Chapter 4 Embryology and Anatomy
Students should be able to describe basic development of the early human embryo, particularly as it relates to reproductive anatomy. They should be able to describe normal prepubertal, reproductive, and menopausal anatomy of the reproductive tract.
Clinical Case
You are performing a total abdominal hysterectomy and bilateral salpingo-oophorectomy upon a patient with a diagnosis of severe endometriosis and chronic disabling pelvic pain that inhibits a normal professional or personal lifestyle and is unresponsive to nonnarcotic analgesia. You have found dense pelvic adhesions, especially in the areas of the posterior cul-de-sac, disrupting normal anatomic relationships. Your dissection has proceeded through the utero-ovarian ligaments and is now approaching the level of the cervical os. You are concerned about inadvertent damage to the ureter because of the difficulty in dissection of the dense adhesions as well as the possibility of alteration of the normal anatomic relationships, especially that of the ureter. Supracervical hysterectomy is not an option because the patient has had severe cervical dysplasia and cervical conization. A preoperative discussion about the possible need for supracervical hysterectomy in the event of dense adhesions had also revealed the patient’s firm desire for removal of the cervix due to the stress involved in her past workup for dysplasia, its treatment, and current follow-up.
An understanding of reproductive anatomy and its developmental precursors is important for learners in their ability to apply basic diagnostic and therapeutic principles in patient care.
Knowledge of the embryology and anatomy of the female genital system is helpful in understanding both normal anatomy and the congenital anomalies that occur. Embryology may be useful in many areas of gynecologic and obstetric practice. For example, in gynecologic oncology, embryology can assist clinicians in predicting the growth and routes of spread of gynecologic cancers; in urogynecology and pelvic reconstructive surgery, it can enhance a surgeon’s comprehension of the components of pelvic support and possible defects.
It can also play a key role in understanding and diagnosing various aspects of sexual dysfunction.Note: Throughout this chapter, “weeks of gestation” and “weeks of development” are used to describe embryologic events. Weeks of gestation is generally based on last menstrual period, whereas weeks of development connote postfertilization age. Clarification and consistency here are important.
 EMBRYOLOGY
EMBRYOLOGY
The ovaries, fallopian tubes, uterus, and upper portion of the vagina are derived from the intermediate mesoderm, whereas the external genitalia develop from genital swellings in the pelvic region. Beginning in the fourth week (postfertilization) of development, the intermediate mesoderm forms the urogenital ridges along the posterior body wall. As their name implies, these ridges contribute to the formation of the urinary and genital systems (Fig. 4.1).
The gonads, genital ducts, and external genitalia all pass through an indifferent (undifferentiated) stage in which it is not possible to determine sex based on the appearance of these structures. The genetic sex of an embryo is determined by the sex chromosome (X or Y) carried by the sperm that fertilizes the oocyte. The Y chromosome contains a gene called SRY (sex-determining region on Y) that encodes a protein called testis-determining factor. When this protein is present, the embryo develops male sex characteristics. The ovary-determining gene is WNT4; when this gene is present and SRY is absent, the embryo develops female characteristics. Gonads become structurally male or female by the 7th week of development, and external genitalia become differentiated by the 12th week. The influence of androgens is crucial in the normal development of the external genitalia. Any condition that increases the level of androgen production in a female embryo will cause developmental anomalies. For example, the genetic disease congenital adrenal hyperplasia (CAH) causes a decreased production of cortisol that results in a compensatory increase in androgens.
