Chapter 6 Preconception and Antepartum Care
This chapter deals primarily with APGO Educational Topic Areas:
TOPIC 9 PRECONCEPTION CARE
TOPIC 10 ANTEPARTUM CARE
Students should be able to describe how medical conditions affect pregnancy outcomes and to counsel patients on appropriate interventions to optimize preconceptional health.
They should be able to describe typical care of the pregnant patient, including accurate diagnosis of pregnancy, medication safety, risk factors for poor outcome, assessments for fetal well-being, and nutritional needs.Clinical Case
A 36-year-old nulliparous woman presents to your office for her first prenatal visit. She is unsure of her last menstrual period as she recently discontinued her birth control pills, but thinks it was 2 months ago. In addition to worrying about her baby having abnormalities related to her age, she is an early elementary school teacher and is concerned about exposure to childhood illnesses. Since she is “older,” she is concerned that she may not have other children and really wants to optimize the outcome of this pregnancy. What will you do during her first obstetric visit? What screening will you offer her? How will you counsel her regarding her goal for a healthy pregnancy?
 PRECONCEPTION COUNSELING AND CARE
PRECONCEPTION COUNSELING AND CARE
Preconception counseling and care is intended to optimize a woman’s health for pregnancy, ideally commencing before conception, with a preconception visit. During this visit, a thorough family and medical history of both parents is obtained as well as a physical examination of the prospective mother. The goal of this visit is to minimize adverse health effects for the woman and fetus and to promote a healthy pregnancy. Preexisting conditions that may affect conception, pregnancy, or both are identified and addressed.
For example, neural tube defects (NTDs) are associated with folic acid deficiency. Discussion about folic acid supplementation is an essential component of preconception. In addition, women with conditions such as maternal phenylketonuria or diabetes can reduce the risks of adverse fetal effects by establishing strict metabolic control before conception and continuing it throughout the pregnancy. In the absence of preconception metabolic control, establishing control of these conditions early in pregnancy, while of lesser benefit, may minimize morbidity and mortality later in gestation.All health encounters during a woman’s reproductive years, particularly those that are a part of preconception care, should include counseling about appropriate medical care and behaviors to optimize pregnancy outcomes. The following maternal assessments may serve as the basis for this counseling:
• Family planning and pregnancy spacing
• Medical, surgical, psychiatric, and neurologic histories
• Obstetric and gynecologic history
• Family history
• Genetic history
• Current medications (prescribed, over-the-counter [OTC], and alternative medicines)
• Substance use (tobacco, alcohol, illicit drugs, and OTC drugs such as cold medications)
• Domestic abuse and violence; bullying
• Sexual abuse
• Nutrition
• Environmental and occupational exposures
• Immunity and immunization status
• Risk factors for sexually transmitted diseases (STDs)
• Physical examination (especially blood pressure with attention to prehypertension and hypertension categories and appropriate weight based on body mass index [BMI])
• Assessment of socioeconomic, education, and cultural context
Vaccinations should be offered to women found to be at risk for or susceptible to rubella, varicella, pertussis, and hepatitis B. All pregnant women should be tested for human immunodeficiency virus (HIV) infection, unless they decline the test. Testing should be offered to women planning a pregnancy.
A number of other tests can be performed for specific indications:• Screening for STDs
• Testing for maternal diseases based on medical or reproductive history
• Mantoux test with purified protein derivative for tuberculosis by epidermal injection technique and not by use of “tine” instruments
• Screening for genetic disorders based on racial and ethnic background:
• Sickle hemoglobinopathies (African Americans)
• β-Thalassemia (individuals of Mediterranean and Southeast Asian descent; African Americans)
• α-Thalassemia (individuals of Southeast Asian and Mediterranean descent; African Americans)
• Tay-Sachs disease (Ashkenazi Jews, French Canadians, and Cajuns)
• Canavan disease and familial dysautonomia (Ashkenazi Jews)
• Cystic fibrosis (similar to SMA, carrier frequency is higher among Caucasians of European and Ashkenazi descent; however, screening should be made available to all couples)
• Screening for other genetic disorders on the basis of family history
Patients should be counseled regarding the benefits of the following activities:
• Maintaining good control of any preexisting medical conditions (e.g., diabetes, hypertension, asthma, systemic lupus erythematosus, seizures, thyroid disorders, and inflammatory bowel disease)
• Taking 0.4 mg of folic acid daily while attempting pregnancy and during the first trimester of pregnancy for prevention of NTDs; women who have had a prior NTDaffected pregnancy, or using medications that interfere with folate metabolism, should consume 4 mg of folic acid per day in the preconception period (this amount can be achieved by adding a separate supplement to a single multivitamin tablet to provide a total of 4 mg of folic acid while avoiding excessive intake of fat-soluble vitamins, which may have adverse fetal effects if taken in high doses)
• Determining the time of conception by an accurate menstrual history
• Reducing weight before pregnancy, if obese; increasing weight, if underweight
• Exercise
• Avoiding food faddism
• Avoiding pregnancy within 1 month of receiving a live attenuated vaccine (e.g., rubella)
• Preventing HIV infection
• Abstaining from tobacco, alcohol, and illicit drug use before and during pregnancy
 ANTEPARTUM CARE
ANTEPARTUM CARE
Women who receive early and regular antepartum care are more likely to have healthier infants.
The goals of obstetric care are to 1) provide easy access to care, 2) promote patient involvement, and 3) provide a team approach to ongoing surveillance and education for the patient and about her fetus. High-risk conditions can be identified and a management plan established for any complications that may arise. Routine antepartum care provides an opportunity for screening, periodic assessments, and patient education.Antepartum surveillance begins with the first prenatal visit. At this time, the health care provider begins to compile an obstetric database of information. Appendix C contains a format for documenting information. Complete antepartum care includes the following:
• Diagnosing pregnancy and determining gestational age
• Monitoring the progress of the pregnancy with periodic examinations and appropriate screening tests
• Assessing the well-being of the woman and her fetus
• Providing patient education that addresses all aspects of pregnancy
• Preparing the patient and her family for her management during labor, delivery, and the postpartum period
• Detecting medical and psychosocial complications and instituting indicated interventions
An important aspect of prenatal/antepartum care is to educate the mother and her family about the value of screening for and managing the unexpected complications that may develop. Specific conditions to which poor maternal and neonatal outcomes are often attributed include preterm labor and preterm delivery, preterm infection, intrauterine growth restriction (IUGR), hypertension and preeclampsia, diabetes mellitus, birth defects, multiple gestation, and abnormal placentation.
DIAGNOSIS OF PREGNANCY
For a woman with regular menstrual cycles, a history of one or more missed periods following a time of sexual activity without effective contraception strongly suggests early pregnancy. Fatigue, nausea/vomiting, and breast tenderness are often associated symptoms.
