pregnancy may produce characteristic hyperpigmentation, which is believed to be the result of elevated levels of estrogen and melanocyte-stimulating hormone and a cross-reaction with the structurally similar hCG. Hyperpigmentation commonly affects the umbilicus and perineum, although it may affect any skin surface. The lower abdomen linea alba darkens to become the linea nigra. The “mask of pregnancy,” or chloasma (melasma), is also common and may never disappear completely. Skin nevi can increase in size and pigmentation but resolve after pregnancy; however, removal of rapidly changing nevi is recommended during pregnancy because of the risk of malignancy. Eccrine sweating and sebum production increase during normal pregnancy, with many patients complaining of acne.
Hair growth during pregnancy is maintained, although there are more follicles in the anagen (growth) phase and fewer in the telogen (resting) phase. Late in pregnancy, the number of hairs in telogen is approximately half of the normal 20%, so that postpartum, the number of hairs entering telogen increases; thus, there is significant hair loss 2 to 4 months after pregnancy. Hair growth typically returns to normal 6 to 12 months after delivery. Patients are often concerned about this “hair loss,” until they are reassured that it is transient and that hair growth will renew.
Reproductive Tract
The effects of pregnancy on the vulva are similar to the effects on other skin. Because of an increase in vascularity, vulvar varicosities are common and usually regress after delivery. An increase in vaginal transudation as well as stimulation of the vaginal epithelium results in a heavier vaginal discharge, called leukorrhea of pregnancy, that some women may mistake as infection or ruptured membranes. The epithelium of the endocervix everts onto the ectocervix, which is associated with a mucus plug.
During pregnancy, the uterus undergoes an enormous increase in weight from the 70-g nonpregnant size to approximately 1,100 g at term, primarily through hypertrophy of existing myometrial cells. After pregnancy, the uterus returns to only a slightly increased size as the actual number of cells comprising it is minimally increased. Similarly, the uterine cavity enlarges to a volume of up to as much as 5 L, compared with less than 10 mL in the nongravid state.
Breasts
The breasts increase in size during pregnancy, rapidly in the first 8 weeks and steadily thereafter. In most cases, the total enlargement is 25% to 50%. The nipples become larger and more mobile and the areola larger and more deeply pigmented, with enlargement of the Montgomery glands. Blood flow to the breasts increases as they change to support lactation. Some patients may complain of breast or nipple tenderness and a tingling sensation. Estrogen stimulation also results in ductal growth, with alveolar hypertrophy being a result of progesterone stimulation. During the latter portion of pregnancy, a thick, yellow fluid can be expressed from the nipples. This is colostrum, more common in parous women. Ultimately, lactation depends on synergistic actions of estrogen, progesterone, prolactin, hPL, cortisol, and insulin.
Ophthalmic
The most common visual complaint during pregnancy is blurred vision. This visual change is primarily caused by increased thickness of the cornea associated with fluid retention and decreased intraocular pressure. These changes manifest in the first trimester and regress within the first 6 to 8 weeks postpartum. Therefore, changes in corrective lens prescriptions should not be encouraged during pregnancy. Women may be reassured that changes in vision during normal pregnancy are usually transient, not requiring glasses after delivery.
 FETAL AND PLACENTAL PHYSIOLOGY
FETAL AND PLACENTAL PHYSIOLOGY
Placenta
The placenta is an essential and unique “organ of pregnancy,” with key functions in respiratory and metabolite exchange and in hormone synthesis and regulation. It is the crucial point of connection between the mother and fetus. The placenta allows the fetus to live and grow until it is mature and able to survive in the outside world.
All gases involved in fetal respiration cross the placenta by simple diffusion. Fetal uptake of O2 and excretion of CO2 depend on the blood-carrying capacities of the mother and fetus for these gases and on the associated uterine and umbilical blood flows.
The single primary metabolic substrate for placental metabolism is glucose. It is estimated that as much as 70% of the glucose transferred from the mother is used by the placenta. The glucose that crosses the placenta does so by facilitated diffusion. Other solutes that are transferred from the mother to the fetus depend on the concentration gradient as well as on their degree of ionization, size, and lipid solubility. There is active transport of amino acids, resulting in levels that are higher in the fetus than in the mother. Free fatty acids have very limited placental transfer, resulting in levels that are lower in the fetus than in the mother.
The placenta also produces estrogen, progesterone, hCG, and hPL. These hormones are important for the maintenance of pregnancy, for labor and delivery, and for lactation.