The genitalia of female fetuses with CAH are ambiguous, that is, neither normal female nor normal male.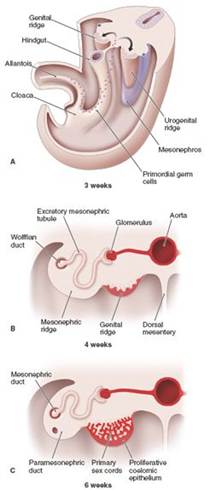
FIGURE 4.1. Early development of the urogenital system. (A) Beginning at approximately 3 weeks of gestation, urogenital ridges arise along the posterior wall of the coelomic cavity. Primordial germ cells migrate across the allantois into the genital ridges. (B) and (C) These transverse sections through the lumbar region of the human embryo show development of the indifferent gonad from the genital ridges at 4 and 6 weeks of gestation. (Modified from Sadler TW. Langman’s Medical Embryology. 10th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2006:240–241.)
Development of the Ovary
Ovaries are homologous to the testes in the male. Both types of gonads begin development as gonadal or genital ridges that form during the fifth week of gestation (not to be confused with weeks of development) from the urogenital ridges. Fingerlike bands of epithelial cells project from the surface of the gonad into each gonadal ridge, forming irregularly shaped primary sex cords. Growth of these cords into the gonadal ridge results in the creation of an outer cortex and an inner medulla in the indifferent gonad.
Primordial germ cells that give rise to gametes appear in the wall of the yolk sac (now called the umbilical vesicle) during the third week of development (see Fig. 4.1). From this location, primordial germ cells migrate along the allantois in the connecting stalk to the dorsal mesentery of the hindgut and then into the gonadal ridges, where they become associated with the primary sex cords by the sixth week. In the female, the primordial germ cells become oogonia, which divide by mitosis during fetal life; no oogonia are formed after birth. If the primordial germ cells fail to migrate to the genital ridges, the ovary does not develop.
By approximately the 10th week of development, the undifferentiated gonad has developed into an identifiable ovary.
Primary sex cords degenerate, and secondary sex cords or cortical cords appear. These cords extend from the surface epithelium into the underlying mesenchyme (Fig. 4.2, right column of figure). By approximately 16 weeks of gestation, cortical cords in the ovary organize into primordial follicles. Each follicle eventually consists of an oogonium, derived from a primary germ cell, surrounded by a single layer of squamous follicular cells, derived from the cortical cords. Follicular maturation begins when the oogonia enter the first stage of meiotic division (at which point they are called primary oocytes). Oocyte development is then arrested until puberty, when one or more follicles are stimulated to continue development each month (see Chapter 38).In male embryos, the primary sex cords do not degenerate; instead, they develop into seminiferous (or testis) cords that eventually give rise to the rete testis and seminiferous tubules (see Fig. 4.2, left column of figure). A layer of dense connective tissue (the tunica albuginea) separates the seminiferous cords from the surface epithelium, which eventually becomes the testis. Cortical cords do not form in the male embryo.
As they develop, gonads descend from their starting point high up in the primitive body cavity, where they are attached to a mesenchymal condensation called the gubernaculum. Ovaries move caudally to a location just below the rim of the true pelvis immediately adjacent to the fimbriated end of the fallopian tubes. The testis, on the other hand, continues to descend, eventually migrating through the anterior abdominal wall just superior to the inguinal ligament. The gubernaculum in the female fetus eventually forms the ovarian and round ligaments (see Figs. 4.2 and 4.3).
alt=image>


FIGURE 4.2. Development of the gonads and their migration to their adult locations.
At approximately 6 weeks of gestation, the gonads have differentiated into either male or female (A and B). In female embryos, the paramesonephric ducts develop into the uterus, uterine tubes, and parts of the vagina (C and D). In male embryos, the mesonephric ducts develop into the main genital tracts (ductus deferens) (E and F). (Modified from Sadler TW. Langman’s Medical Embryology. 10th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2006:243, 245.)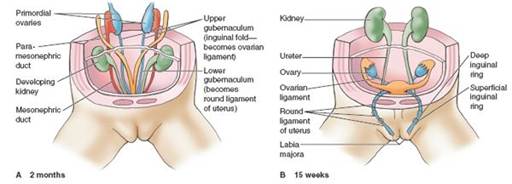

Anterior views
FIGURE 4.3. Route of the migrating gonads in a female fetus. (A) At 2 months, the early gonads are located high up in the coelomic cavity attached to the gubernaculum. (B) The gubernaculum migrates through the anterior abdominal wall just above the inguinal ligament; this process also takes place in the male embryo. (C) The ovaries arrest their descent in the ovarian fossa, immediately subjacent to the uterus on either side. (From Moore KL, Dalley AF. Clinically Oriented Anatomy. 5th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2006: Fig. 2.14.)