On physical examination, softening and enlargement of the pregnant uterus becomes apparent 6 or more weeks after the last normal menstrual period. At approximately 12 weeks of gestation (12 weeks from the onset of the last menstrual period [LMP]), the uterus is generally enlarged sufficiently to be palpable in the lower abdomen. Other genital tract findings early in pregnancy include congestion and a bluish discoloration of the vagina (chadwick sign) and softening of the cervix (Hegar sign). Increased pigmentation of the skin and the appearance of circumlinear striae on the abdominal wall occur later in pregnancy and are associated with progesterone effects and physical stretching of the dermis. Palpation of fetal parts and the appreciation of fetal movement and fetal heart tones are diagnostic of pregnancy but at a more advanced gestational age. The patient’s initial perception of fetal movement (called quickening) is not usually reported before 16 to 18 weeks of gestation and often as late as 20 weeks in first-time mothers.
Pregnancy cannot be diagnosed only on the basis of symptoms and subjective physical findings. A pregnancy test is needed to confirm the diagnosis. Once a positive pregnancy test is identified and before fetal heart activity (i.e., a beating fetal heart) is seen on ultrasound, the physician and patient must be aware of signs and symptoms of an abnormal pregnancy, including those associated with spontaneous abortion, ectopic pregnancy, and trophoblastic disease. Several types of urine pregnancy tests are available that measure human chorionic gonadotropin (hcG) produced in the syncytiotrophoblast of the growing placenta. Because hCG shares an α-subunit with luteinizing hormone (LH), interpretation of any test that does not differentiate LH from hCG must take into account this overlap in structure. The concentration of hCG necessary to evoke a positive test result must therefore be high enough to avoid a false-positive diagnosis of pregnancy.
Standard laboratory urine pregnancy tests become positive approximately 4 weeks following the first day of the LMP (i.e., around the time of the missed period). Home urine pregnancy tests have a low false-positive rate but a high false-negative rate (i.e., the test result is negative even though the patient is pregnant). All urine pregnancy tests are best performed on early-morning urine specimens, which contain the highest concentration of hCG.Serum pregnancy tests are more specific and sensitive because they test for the unique β-subunit of hCG, allowing detection of pregnancy very early in gestation, often before the patient has missed a period. During the first few weeks, the status of a pregnancy may be evaluated by following serial quantitative hCG levels and comparing them to the expected rise derived from normative data for proven normal intrauterine pregnancies. The mean doubling time for hCG in patients with a viable intrauterine pregnancy is approximately 1.5 to 2.0 days. Such serial studies often allow differentiation of normal and abnormal pregnancy or indicate that further testing of other kinds is needed for the same purpose.
Detection of fetal heart activity (fetal heart tones) is also almost always evidence of a viable intrauterine pregnancy. With a traditional, nonelectronic, acoustic fetoscope, auscultation of fetal heart tones is possible at or beyond 18 to 20 weeks of gestational age. The commonly used electronic Doppler devices can usually detect fetal heart tones at approximately 12 weeks of gestation (or perhaps a little later if the mother is obese).
THE INITIAL PRENATAL VISIT
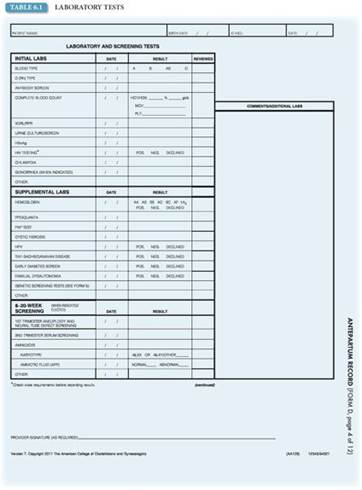
At the initial prenatal appointment, a comprehensive history is taken, focusing on past pregnancies, gynecologic history, medical history with attention to chronic medical issues and infections, information pertinent to genetic screening, and information about the course of the current pregnancy. A complete physical examination is performed, including breast and pelvic examinations, as well as routine first-trimester laboratory studies (Table 6.1). Other studies may be performed as indicated. The patient is given instructions concerning routine prenatal care, warning signs of complications, whom to contact with questions or problems, and nutritional and social service information.
The initial obstetric pelvic examination also includes a description of the various diameters of the bony pelvis (see Chapter 4), assessment of the cervix (including cervical length, consistency, dilation, and effacement), and size (usually expressed in weeks), shape, consistency (firm to soft), and mobility. When the uterus grows in size so that it exits the pelvis, the fundal height in centimeters represents the gestational age of the fetus from that time to about 36 weeks.
Risk Assessment
Risk assessment is an important part of the initial antenatal evaluation. Questions about history and chronic medical conditions are important in order to identify the pregnant woman who is at risk for maternal and fetal complications and to initiate a management plan at the appropriate time. In addition to understanding the medical risks, it is important to understand each woman’s social circumstances, some of which may place her at risk for both physical and emotional complications. Patients should be questioned about the following aspects of their lifestyle that could pose a risk and receive appropriate counseling, if indicated:
• Nutrition and weight gain counseling
• Sexual activity
• Exercise
• Smoking
• Environmental and work hazards
• Alcohol
• Traditional and home medications; OTC medications (for example, cough medications)
• Illicit/recreational drugs
• Domestic violence
• Sexual abuse
• Seat belt use
Initial Assessment of Gestational Age: Estimated Date of Delivery
Gestational age is the number of weeks that have elapsed between the first day of the LMP (not the presumed time of conception) and the date of delivery. Establishing an accurate estimated gestational age and estimated date of delivery (EDD) is an important part of the initial antepartum visit. Issues such as prematurity and postterm pregnancy and their subsequent management as well as the timing of screening tests (i.e., maternal serum screening for trisomy 21 and NTDs and assessment of fetal maturity) are affected by the accuracy of gestational age.
The Naegele rule is an easy way to calculate the EDD: add 7 days to the first day of the last normal menstrual flow and subtract 3 months. In a patient with an idealized 28-day menstrual cycle, ovulation occurs on day 14; therefore, the conception age of the pregnancy is actually 38 weeks. The use of the first day of the LMP as a starting point for gestational age is standard, and gestational, not conceptional, age is used. “Normal” pregnancy lasts 40 ± 2 weeks, calculated from the first day of the last normal menses (menstrual or gestational age).
To establish an accurate gestational age, the date of onset of the last normal menses is crucial. A light-bleeding episode should not be mistaken for a normal menstrual period. A history of irregular periods or taking medications that alter cycle length (e.g., oral contraceptives, other hormonal preparations, and psychoactive medications) can confuse the menstrual history. If sexual intercourse is infrequent or timed for conception based on assisted reproductive techniques, a patient may know when conception is most likely to have occurred, thus facilitating an accurate calculation of gestational age. However, ultrasound-established dates should take preference over menstrual dates.
Ultrasound examination can detect pregnancy early in gestation. With an abdominal ultrasound, the ultrasound transducer is placed on the maternal abdomen, allowing visualization of a normal pregnancy gestational sac 5 to 6 weeks after the beginning of the last normal menstrual period (corresponding to β-hCG concentrations of 5,000– 6,000 mIU/mL). Transvaginal ultrasound often detects pregnancy at 3 to 4 weeks of gestation (corresponding to β-hCG concentrations of 1,000–2,000 mIU/mL) because the probe is placed in the posterior fornix of the vagina only a few centimeters from the uterine cavity, compared with the relatively longer distance from the abdominal wall to the same location. A β-hCG of 1,500 mIU/mL is often used as the cutoff beyond which an intrauterine gestational sac should be visualized when ruling out an ectopic pregnancy. If the β-hCG concentration is >4,000 mIU/mL, the embryo should be visualized and cardiac activity detected by all ultrasound techniques.