Fetal Circulation
Oxygenation of fetal blood occurs in the placenta rather than in the fetal lungs. This oxygenated blood (80% saturated) is carried from the placenta to the fetus through the umbilical vein, which enters the portal system of the fetus and branches off to the left lobe of the liver (Fig. 5.4). The umbilical vein then becomes the origin of the ductus venosus. Another branch joins the blood flow from the portal vein to the right lobe of the liver. Fifty percent of the umbilical blood supply goes through the ductus venosus. The blood flow from the left hepatic vein is mixed with the blood in the inferior vena cava and is directed toward the foramen ovale. Consequently, the well-oxygenated umbilical vein blood enters the left ventricle. Less-oxygenated blood in the right hepatic vein enters the inferior vena cava and then flows through the tricuspid valve into the right ventricle. Blood from the superior vena cava also preferentially flows through the tricuspid valve to the right ventricle. Blood from the pulmonary artery primarily flows through the ductus arteriosus into the aorta.
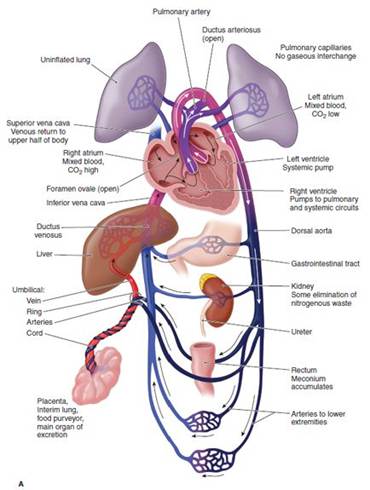
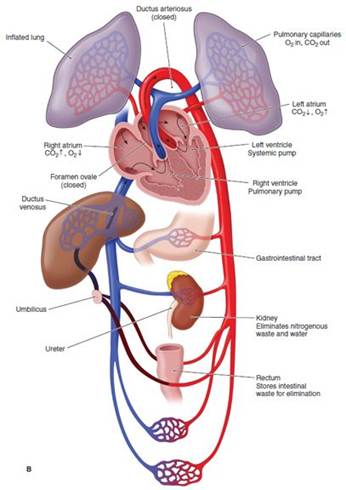
FIGURE 5.4. Fetal circulation at term (A) and after delivery (B). Note the changes in function of the ductus venosus, foramen ovale, and ductus arteriosus in the transition from intrauterine to extrauterine existence. Red, oxygenated blood; pink/purple, partially oxygenated blood; blue, deoxygenated blood.
The fetal ventricles work in a parallel circuit, with blood flow from the right and left unequally distributed to the pulmonary and systemic vascular beds. Within a fetal heart rate range of 120 to 180 bpm, the fetal cardiac output remains relatively constant. Overall, less than 10% of right ventricular cardiac output goes to the fetal lungs. The remainder of the right ventricular cardiac output is shunted through the ductus arteriosus to the descending aorta. Output from the left ventricle into the proximal aorta supplies highly saturated blood (65% saturated) to the brain and upper body. Once joined by the ductus arteriosus, the descending aorta then supplies blood to the lower portion of the fetal body, with a major portion of this blood being delivered to the umbilical arteries, which carry deoxygenated blood to the placenta.
The umbilical blood flow represents about 40% of the combined output of both fetal ventricles. In the last half of pregnancy, this flow is proportional to fetal growth (approximately 300 mL/mg/minute), so that umbilical blood flow is relatively constant, normalized to fetal weight. This relationship allows measurement of fetal blood flow to be used as an indirect measure of fetal growth and fetal well-being.
Hemoglobin and Oxygenation
Fetal Hgb, like adult Hgb, is a tetramer composed of two copies of two different peptide chains. But unlike adult hemoglobin A (HgbA), which is composed of α- and β-chains, fetal Hgb is composed of a series of different pairings of peptide chains that change as embryonic and fetal development progresses. In late fetal life, hemoglobin F (HgbF), composed of two α-chains and two β-chains, predominates. The key physiologic difference between adult HgbA and fetal HgbF is that, at any given oxygen tension, HgbF has higher oxygen affinity and oxygen saturation than HgbA. The main reason for this functional difference is that HgbA binds 2,3-DPG (diphosphoglycerate) more avidly than does HgbF.
The Bohr effect modulates the oxygen-binding capacity of Hgb and plays an important role in exchange of O2 and CO2 between the maternal and fetal circulations. As maternal blood enters the placenta, the maternal respiratory alkalosis facilitates transfer of CO2 from the fetal circulation to the maternal circulation. Loss of CO2 from the fetal circulation causes a rise in the fetal blood pH, shifting the fetal oxygen dissociation curve to the left and resulting in increased oxygen binding affinity (Fig. 5.5). Conversely, as the maternal circulation takes up CO2, the blood pH decreases, resulting in a shift in the maternal oxygen dissociation curve to the left, reducing oxygen affinity. Hence, a favorable gradient is created, facilitating diffusion of O2 from the maternal to the fetal circulation. Therefore, although the partial pressure of oxygen in fetal arterial blood is only 20 to 25 mm Hg, the fetus is adequately oxygenated.