Development of the Genital Ducts
In both male and female embryos, two pairs of ducts develop—the mesonephric (wolffian) and paramesonephric (Müllerian) ducts. As with the gonad, these ducts pass through an indifferent stage in which both pairs of ducts are present in both the male and the female embryo. Differentiation of the female ductal system is not dependent on development of the ovaries (Fig. 4.4).
In the male embryo, the mesonephric ducts, which drain the embryonic mesonephric kidneys, eventually form the epididymis, ductus deferens, and ejaculatory ducts. In the female embryo, the mesonephric ducts disappear. The paramesonephric ducts persist to form major parts of the female reproductive tract (the fallopian tubes, uterus, and upper portion of the vagina).
Paramesonephric ducts begin as invaginations of the epithelium covering the urogenital ridges, eventually forming longitudinally oriented tubes. The cranial end of each duct opens into the body (future peritoneal) cavity. The ducts grow caudally until the two caudal ends contact the posterior wall of the urogenital sinus. This contact induces the posterior wall to proliferate and form the vaginal plate that eventually gives rise to the lower portion of the vagina. Meanwhile, the lower ends of the paramesonephric ducts fuse to form the upper portion of the vagina, cervix, and uterus. The cranial portion of each duct remains separated and forms the fallopian tube on each side. As the ducts move toward fusion in the midline, they carry a fold of peritoneum with them that becomes the broad ligament.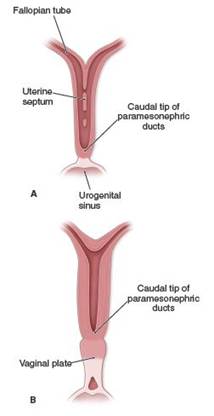

FIGURE 4.4. Development of the internal reproductive organs from the Müllerian ducts in the female embryo. (A) Initially, the ducts are separate structures that begin to fuse lengthwise at their caudal ends. (B) This fusion creates the lumen of the uterus. Simultaneously, the vagina develops where the urogenital sinus meets the Müllerian ducts, the vaginal plate. (C) Eventually, the uterus, cervix, and vagina are formed. (Modified from Sadler TW. Langman’s Medical Embryology. 10th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2006:246.)
Development of the External Genitalia
The cloaca is formed from a dilatation of the caudal end of the hindgut and is covered exteriorly by the cloacal membrane. Eventually, the cloaca is separated into the urogenital sinus anteriorly and the anorectal canal posteriorly by the urorectal septum. This septum forms from a collection of mesoderm in the pelvic floor that grows downward during the fifth to the eighth weeks of gestation to reach the cloacal membrane. At the same time, the genital tubercle develops at the cranial end of the cloacal membrane, while labioscrotal swellings and urogenital folds appear on each side (Fig. 4.5A). The genital tubercle enlarges in both the male and the female (Fig. 4.5B). In the presence of estrogens and the absence of androgens, external genitalia are feminized. The genital tubercle develops into the clitoris (Fig. 4.5C). The unfused urogenital folds form the labia minora, and the labioscrotal swellings become the labia majora (Fig. 4.5D). At approximately 15 weeks of gestation, transabdominal ultrasonography can often distinguish between the two sexes.
ANATOMY
Bony Pelvis
The bony pelvis is composed of the paired innominate bones and the sacrum. The innominate bones are joined anteriorly to form the symphysis pubis, and each is articulated posteriorly with the sacrum through the sacroiliac joint (Fig. 4.6). The sacrum is composed of five or six sacral vertebrae, which are fused in adulthood. The sacrum articulates with the coccyx inferiorly and with the fifth lumbar vertebra superiorly.