SUBSEQUENT ANTENATAL VISITS
Regular monitoring of the mother and fetus is essential for identifying complications that may arise during pregnancy and to provide assurance and support for mother and family, especially for first pregnancies or when previous pregnancies have been complicated or had unfortunate outcomes. For a patient with a normal pregnancy, periodic antepartum visits at 4-week intervals are usually scheduled until 28 weeks, every 2 weeks until 36 weeks, and weekly thereafter. Patients with high-risk pregnancies or those with ongoing complications are usually seen more frequently, depending on the clinical circumstances. At each visit, patients are asked about how they are feeling and if they are having any problems, such as vaginal bleeding, nausea and vomiting, dysuria, and vaginal discharge. After quickening, patients are asked if they continue to feel fetal movement and if it is the same or less since the last antepartum visit. Decreased fetal movement after the time of fetal viability is a warning sign requiring further evaluation of fetal well-being.
Every prenatal assessment includes the following assessments:
• Blood pressure
• Weight
• Obstetric physical findings
Blood Pressure and Urinalysis
It is important to determine baseline blood pressure and urine protein levels at the first antepartum visit. Blood pressure generally declines at the end of the first trimester and rises again in the third trimester. After 20 weeks of gestation, an elevated systolic pressure above 140 mm Hg or an elevated diastolic pressure of more than 90 mm Hg without proteinuria suggests gestational hypertension (see Chapter 22). Comparison with baseline levels is necessary in order to accurately distinguish preexisting hypertension from hypertension associated with pregnancy.
Weight
Maternal weight is another important parameter to follow through pregnancy, insofar as weight gain recommendations differ for women of differing prepregnancy BMI. A total weight gain of 25 to 35 lb is only appropriate for a woman of normal BMI (Table 6.2). The obese pregnant woman with a pregravid BMI ≥ 30 is at risk for multiple complications during pregnancy, including preeclampsia, gestational diabetes, and cesarean delivery. Between monthly visits, a 3-to 4-lb weight gain is generally appropriate for a woman of normal BMI. Significant deviation from this trend may require nutritional assessment and further evaluation.

Physical Findings
Obstetric physical findings made at each visit include fundal height measurement, documentation of the presence and rate of fetal heart tones, and determination of the presentation of the fetus. Until 16 to 20 weeks, the uterine size is generally stated as weeks size, such as “12-week uterus.”
Fundal Height Measurement
After 20 weeks of gestation (when the fundus is palpable at or near the umbilicus in a woman of normal body habitus and a singleton pregnancy in the vertex presentation), the uterine size can be assessed with the use of a tape measure, which is the fundal height measurement. In this procedure, the top of the uterine fundus is identified, and the zero end of the tape measure is placed at this uppermost part of the uterus. The tape is then carried anteriorly across the abdomen to the level of the symphysis pubis. From 16 to 18 weeks of gestation until 36 weeks of gestation, the fundal height in centimeters (measured from the symphysis to the top of the uterine fundus) is roughly equal to the number of weeks of gestational age in normal singleton pregnancies in the cephalic presentation within an anatomically normal uterus (Fig. 6.1). Until 36 weeks in the normal singleton pregnancy, the number of weeks of gestation approximates the fundal height in centimeters. Thereafter, the fetus moves downward into the pelvis beneath the symphysis pubis (“lightening” or engagement of the head into the true pelvis), so that the fundal height measurement is increasingly unreliable.
Fetal Heart Rate
Fetal heart rate should be verified at every visit, by direct auscultation or by the use of a fetal Doppler ultrasound device. The normal fetal heart rate is 110 to 160 bpm, with higher rates found in early pregnancy. The maternal pulse may also be detected with the Doppler device, so simultaneous palpation of maternal pulse and auscultation of fetal pulse may be necessary to differentiate the two. Deviation from the normal rate or occasional arrhythmias must be evaluated carefully.

FIGURE 6.1. Fundal height. In a normal singleton pregnancy in the vertex presentation, fundal height roughly corresponds to gestational age between 16 and 36 weeks’ gestation. A convenient guideline is 20 weeks equals 20 cm equals fundus at umbilicus in a woman with a normal body habitus. After 36 weeks, the fundal height either grows more slowly or actually decreases as the uterus changes shape and/or the fetal head engages in the pelvis.
Uterine palpation
Several determinations concerning the fetus can be made by palpation of the pregnant uterus, such as identifying the presentation, or “presenting part” of the fetus (i.e., what part of the fetus is entering the pelvis first). Before 34 weeks of gestation, breech, oblique, and transverse presentations are not uncommon. The presentation of the fetus may also vary from day to day. At term, more than 95% of fetuses are in the cephalic presentation (head down). Approximately 3.5% are breech (bottom first) and 1% are shoulder first. Unless the fetus is in a transverse lie (the long axis of the fetus is not parallel with the mother’s long axis), the presenting part will be either the head (vertex and cephalic) or the buttocks (breech).
Fetal Presentation
The presentation of the fetus can be appreciated on clinical examination with the use of Leopold maneuvers (see Fig. 9.7). In the first maneuver, breech presentation can be appreciated by outlining the fundus and determining what part is present. The head is hard and well defined by ballottement, especially when the head is freely mobile in the fluid-filled uterus; the breech is softer, less round, and, therefore, more difficult to outline. In the second and third maneuvers, the examiner’s palms are placed on either side of the maternal abdomen to determine the location of the fetal back and small parts. In the fourth maneuver, the presenting part is identified by exerting pressure over the pubic symphysis. If a breech presentation persists at 36 and 38 weeks, the option of external cephalic version should be discussed with the patient. This procedure involves turning the fetus from the breech presentation to a vertex presentation to allow vaginal rather than cesarean delivery. It is contraindicated in the presence of multifetal gestation, fetal compromise, uterine anomalies, and problems of placentation.
ULTRASOUND
In the United States, approximately 65% of pregnant women have at least one ultrasound examination. The optimal timing for a single ultrasound examination in the absence of specific indications for a first-trimester examination is at 18 to 20 weeks of gestation. Ultrasonography in the first trimester may be performed either transabdominally or transvaginally. If a transabdominal examination is not definitive, a transvaginal or transperineal examination should be performed whenever possible. First-trimester ultrasonography is used to confirm the presence of an intrauterine pregnancy, estimate gestational age, diagnose and evaluate multiple gestations, confirm cardiac activity, and evaluate pelvic masses or uterine abnormalities (as an adjunct to chorionic villus sampling, embryo transfer, or localization and removal of intrauterine contraceptives). It is also useful for evaluating vaginal bleeding, suspected ectopic pregnancy, and pelvic pain.