Kidney
The fetal kidney becomes functional in the second trimester, producing dilute, hypotonic urine. The rate of fetal urine production varies with fetal size and ranges from 400 to 1,200 mL/day. Fetal urine becomes the primary source of the amniotic fluid by the middle of the second trimester.
Liver
The fetal liver is slow to mature. The fetal liver capacity for glycogen synthesis and bilirubin conjugation increases with gestational age. As a consequence, during fetal life, bilirubin is primarily eliminated through the placenta. Hepatic production of coagulation factors is deficient and may be attenuated in newborn life due to vitamin K deficiency. Routine neonatal administration of vitamin K prevents newborn hemorrhagic disorders.
Thyroid Gland
The fetal thyroid gland develops without direct influence from the mother, becoming functional by the end of the first trimester, so that, thereafter, levels of fetal T3, T4, and TBG increase throughout the rest of gestation. The placenta does not transport the thyroid-stimulating hormone, and only moderate amounts of T3 and T4 cross the placenta. The mother is the primary source of the thyroid hormone for the fetus prior to 24 to 28 weeks of gestation.

FIGURE 5.5. HgbA vs. HgbF oxygen saturation curve. The oxygen saturation curve for fetal hemoglobin (blue) appears left-shifted when compared with adult hemoglobin (red), because fetal hemoglobin has a greater affinity for oxygen.
Gonads
The primordial germ cells migrate during the eighth week of gestation from the endoderm of the yolk sac to the genital ridge. At this point, the gonads are undifferentiated. Differentiation into the testes occurs 6 weeks after conception, if the embryo is 46, XY. This testicular differentiation appears to depend on the presence of the H–Y antigen and the Y chromosome. If the Y chromosome is absent, however, an ovary develops from the undifferentiated gonad. Development of the fetal ovary begins at approximately 7 weeks. The development of other genital organs depends on the presence or absence of specific hormones and is independent of gonadal differentiation. If the fetal testes are present, testosterone and the Müllerian inhibitory factor inhibit the development of female external genitalia. If these two hormones are not present, the female genitalia develop, with regression of the Wolffian ducts.
 IMMUNOLOGY OF PREGNANCY
IMMUNOLOGY OF PREGNANCY
Although the maternal immune system is not altered in pregnancy, the antigenically dissimilar fetus is able to survive in the uterus without being rejected. The key to this successful fetal allograft appears to be the placenta. The placenta serves as an effective interface between the maternal and fetal vascular compartments by keeping the fetus from direct contact with the maternal immune system. The placenta also produces estrogen, progesterone, hCG, and hPL, all of which may contribute to suppression of maternal immune responses on a local level. In addition, the placenta is the site of origin for blocking and masking antibodies, which alter the immune response.
The mother’s systemic immune system remains intact, as evidenced by leukocyte count, B- and T-cell count and function, and immunoglobulin (Ig) levels. Because IgG is the only Ig that can cross the placenta, maternal IgG comprises a major proportion of fetal Ig, both in utero and in the early neonatal period. In this fashion, passive immunity is transferred to the fetus.
In this environment, the fetal immune system is afforded the opportunity to gradually develop and mature by term. Fetal lymphocyte production begins as early as 6 weeks of gestation. By 12 weeks of gestation, IgG, IgM, IgD, and IgE are present and are produced in progressively increasing amounts throughout pregnancy. At birth, the newborn fetus is equipped with both passive immunity and a mature immunologic system to defend against infectious diseases.
Clinical Follow-Up
Your patient is 20 years old and has a completely negative medical history. On physical examination, her blood pressure and pulse rate are normal as is auscultation of her heart and lungs. After this examination, you explain that shortness of breath (dyspnea) is normal in pregnancy because of a lowered CO2 level. In her case, it is probable that she had not noted this until her abrupt introduction into a high-altitude environment. You also show her a picture of a chest x-ray during pregnancy, explaining that her heart is quite normal, simply displaced upward, and somewhat sideways by her growing baby. Reassured, they continue prenatal care and subsequently she has a normal vaginal delivery of a healthy daughter 2 weeks after this visit.
thePoint Visit http://thePoint.lww.com/activate for an interactive USMLE-style question bank and more!