The pelvis is divided into the greater pelvis (false pelvis) and the lesser pelvis (true pelvis), which are separated by the linea terminalis. The greater pelvis distributes the weight of the abdominal organs and supports the pregnant uterus at term. The greater pelvis is bounded by the lumbar vertebrae posteriorly, an iliac fossa bilaterally, and the abdominal wall anteriorly. The true pelvis contains the pelvic viscera, including the uterus, vagina, bladder, fallopian tubes, ovaries, and the distal rectum and anus. It is formed by the sacrum and coccyx posteriorly and by the ischium and pubis laterally and anteriorly.
In obstetrics, it is important to assess the size of the pelvis to determine whether it is of adequate capacity for vaginal birth. This evaluation is based on the diameters of the pelvic outlet, pelvic inlet, and midpelvis. Measurement of these diameters is called pelvimetry and can be made radiographically, with computed tomography (the most accurate method), or during a pelvic examination. One of the most important measurements is that of the obstetric conjugate (Fig. 4.7), which is the narrowest fixed distance through which the fetal head must pass during a vaginal delivery. The obstetric conjugate cannot be measured directly due to the presence of the bladder.
The obstetric conjugate is calculated indirectly by measuring the diagonal conjugate, which is the distance between the lower border of the pubis anteriorly to the lower sacrum at the level of the ischial spines. The obstetric conjugate is 1.5 to 2 cm shorter. In general, it should be 11.0 cm or greater to accommodate a fetal head of normal size. Other measurements include the interspinous diameter (the distance between the ischial spines) and transverse diameter (the distance measured at the greatest width of the s uperior aperture).
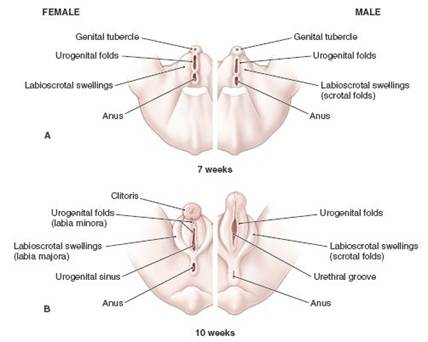

FIGURE 4.5. Comparison of the development of male and female external genitalia. (A) Early in gestation, the genital tubercle develops along with labioscrotal swellings and urogenital folds. (B) Shortly thereafter, the genital tubercle enlarges in both the male and female fetus. (C) The posterior commissure forms, effectively dividing genitals from anus. (D) Without the influence of a Y chromosome, the phallus regresses in relative size to form the clitoris.
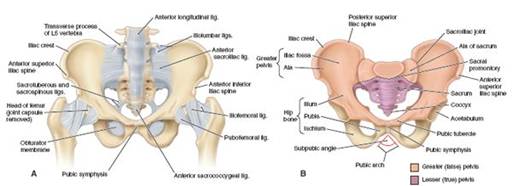
FIGURE 4.6. The bony pelvis. (A) Anterior view of the pelvis; the greater and lesser pelves are color-coded. (B) The pelvic ligaments are shown in detail. (From Moore KL, Dalley AF. Clinically Oriented Anatomy. 5th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2006:Figs. 3.3B and 3.2A.)

FIGURE 4.7. Pelvic diameters and estimating the obstetric conjugate. (A) Superior view of the pelvis showing the diameters that are measured in pelvimetry. (B) Medial view of the pelvis demonstrating the diagonal conjugate and the obstetric conjugate. (C) Measurement of the obstetric conjugate. The examiner palpates the sacral promontory with the tip of the middle finger. The distance between the tip of the index finger, which is 1.5 cm shorter than the middle finger, and the place on the hand where the pubic symphysis is felt is measured to yield the obstetric conjugate, which should be at least 11 cm. (From Moore KL, Dalley AF. Clinically Oriented Anatomy. 5th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2006:Fig. B3.2.)