An ultrasound examination may be targeted to help diagnose chromosomal abnormalities in the first trimester. One such examination is measurement of nuchal translucency (NT), the lucent area behind the head in the nuchal region. Use of standardized techniques for measuring NT has resulted in higher detection rates for Down syndrome, trisomy 18, trisomy 13, Turner syndrome, and other anatomic abnormalities such as cardiac defects. Recent studies demonstrate improved detection of Down syndrome at lower false-positive rates when NT measurement is combined with biochemical markers (see Section “Screening Tests”).
Various types of ultrasound examinations performed during the second or third trimester can be categorized as “standard,” “limited,” or “specialized.” A standard examination is performed during the second or third trimester of pregnancy. It includes an evaluation of fetal presentation, amniotic fluid volume, cardiac activity, placental position, fetal biometry, and an anatomic survey. If technically feasible, the uterus and adnexa are also examined. A limited examination is performed when a specific question requires investigation. In an emergency, for example, a limited examination can be performed to evaluate heart activity in a bleeding patient. A detailed or targeted anatomic specialized examination is performed when an anomaly is suspected on the basis of history, biochemical abnormalities or clinical evaluation, or suspicious results from either the limited or standard ultrasound examination. Other specialized examinations might include fetal Doppler, biophysical profile (BPP), fetal echocardiography, or additional biometric studies.
Evaluation of placental and cervical abnormalities may be accomplished with ultrasonography. Placental abruption can be identified by ultrasonography in approximately half of all patients who present with bleeding and do not have placenta previa. Color-flow Doppler ultrasound assessment is used to identify placenta accreta. Transvaginal ultrasound examination most accurately can visualize the cervix and can also be employed to detect or rule out placenta previa as well as an abnormally shortened cervix, which has been correlated with an increased risk of preterm delivery when measured at 24 to 30 weeks of gestation.
SCREENING TESTS
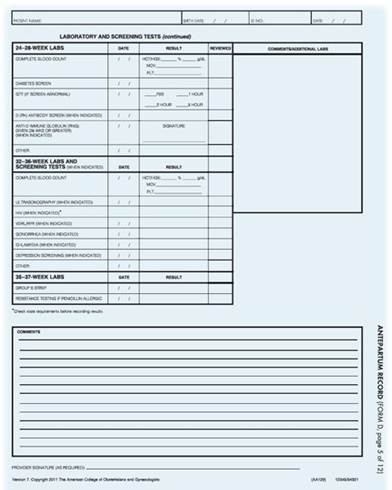
In addition to the routine laboratory tests performed at the initial antepartum visit, additional tests are performed at specific intervals throughout the pregnancy to screen for birth defects and other conditions. The specific tests and intervals for each are indicated on the Antepartum Record (see Appendix C). Additional laboratory testing, such as testing for STDs or tuberculosis, is recommended or offered on the basis of the patient’s history, physical examination, parental desire, or in response to public health guidelines.
There are several options for screening for fetal aneuploidy (abnormal number of chromosomes) such as trisomies 18 and 21 (see also Chapter 7 for a detailed discussion of each of these markers). Options for aneuploidy screening include the following:
• First-trimester screening (10–13 weeks’ gestation), which includes serum screening for pregnancy-associated plasma protein A (PAPP-A) and β-hCG and an ultrasound assessment of nuchal transparency.
• Second-trimester screening (15–20 weeks’ gestation) consisting of triple (maternal serum α-fetal protein [MSAFP], estriol, and hCG) or quadruple (“quad”) (MSAFP, hCG, estriol, and inhibin) screening tests.
• Integrated first- and second-trimester screening, which includes all of the first-trimester screening tests listed in addition to a PAPP-A test and a quad screen, with or without an ultrasound examination for NTDs, in the second trimester.
Additionally, third-trimester screening includes the glucose challenge test, a screening test performed for gestational diabetes between 24 and 28 weeks, unless the pregnant patient is obese or at high risk for developing diabetes. In these cases, the test should be performed at the first visit. If the test result is abnormal, a glucose tolerance test is performed to confirm diabetes. Universal screening for group B streptococcus is performed at 35 to 37 weeks of gestation, and treatment is based on culture results. In addition, the measurement of hemoglobin and hematocrit levels is repeated in the third trimester. Repeat screening in the third trimester for antibodies in Rh-negative patients and for HIV in all patients is commonly recommended and even required in some regions.
SPECIFIC TECHNIQUES OF FETAL ASSESSMENT
Continued evaluation of the fetus includes techniques for assessment of fetal 1) growth, 2) well-being, and 3) maturity. These tests must be interpreted in light of the clinical context and provide a basis for management decisions.
Assessment of Fetal Growth
Fetal growth can be assessed by fundal height measurement, as the initial measure, and ultrasonography. The increase in fundal height through pregnancy is predictable. If the fundal height measurement is significantly greater than expected (i.e., large for gestational age), possible considerations include incorrect assessment of gestational age, multiple pregnancy, macrosomia (large fetus), hydatidiform mole, and excess accumulation of amniotic fluid (polyhydramnios). A fundal height measurement less than expected, or small for gestational age, suggests the possibility of incorrect assessment of gestational age, hydatidiform mole, fetal growth restriction, inadequate amniotic fluid accumulation (oligohydramnios), or even intrauterine fetal demise. Deviation in fundal height measurement should be closely evaluated.
Ultrasound is the most valuable tool in assessing fetal growth and has many potential uses for both fetal dating and identifying fetal anomalies. In early pregnancy, determination of the gestational sac diameter and the crown-to-rump length correlates closely with gestational age. Later in pregnancy, measurement of the biparietal diameter of the skull, the abdominal circumference, the femur length, and the cerebellar diameter can be used to assess gestational age and, using various formulas, to estimate fetal weight.
Assessment of Fetal Well-Being
Assessment of fetal well-being includes subjective maternal perception of fetal activity and several objective tests using electronic fetal monitoring and ultrasonography. Tests of fetal well-being have a wide range of use, including the assessment of fetal status at a particular time and prediction of future well-being for varying time intervals, depending on the test and the clinical situation.
Evaluation of fetal activity is a common indirect measure of fetal well-being. Various methods can be used to quantify fetal activity, including the time necessary to achieve a certain number of movements each day, or counting the number of movements (“kick counts”) in a given hour. This type of testing is easily performed and involves the patient in her own care. If the mother notices less movement, further evaluation may be needed.
Fetal monitoring tests can provide more objective information about fetal well-being. These tests include the nonstress test (NST), contraction stress test (cST) (called the oxytocin challenge test [OCT] if oxytocin is used), Bpp, and ultrasonography of umbilical artery blood flow velocity. Although there is no optimal time to initiate fetal testing, there are several maternal- and pregnancy-related indications (Box 6.1).