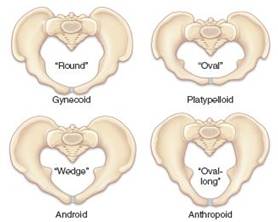
FIGURE 4.8. Caldwell-Moloy pelvic types.
The female pelvis may be classified into four basic types, according to the scheme of Caldwell and Moloy (Fig. 4.8), although an individual may have a pelvis that is a mixture of types. The most common type is the gynecoid pelvis, occurring in approximately 40% to 50% of women. In general, this pelvic shape is cylindrical and has adequate space along its length and breadth. The anthropoid type occurs in approximately 25% of all women, and the android pelvis occurs in approximately 20%. The platypelloid pelvis occurs in only 2% to 5% of women.
Vulva and Perineum
The perineum comprises the area of the surface of the trunk between the thighs and the buttocks, extending from the coccyx to the pubis. Anatomists also use the term “perineum” to refer to the shallow compartment that lies deep to this area and inferior to the pelvic diaphragm.
The vulva contains the labia majora, labia minora, mons pubis, clitoris, vestibule, and ducts of glands that open into the vestibule (Fig. 4.9). The labia majora are folds of skin with underlying adipose tissue, fused anteriorly with the mons pubis and posteriorly at the perineum. The skin of the labia majora contains hair follicles as well as sebaceous and sweat glands. The labia minora are narrow skin folds lying inside the labia majora. The labia minora merge anteriorly with the prepuce and frenulum of the clitoris and posteriorly with the labia majora and the perineum. The labia minora contain sebaceous and sweat glands but no hair follicles, and there is no underlying adipose tissue. The clitoris, which is located anterior to the labia minora, is the embryologic homologue of the penis. It consists of two crura (corresponding to the corpora cavernosa in the male) and the glans, which is found superior to the point of fusion of the crura. On the ventral surface of the glans is the frenulum, the fused junction of the labia minora. The vestibule lies between the labia minora and is bounded anteriorly by the clitoris and posteriorly by the perineum. The urethra and the vagina open into the vestibule in the midline. The ducts of Skene (paraurethral) glands and Bartholin glands also empty into the vestibule. Secretions from the Bartholin glands are responsible for sexually stimulated vaginal lubrication.

FIGURE 4.9. External female genitalia.
The muscles of the vulva (superficial transverse perineal, bulbocavernosus, and ischiocavernosus) lie superficial to the fascia of the urogenital diaphragm (Fig. 4.10). The vulva rests on the triangular-shaped urogenital diaphragm, which lies in the anterior part of the pelvis between the ischiopubic rami.

FIGURE 4.10. The urogenital diaphragm with the skin and subcutaneous fat cuts away. The musculature, blood supply, and nerve supply constitute the external part of the pelvic floor.
The Vagina
The lumen of the vagina is lined by a stratified squamous epithelium and surrounded by three layers of smooth muscle. Beneath the smooth muscle layers is a submucosal layer of connective tissue containing a rich supply of veins and lymphatic vessels. In children and young women, the anterior and posterior walls of the vagina are in contact due to the presence of submucosal rugae. Because the vagina is collapsed, it appears H-shaped in cross section. The underlying rugae connect to the tendinous arch of the pelvic fascia, which is the major support of the walls of the vagina and help maintain its normal architecture. With age and childbirth, the connection between the vaginal walls and the muscular pelvis may weaken or deteriorate, weakening the pelvic floor and causing the surrounding structures (i.e., bladder, rectum, urethra, and uterus) to become less stable.
The cervix joins the vagina at an angle between 45° and 90°. The area around the cervix, the fornix, is divided into four regions: the anterior fornix, two lateral fornices, and the posterior fornix. The posterior fornix is in close proximity to the peritoneum that forms the floor of the posterior pelvic cul-de-sac (pouch of Douglas). The cervical opening to the vagina, the external os, is round to oval in women who have not had children but is often a transverse slit after childbirth. The portion of the cervix that projects into the vagina is covered with stratified squamous epithelium, which resembles the vaginal epithelium. The squamous epithelium of the vaginal aspect of the exocervix changes to the columnar epithelium of the endocervical portion in the transformation zone¸ the most caudal part of which is the original squamocolumnar junction (SCJ). During adolescence and the menstrual years, the SCJ is visible at the upper limit of the transformation zone. As the level of sex steroids falls during menopause, the SCJ passes back up the canal until it is often barely visible, if at all. (The histology of the cervix is discussed in more detail in Chapter 47.)
At its lower end, the vagina traverses the urogenital diaphragm and is then surrounded by the two bulbocavernosus muscles of the vulva. These muscles act as a sphincter. The hymen, a fold of mucosa-covered connective tissue, somewhat obscures the external vaginal orifice. The hymen is fragmented into irregular remnants with sexual activity and childbearing. The major blood supply to the vagina is from the vaginal artery, a branch of the hypogastric artery, also known as the internal iliac and parallel veins.
Uterus and Pelvic Support
The uterus lies between the rectum and the bladder (Fig. 4.11). Various pelvic ligaments help support the uterus and other pelvic organs. The broad ligament overlies the structures and connective tissue immediately adjacent to the uterus. Because it contains the uterine arteries and veins and the ureters, it is important to identify the broad ligament during surgery. The infundibulopelvic ligament connects the ovary to the posterior abdominal wall and is composed mainly of the ovarian vessels. The uterosacral ligament connects the uterus at the level of the cervix to the sacrum and is, therefore, its primary support. The cardinal ligament is attached to the side of the uterus immediately inferior to the uterine artery. The sacrospinous ligament connects the sacrum to the iliac spine and is not attached to the uterus. This ligament is frequently used surgically to support the pelvic viscera.
The two major portions of the uterus are the cervix and the body (corpus), which are separated by a narrower isthmus. The length of the cervix is established at puberty. Before puberty, the relative lengths of the body of the uterus and cervix are approximately equal; after puberty, under the influence of increased estrogen levels, the ratio of the body to the cervix changes between 2:1 and 3:1. The junction of the uterus and fallopian tubes is called the cornu. The part of the corpus between the cornu is referred to as the fundus. In a woman who has had no children, the uterus is approximately 7 to 8 cm long and 4 to 5 cm wide at the widest part. The cervix is relatively cylindrical in shape and is 2 to 3 cm long. The body is generally pear shaped, with the anterior surface flat and the posterior surface convex. In cross section, the lumen of the uterine body is triangular.
The wall of the uterus consists of three layers:
1. The endometrium, the inner mucosa, consists of simple columnar epithelium with underlying connective tissue, which changes in structure during the menstrual cycle.
2. The myometrium, or middle layer, consists of smooth muscle. This layer becomes greatly distensible during pregnancy; during labor, the smooth muscle in this layer contracts in response to hormonal stimulation.
3. The serosa, or outermost layer, consists of a thin layer of connective tissue. It is distinct from the parametrium, a subserosal extension of the uterus between the layers of the broad ligament.
The position of the uterus can vary depending on the relationship of a straight axis that extends from the cervix to the uterine fundus to the horizontal. When a woman is in the dorsal lithotomy position, the uterus may be tilted forward (anteversion), slightly forward but functionally straight (midposition), or tilted backward (retroversion, RV). The top of the uterus can also fold forward (anteflexion) or backward (retroflexion, RF). Five combinations of these configurations are possible (Fig. 4.12). In addition, the uterus may be tilted axially to the right or left. The position of the uterus is clinically important. For example, estimation of gestational age in the late part of the first trimester may be difficult when the uterus is in the RVRF or RV positions. The risk of uterine perforation during procedures such as dilatation and curettage or insertion of an intrauterine device is increased in a woman with a retroflexed or anteflexed uterus. Applying traction on the cervix to pull the uterine canal into a straight line can greatly reduce this risk.