BOX 6.1 Indications for fetal Testing
Maternal conditions
• Antiphospholipid syndrome
• Cyanotic heart disease
• Systemic lupus erythematosus
• Chronic renal disease
• Insulin-treated diabetes mellitus
• Hypertensive disorders
Pregnancy-Related or Fetal conditions
• Pregnancy-induced hypertension
• Decreased fetal movement
• Oligohydramnios and polyhydramnios
• Intrauterine growth restriction
• Postterm pregnancy
• Isoimmunization (moderate to severe)
• Previous fetal demise (unexplained)
• Multiple gestation (with significant growth discrepancy)
• Monochorionic diamniotic multiple gestation
From the American College of Obstetricians and Gynecologists. Guidelines for Perinatal Care. 7th ed. Washington, DC: American College of Obstetricians and Gynecologists; 2012:144–145.
Nonstress Test
The NST measures the fetal heart rate, patterns, and accelerations, which are monitored with an external transducer for at least 20 minutes. The patient may also be asked to note fetal movement, usually accomplished by pressing a button on the fetal monitor, which causes a notation on the monitor strip. The tracing is observed for fetal heart rate accelerations (Fig. 6.2). The results are considered reactive (or reassuring) if two or more fetal heart rate accelerations (peaking 15 beats above the baseline and lasting for 15 seconds) occur in a 20-minute period, with or without fetal movement discernible by the mother. A nonreactive (nonreassuring) tracing is one without sufficient heart rate accelerations in a 40-minute period. A nonreactive NST should be followed with further fetal assessment.
Contraction Stress Test
Whereas the NST evaluates the fetal heart rate response to fetal activity, the CST measures the response of the fetal heart rate to the stress of a uterine contraction. During a uterine contraction, uteroplacental blood flow is temporarily reduced by the contracting myometrium. A healthy fetus is able to compensate for this intermittent decreased blood flow, whereas a fetus that is compromised may be unable to do so. To perform a CST, a tocodynamometer is placed on the maternal abdomen along with a fetal heart rate transducer for a baseline tracing for 10 to 20 minutes. If there are no contractions, they are induced by nipple self-stimulation or oxytocin (this test is called an OCT). The result is negative if there is no change from the baseline fetal heart rate and no fetal heart rate decelerations. If decelerations occur, the results can be considered positive, equivocal, or unsatisfactory, depending on the pattern, frequency, and strength of the deceleration.
These tests of fetal well-being have a significant incidence of false-positive results (i.e., results suggesting that the fetus is in jeopardy, though the fetus is actually healthy). Because of this high incidence of false positives, the results of these tests must be interpreted collectively, and the tests themselves repeated to verify the results. When multiple test results are reassuring, they tend to rule out a problem. When all results are nonreassuring, they tend to signify the presence of a problem.
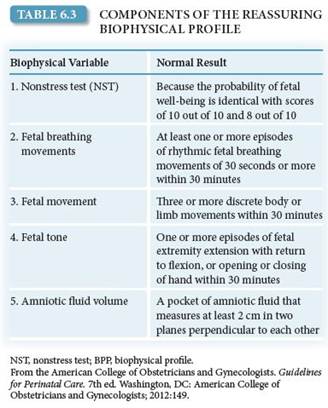
Biophysical profile
If an NST is nonreactive, evidence to support fetal well-being, such as that provided by a BPP, is sought. The BPP is a series of five assessments of fetal well-being, each of which is given a score of 0 (absent) or 2 (present), as shown in Table 6.3. The parameters include a reactive NST, the presence of fetal breathing movements, the presence of fetal movement of the body or limbs, the finding of fetal tone (flexed extremities as opposed to a flaccid posture), and an adequate amount of amniotic fluid volume. A total score of 8 to 10 is considered reassuring. A total score of 6 is equivocal and generally should lead to delivery if the patient is at term. If the patient is preterm, retesting within 12 to 24 hours may be appropriate. A score of 4 or less is nonreassuring and warrants further evaluation and consideration of delivery. Irrespective of the score, more frequent BPP testing or consideration of delivery may be warranted when oligohydramnios is present. Management based on the BPP depends not only on the score itself but also on the gestational age of the fetus.

FIGURE 6.2. Nonstress testing. (A) Reactive nonstress in response to fetal movement. (B) Nonreactive NST; response to fetal movement.
Modified BPP combines the use of an NST and assessment of an amniotic fluid index (AFI). The AFI is a semiquantitative, four-quadrant assessment of amniotic fluid depth. The importance of adequate amniotic fluid volume is well established. Diminished amniotic fluid is thought to represent decreased fetal urinary output caused by chronic stress and shunting of blood flow away from the kidneys. The decreased amniotic fluid provides less support for the umbilical cord, which may be more compressed, reducing blood flow. The modified BPP is less cumbersome than the BPP and appears to be as predictive of fetal well-being.
Doppler Ultrasound of Umbilical Artery
Umbilical artery Doppler flow ultrasonography is a noninvasive technique to assess resistance to blood flow in the placenta. It can be used in conjunction with other biophysical tests in high-risk pregnancies associated with suspected IUGR. Umbilical cord Doppler flow velocimetry is based on the characteristics of the systolic blood flow and the diastolic blood flow. The most commonly used index to quantify the flow velocity waveform is the systolic/diastolic ratio. As peripheral resistance increases, diastolic flow decreases and may become absent or reversed, and the systolic/diastolic ratio increases. Reversed end-systolic flow can be seen with severe cases of IUGR secondary to uteroplacental insufficiency and may suggest impending fetal demise.
BOX 6.2 Tests to Assess for fetal Maturity
Surfactant/albumin ratio (fetal lung maturity index)
Lecithin/sphingomyelin ratio Phosphatidylglycerol
Foam stability index
Fluorescence polarization
Optical density at 650 nm
Lamellar body counts
Saturated phosphatidylcholine
Assessment of Fetal maturity
Fetal maturity should always be taken into consideration when delivering a fetus preterm or electively in high-risk pregnancies. Several tests are available to assess fetal maturity (Box 6.2). Because the respiratory system is the last fetal system to mature functionally, many of the tests available to assess fetal maturity focus on this organ system. Several phospholipids, collectively known as surfactant, enter the amniotic fluid where they can be obtained by amniocentesis and measured. Surfactant is necessary for normal lung function to maintain the patency of the alveolar sacs. The ratio of two phospholipids, lecithin and sphingomyelin, called the L/S ratio, has been used to determine fetal lung maturity, but other tests are rapidly replacing the use of this ratio. Another important phospholipid contained in the surfactant complex is phosphatidylglycerol, a marker of complete pulmonary maturation that is present after 35 weeks of gestation.
Neonates delivered before their lungs have matured are at risk for respiratory distress syndrome (RDS), a serious and life-threatening condition caused by lack of surfactant. RDS in newborns is manifest by signs of respiratory failure— grunting, chest retractions, nasal flaring, and hypoxia— possibly leading to acidosis and death. Management consists of skillful support of ventilation and correction of associated metabolic disturbances until the neonate can ventilate without assistance. Administration of synthetic or semisynthetic surfactant to the neonate has resulted in improved outcomes for infants with RDS.
Results of pulmonary function tests that indicate immaturity do not have a high predictive value for RDS. Because no test indicating maturity can completely rule out the risk of RDS or other neonatal complications, the risk of adverse fetal outcome following delivery must be weighed against the potential risk of allowing the pregnancy to continue.
ANTEPARTUM PATIENT EDUCATION
Plans for the antepartum, intrapartum, and postpartum periods provide an opportunity for patient education and interaction. The Antepartum Record in Appendix C provides a list of the issues to be discussed during antepartum care.
Employment
A woman with an uncomplicated pregnancy can theoretically continue to work until the onset of labor. In a normal pregnancy, there are few restrictions concerning work, although it is beneficial to allow moderate activity and to allow for periods of rest. Strenuous work (prolonged standing or repetitive, strenuous, and physical lifting) is best avoided.
A period of 4 to 6 weeks generally is required for a woman’s physical condition to return to normal. However, the patient’s individual circumstances may be a factor in determining when she returns to work. The length of a woman’s leave from work can depend on whether there are pregnancy or delivery complications, the work involved, the employer attitude, the rules of the health care system under which the patient receives care, and the wishes of the patient. The federal Family and Medical Leave Act and state laws should be consulted to determine the family and medical leave that is available.
Exercise
In the absence of either medical or obstetric complications, up to 30 minutes of moderate exercise per day on most if not all days of the week is acceptable (Box 6.3). Each sport should be reviewed for its potential risk, and activities with a high risk of falling or of abdominal trauma should be avoided.
BOX 6.3 Contraindications to Aerobic Exercise during Pregnancy
Absolute
• Hemodynamically significant heart disease
• Restrictive lung disease
• Cervical insufficiency
• Multiple gestation at risk for premature labor
• Persistent second-trimester or third-trimester bleeding
• Placenta previa after 26 weeks of gestation
• Premature labor during the current pregnancy
• Ruptured membranes
• Preeclampsia/gestational hypertension
Relative
• Severe anemia
• Unevaluated maternal cardiac arrhythmia
• Chronic bronchitis
• Poorly controlled type 1 diabetes
• Extreme morbid obesity
• Extreme underweight (BMI < 12)
• History of extremely sedentary lifestyle
• Intrauterine growth restriction in current pregnancy
• Poorly controlled hypertension
• Orthopedic limitations
• Poorly controlled seizure disorder
• Poorly controlled hyperthyroidism
• Heavy smoker
From the American College of Obstetricians and Gynecologists. Exercise during pregnancy and the postpartum period. ACOG Committee Opinion No. 267. Washington, DC: American College of Obstetricians and Gynecologists; 2002;99(1):171–173.
Overly strenuous exercise, especially for prolonged periods, should be avoided. Patients unaccustomed to regular exercise should not undertake vigorous new programs during pregnancy. Supine exercises should be discontinued after the first trimester to minimize circulatory changes brought on by pressure of the uterus on the vena cava. Any activity should be discontinued if discomfort, significant shortness of breath, or pain in the chest or abdomen appears (Box 6.4). Changes in body contour and balance will alter the advised types of activities; abdominal trauma should be avoided.
Sitting in a hot tub or sauna after exercise is not recommended for pregnant women. Hyperthermia may be teratogenic, particularly in the first trimester. Pregnant women might reasonably be advised to remain in saunas for no more than 15 minutes and in hot tubs for no more than 10 minutes. In a hot tub, if a woman’s head, arms, shoulders, and upper chest are not submerged, there is less surface area to absorb heat.
Nutrition and Weight Gain
Concerns about adequate nutrition and weight gain during pregnancy are common. Poor nutrition, obesity, and food faddism are associated with poor perinatal outcome. Pica, or an inclination for nonnutritional substances such as ice, food starch, clay, and dirt, is often associated with anemia.
A complete nutritional assessment is an important part of the initial antepartum assessment, including history of dietary habits, special dietary issues or concerns, and weight trends. Anorexia and bulimia increase the risks of associated problems such as cardiac arrhythmias, gastrointestinal (GI) pathology, and electrolyte disturbances. Calculation of BMI is useful because it relates weight to height, allowing for a better indirect measurement of body fat distribution than is obtained with weight alone. Further, because of the “personalized nature” of an individual’s BMI, it is often more useful in teaching a patient about diet and weight issues than an abstract table.
BOX 6.4 Warning Signs to Terminate Exercise While Pregnant
Vaginal bleeding
Dyspnea prior to exertion
Dizziness
Headache
Chest pain
Muscle weakness
Calf pain or swelling (need to rule out thrombophlebitis)
Preterm labor
Decreased fetal movement Amniotic fluid leakage
From the American College of Obstetricians and Gynecologists. Exercise during pregnancy and the postpartum period. ACOG Committee Opinion No. 267. Washington, DC: American College of Obstetricians and Gynecologists; 2002;99(1):171–173.
Recommendations for total weight gain during pregnancy and the rate of weight gain per month appropriate to achieve it may be made based on a BMI calculated for the prepregnancy weight. Pregnant women in their early teens who may still be growing should consider total weight gain in the upper end of these ranges to optimize fetal growth as well. The components that make up the average weight gain in a normal singleton pregnancy are listed in Table 6.4. The maternal component of this weight gain starts in the first trimester and increases linearly after the second trimester. Fetal growth is most rapid in the second half of pregnancy, with the normal fetus tripling its weight in the last 12 weeks.
Published recommended daily allowances (RDAs) for protein, minerals, and vitamins are useful approximations. It should be kept in mind, however, that the RDAs are a combination of estimates and values adjusted near the top of the normal ranges to encompass the estimated needs of most women. Thus, many women have an adequate diet for their individual needs, even though it does not supply all the RDAs. Vitamin supplementation is appropriate for specific therapeutic indications, such as a patient’s inability or unwillingness to eat a balanced, adequate diet, or clinical demonstration of a specific nutritional risk. Except for iron, mineral supplementation is likewise not required in otherwise healthy women. The National Academy of Science recommends 27 mg of iron supplementation.

Financial problems, the inability to get to a grocery store, and foodstuffs unique to a patient’s social group that differ in substantial quantitative ways with respect to important nutrients may prevent some women from obtaining adequate nutrition, even if the volume of foodstuffs seems sufficient. The Women, Infants and Children Federal Supplemental Food Program, Food Stamp Programs, and Aid for Families with Dependent Children are resources that may help in these situations.
Breastfeeding
The benefits of breastfeeding include, for the newborn, excellent nutrition and provision of immunologic protection, and, for the mother, more rapid uterine involution, economy, maternal–child bonding, natural contraception (to some extent), and more rapid weight loss associated with extra caloric expenditure (for some women). Contraindications to breastfeeding include certain maternal infections and use of medications. It is important to support a woman who chooses not to breastfeed. The use of breast pumps and milk storage may allow a mother to continue breastfeeding while continuing to work.
Sexual Activity
Sexual intercourse is not restricted during a normal pregnancy, although advice about more comfortable positions in later pregnancy may be appreciated—for example, sideto-side or the female superior position. Sexual activity may be restricted or prohibited under certain high-risk circumstances, such as known placenta previa, premature rupture of membranes, or history of or current preterm labor (or delivery). Education of the patient (and partner) about safe sex practices is as important in antepartum care as in regular gynecologic care.