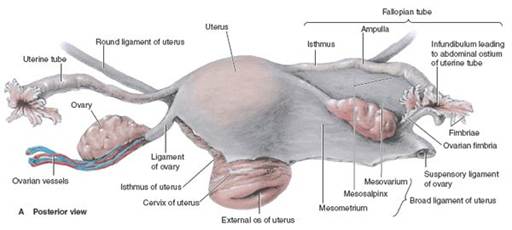

FIGURE 4.11. Internal female reproductive organs. (From Moore KL, Dalley AF. Clinically Oriented Anatomy. 5th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2006:Fig. 3.39A&B.)
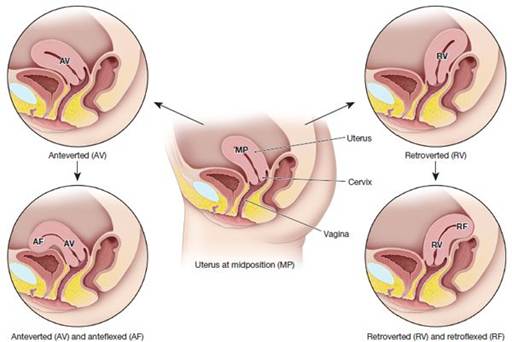
FIGURE 4.12. Positions of the uterus within the pelvis. (From Moore KL, Dalley AF. Clinically Oriented Anatomy. 5th ed. Baltimore, MD: Lippincott Williams & Wilkins; 2006:B3.17A-D.)
The blood supply to the uterus comes primarily from the uterine arteries, with a contribution from the ovarian arteries, whereas the venous plexus drains through the uterine vein.
Of particular importance in pelvic surgery is the relative position of the uterine arteries to the ureter.
The arteries travel in a lateral-to-medial direction at the level of the internal os of the cervix. At the point where they meet the uterus, they overlie the ureter. This proximity can cause inadvertent injury during pelvic surgery. The ureters lie between 1.5 and 3 cm from the uterine sidewall at this point (Fig. 4.13).
Uterine Tubes
The fallopian (uterine) tubes (oviducts) are approximately 7 to 14 cm in length and are divided into four portions: the interstitial portion of the tube that lies within the wall of the uterus and communicates between the uterine cavity and the next segment of the tube; the isthmus, a narrow and straight segment that forms the first portion outside the uterine wall; the ampulla, a widening central portion; and the infundibulum, fringed by the finger-shaped fimbriae that surround the ovary and collect the oocyte at the time of ovulation. The fallopian tubes are supplied by the ovarian and uterine arteries. The epithelial lining of the fallopian tube is ciliated columnar; the cilia beat toward the uterus, assisting in oocyte transport.

FIGURE 4.13. Relative locations of the ureter and uterine artery. During pelvic surgery, it is important to correctly identify the ureter in order to avoid injury to the uterine artery.
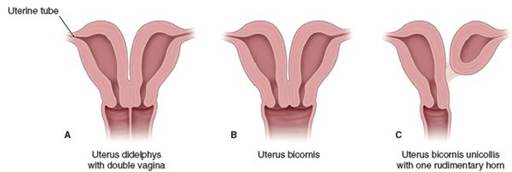
FIGURE 4.14. Uterine and vaginal anomalies. These anomalies result from abnormal or incomplete fusion of the paramesonephric ducts.