Travel
Most airlines allow pregnant women to fly up to 36 weeks. Air travel is not recommended for women who have medical or obstetric complications, such as hypertension, poorly controlled diabetes mellitus, or sickle cell disease. This recommendation is not due to substantial risk to either mother or fetus but because of the likelihood that labor may ensue away from home and customary health care providers. If a long trip near term is planned, it is useful for the patient to carry a copy of her obstetric record in case she requires obstetric care. When traveling, patients are advised to avoid long periods of inactivity such as sitting. Walking every 1 to 2 hours, even for short periods, promotes circulation, especially in the lower legs, and decreases the risk of venous stasis and possible thromboembolism. Additionally, preventive antiemetic medicine should be considered for pregnant women with increased nausea. Education about the regular use of a seat belt is especially important, with the seat belt worn low on the hip bones, between the protuberant abdomen and the pelvis.
Teratogens
Many patient inquiries concern the teratogenic potential of environmental exposures. Major birth defects are apparent at birth in 2% to 3% of the general population. The possible occurrence of fetal malformations or mental retardation is a frequent cause of anxiety among pregnant women. Of these, about 5% may be a result of maternal exposure to drugs or environmental chemicals, and only approximately 1% can be attributed to pharmaceutical agents. The most important determinants of the developmental toxicity of an agent are timing, dose, and fetal susceptibility. Many agents have teratogenic effects only if taken while the susceptible fetal organ system is forming.
The health care provider may wish to consult with or refer at-risk patients to health care professionals with special knowledge or experience in teratology and birth defects. The Organization of Teratology Information Services provides information on teratology issues and exposures in pregnancy (www.otispregnancy.org).
Medications
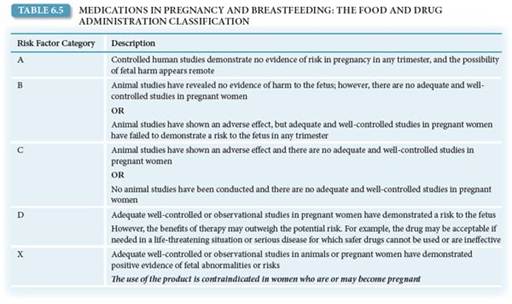
Very few medications have been proven to be true human teratogens (Box 6.5). Most commonly prescribed medications are relatively safe in pregnancy. The Food and Drug Administration assigns medications a pregnancy risk factor based on information about the medication and its risk/benefit ratio. These pregnancy risk factors help guide the appropriate use of medications in pregnancy (Table 6.5). Table 6.6 provides a summary of the teratogenicity of many common medications. Little data exist about the safety of traditional or folk
BOX 6.5 Drugs or Substances Suspected or Proven to Be human Teratogens
ACE inhibitorsa
Aminopterin
Androgens
Ang-II antagonistsb
Busulfan
Carbamazepine
Chlorobiphenyls
Cocaine
Coumarins
Cyclophosphamide
Danazol
Diethylstilbestrol
Ethanol
Etretinate
Kanamycin
Lithium
Methimazole
Methotrexate
Misoprostol
Penicillamine
Phenytoin
Radioactive iodine
Streptomycin
Tamoxifen
Tetracycline
Thalidomide
Tretinoin
Trimethadione
Valproic acid
Isotretinoin
aAngiotensin–converting enzyme inhibitors.
bAngiotensin II receptor antagonists.
Adapted from Briggs GG, Freeman RK, Yaffe SJ. Drugs in Pregnancy and Lactation: A Reference Guide to Fetal and Neonatal Risk. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins 2008.
From Cunningham GF, Leveno KJ, Bloom SL, Hauth JC, Gilstrap LC, Wenstom KD, eds. Williams Obstetrics. 22nd ed. New York, NY: McGraw Hill Professional; 2005:T14-1.
Ionizing Radiation
Ionizing radiation exposure is universal; most radiation originates from beyond the earth’s atmosphere, from the land, and from endogenous radionuclides. The total radiation exposure from these sources is approximately 125 mrad/y. Although radiation exposure has the potential to cause gene mutations, growth impairment, chromosome damage and malignancy, and fetal death, large doses are required to produce discernible fetal effects. Large doses (10 rad) during the first 2 weeks after fertilization are required to produce a deleterious effect. In the first trimester, 25 rad is required to produce detectable damage, and 100 rad is required later in pregnancy. Diagnostic radiation usually exposes the fetus to much less than 5 rad, depending on the number of radiographs taken and the maternal site examined (Table 6.7). Exposure to less than 5 rad has not been associated with an increase in fetal anomalies or pregnancy loss; therefore, it is recommended to limit accumulated fetal exposure to less than 5 rad during pregnancy.
Methyl Mercury
Industrial pollution is the major source of mercury entry in our ecosystem. Large fish, such as tuna, shark, and king mackerel, retain higher levels of mercury from the smaller fish and organisms they consume. Therefore, women who eat these fish are storing high levels of mercury.
Pregnant women should be encouraged to enjoy a variety of fish, including up to 12 ounces (two average meals) a week of fish and shellfish that are lower in mercury. Five of the most common fish low in mercury are shrimp, canned light tuna, salmon, pollock, and catfish. White (albacore) tuna has more mercury and should be limited to no more than 6 ounces per week.
Herbal Remedies
Herbal remedies are not regulated as prescription or OTC drugs, the identity and quantity of their ingredients are unknown, and there are virtually no studies of their teratogenic potential. Because it is not possible to assess their safety, pregnant women should be counseled to consider avoiding these substances. Remedies containing substances with pharmaceutical properties that could theoretically have adverse fetal affects include the following:
• Echinacea—causes fragmentation of hamster sperm at high concentrations
• Black cohosh—contains a chemical that acts like an estrogen
• Garlic and willow barks—have anticoagulant properties
• Ginkgo—can interfere with effects of monamine oxidase inhibitors; has anticoagulant effects
• Real licorice—has hypertensive and potassium-wasting effects
• Valerian—intensifies the effects of prescription sleep aids
• Ginseng—interferes with the effects of monamine oxidase inhibitors
• Blue cohosh and pennyroyal—stimulate uterine musculature; pennyroyal can also cause liver damage, renal failure, disseminated intravascular coagulation, and maternal death


Alcohol
Alcohol is the most common teratogen to which a fetus is exposed, and alcohol consumption during pregnancy is a leading preventable cause of mental retardation, developmental delay, and birth defects in the fetus. There is substantial evidence that fetal toxicity is dose related and that the exposure time of greatest risk is the first trimester. There is no established safe level of alcohol use during pregnancy. Women who are pregnant or who are at risk for pregnancy should not drink alcohol. Although consumption of small amounts of alcohol early in pregnancy is unlikely to cause serious fetal problems, patients are best advised to refrain from alcohol entirely.
Fetal alcohol syndrome (FAS) is a congenital syndrome characterized by alcohol use during pregnancy and includes three findings:
1. Growth restriction (which may occur in the prenatal period, the postnatal period, or both)
2. Facial abnormalities, including shortened palpebral fissures, low-set ears, midfacial hypoplasia, a smooth philtrum, and a thin upper lip
3. Central nervous system dysfunction including microcephaly, mental retardation, and behavioral disorders such as attention deficit disorder
The exact risk incurred by maternal alcohol use is difficult to establish, because the complex pattern of symptoms associated with FAS can make diagnosis difficult. Consumption of eight or more drinks daily throughout pregnancy confers a 30% to 50% risk of having a child with FAS. However, even low levels of alcohol consumption (two or fewer drinks per week) have been associated with increased aggressive behavior in children.
Tobacco Use
The risks of smoking during pregnancy have been well established and include risks to the fetus such as IUGR, low birthweight, and fetal mortality. It is important for the obstetrician to take advantage of the prenatal visits to educate patients about the risks of smoking for both themselves and their newborns and to coordinate appropriate resources to help patients quit. Counseling programs are available to help patients quit smoking. Nicotine replacement products may be considered, although their safety in pregnancy has not been documented.

Substance Abuse
The use of illicit substances by women of childbearing age has led to an increased number of neonates having had in utero exposure and subsequent risk of adverse effects from a variety of drugs. Fetal drug exposure is often unrecognized because of the lack of overt symptoms or structural anomaly following birth.
Illicit drugs may reach the fetus via placental transfer or may reach the newborn through breast milk. The specific effect on the fetus and newborn varies with the respective substances. An opiate-exposed fetus may experience withdrawal symptoms in utero if the woman stops; when the woman herself goes through withdrawal, either voluntarily or under supervision; or after birth when opiate delivery by way of the placenta ceases.
Universal screening, using biologic specimens, of women and newborns for substance abuse is not recommended. However, all pregnant women should be asked at their first prenatal visit about past and present use of alcohol; nicotine; and other drugs, including recreational use of prescription and OTC medications. Use of specific screening questionnaires may improve detection rates. A woman who acknowledges the use of these substances should be counseled about the perinatal implications of their use during pregnancy and offered referral to an appropriate drug treatment program if chemical dependence is suspected. Careful follow-up during the postpartum period is also recommended.
 COMMON SYMPTOMS
COMMON SYMPTOMS
The normal physiology of pregnancy often results in symptoms that would be considered pathologic were the patient not pregnant. All health care providers caring for pregnant patients should be familiar with what changes are considered normal in pregnancy and be able to educate the patient in that regard.
Headaches
Headaches are common in early pregnancy and may be severe. The etiology of such headaches is not known. Treatment with acetaminophen in usual doses is recommended and is generally adequate. A persistent headache unrelieved by acetaminophen should be further evaluated.
Edema
The presence of significant edema in the lower extremities (dependent edema) and/or hands is very common in pregnancy and, by itself, is not abnormal. Fluid retention can be associated with hypertension, however, so that blood pressure as well as weight gain and edema must be evaluated in a clinical context before the findings are presumed to be innocuous.
Nausea and Vomiting
The majority of pregnant women experience some degree of upper GI symptoms in the first trimester of pregnancy. Classically, these symptoms are worse in the morning (the so-called morning sickness). However, patients may experience symptoms at other times or even throughout the day. Most mild cases of nausea and vomiting can be resolved with lifestyle and dietary changes, including consuming more protein, ginger, vitamin B6, or vitamin B6 with doxylamine. Usually, nausea and vomiting improve significantly by the end of the first trimester. Effective and safe treatments for more serious cases include antihistamine H1-receptor blockers and phenothiazines. The most severe form of pregnancy-associated nausea and vomiting is hyperemesis gravidum, which occurs in less than 2% of pregnancies. This condition may require hospitalization, with fluid and electrolyte therapy and medications.
Heartburn
Heartburn (gastric reflux) is common, especially postprandially, and is often associated with eating large meals or spicy or fatty foods. Patient education about smaller and more frequent meals and blander foods, combined with not eating immediately before retiring, is helpful. Antacids may be helpful when used judiciously in pregnancy.
Constipation
Constipation is physiologic in pregnancy, associated with increased transit time; increased water absorption; and, often, decreased bulk. Dietary modifications, including increased fluid intake and increased bulk with such foods as fruits and vegetables, are usually helpful. Other useful interventions may include the use of surface-active bowel softeners such as docusate, supplemental dietary fibers such as psyllium hydrophilic mucilloid, and lubricants.
Fatigue
In early pregnancy, patients often complain of extreme fatigue that is unrelieved by rest. There is no specific treatment, other than adjustment of the woman’s schedule to the extent possible to accommodate this temporary lack of energy. Patients can be reassured that the symptoms disappear in the second trimester.
Leg Cramps
Leg cramps, usually affecting the calves, are common during pregnancy. A variety of treatments, including oral calcium supplement, potassium supplement, and tonic water, have been proposed over the years, none of which are universally successful. Massage and rest are often advised.
Back Pain
Lower back pain is common, especially in late pregnancy. The altered center of gravity caused by the growing fetus places unusual stress on the lower spine and associated muscles and ligaments. Treatment focuses on heat, massage, and limited use of analgesia. A specially fitted maternal girdle may also help, as will not wearing shoes with high heels.
Round Ligament Pain
Sharp groin pain, especially as pregnancy advances, is common, often quite uncomfortable, and disturbing to patients. This pain is often more pronounced on the right side because of the usual dextrorotation of the gravid uterus. The woman should be reassured that the pain represents stretching and spasm of the round ligaments. Modification of activity, especially more gradual movement, is often helpful; analgesics are rarely indicated.
Varicose Veins and Hemorrhoids
Varicose veins are not caused by pregnancy but often first appear during the course of gestation. Besides the disturbing appearance to many patients, varicose veins can cause an aching sensation, especially when patients stand for long periods of time. Support hose can help diminish the discomfort, although it has no effect on the appearance of the varicose veins. Popular brands of support hose do not provide the relief that prescription elastic hose can. Hemorrhoids are varicosities of the hemorrhoidal veins. Treatment consists of sitz baths and local preparations. Varicose veins and hemorrhoids regress postpartum, although neither condition may abate completely. Surgical correction of varicose veins or hemorrhoids should not be undertaken for approximately the first 6 months postpartum to allow for the natural involution to occur.
Vaginal Discharge
The hormonal milieu of pregnancy often causes an increase in normal vaginal secretions. These normal secretions must be distinguished from infections, such as vaginitis, which has symptoms of itching and malodor, and bacterial vaginosis, which has been linked to preterm labor. Spontaneous rupture of membranes, which is characterized by leakage of thin, clear fluid, is another possible cause that must be considered.
Clinical Follow-Up
The patient is 8 weeks pregnant based on your bedside vaginal sonogram. You perform a thorough history and physical examination, obtaining the appropriate prenatal screening blood work and cervico-vaginal cultures. You discuss available screening for genetic conditions, including fetal chromosome abnormalities, as well as screening for immunity to more common infectious diseases. The patient is educated on the importance of regular prenatal care, appropriate exercise, nutrition, and weight gain, and how to manage common complaints in pregnancy.
thePoint Visit http://thePoint.lww.com/activate for an interactive USMLE-style question bank and more!