Ovaries
Each ovary is approximately 3 to 5 cm long, 2 to 3 cm wide, and 1 to 3 cm thick in the menstrual years. The size decreases by approximately two thirds after menopause, when follicular development ceases. The ovary is attached to the broad ligament by the mesovarium, to the uterus by the ovarian ligament, and to the side of the pelvis by the suspensory ligament of the ovary (infundibulopelvic ligament), which is the lateral margin of the broad ligament. The outer ovarian cortex consists of follicles embedded in a connective tissue stroma. Embryologically, this stroma is the medulla that originated as the gonadal ridge, whereas the cortex originated as coelomic epithelium. The medulla contains smooth muscle fibers, blood vessels, nerves, and lymphatics.
The ovaries are mainly supplied by the ovarian arteries, which are direct branches of the abdominal aorta, but there is also a blood supply from the uterine artery, a branch of the hypogastric artery (or internal iliac artery). Venous return via the right ovarian vein is directly into the inferior vena cava and from the left ovary into the left renal vein.
ANOMALIES OF THE FEMALE REPRODUCTIVE SYSTEM
Anatomic anomalies are infrequent and arise from defects during embryologic development. Ovarian dysgenesis or congenital absence is rare except in cases of chromosomal abnormalities. In Turner syndrome (45XO), there are streaks of abnormal ovarian tissues in the pelvis. In the anatomically female patient with a male chromosome compliment (46XY), the gonads only partially descend and can usually be found in the pelvis or even in the inguinal canal.
Much more common are Müllerian (paramesonephric) abnormalities, most of which stem from incomplete or anomalous fusion of the Müllerian ducts. Absence of the uterus occurs when the Müllerian ducts degenerate, a condition called Müllerian agenesis (Fig. 4.14). This condition is associated with vaginal anomalies (such as absence of the vagina), because vaginal development is stimulated by the developing uterovaginal primordium. Because the vulva and the external portion of the vagina develop from the invagination of the urogenital sinus, the external genitalia can appear normal in these women. A double uterus (uterus didelphys) occurs when the inferior parts of the Müllerian ducts do not fuse; this condition may be associated with a double or a single vagina. A bicornuate uterus (Fig. 4.15) results when lack of fusion is limited to the superior portion of the uterine body. If one of the ducts is poorly developed, and fusion with the other duct does not occur, the result is a bicornuate uterus with a rudimentary horn. This horn may or may not communicate with the uterine cavity.
The mesonephric ducts normally degenerate in the female embryo during development of the reproductive tract. However, remnants of the mesonephric ducts can persist, which can manifest as Gartner cysts (Fig. 4.16). These cysts are located along the vaginal wall or within the broad ligament of the uterus.

FIGURE 4.15. Reconstructed coronal view of bicornuate uterus.
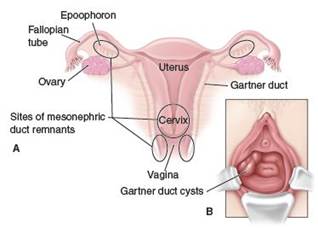
FIGURE 4.16. Gartner cysts. (A) These cysts are remnants of the mesonephric ducts that are not completely resorbed during development. (B) Gartner cysts are located along the sidewall of the vagina and can be identified during a pelvic examination.
Because the paramesonephric system develops alongside the renal system, when one system is abnormally formed, an abnormality in the other is likewise frequently present. For example, in a woman with renal agenesis on one side, an abnormal fallopian tube is often found. Conversely, despite the functional connection between the ovaries and fallopian tubes, a lack of one does not indicate a probable lack of the other.
Clinical Follow-Up
You are guided in your surgery as you identify the uterine arteries, knowing that the arteries travel in a lateral-to-medial direction at the level of the internal os of the cervix. At the point where the arteries meet the uterus, you are aware that they overlie the ureter and that it is at this point that great attention to anatomy is required to avoid inadvertent injury to the ureters. Knowing that the ureters lie between 1.5 and 3 cm from the uterine sidewall at this point, you are guided in your dissection and are able to visually identify the ureters and, thus, protect them during the surgery.
thePoint Visit http://thePoint.lww.com/activate for an interactive USMLE-style question bank and more!