Chapter 2 The Obstetrician– Gynecologist’s Role in Screening and Preventive Care
This chapter deals primarily with APGO Educational Topic Areas:
TOPIC 3 PAP SMEAR AND DNA PROBES/CUlTURE
TOPIC 7 PREVENTIVE CARE AND HEAlTH MAINTENANCE
Students should be able to counsel patients on important preventive medicine and health maintenance topics, such as immunization, diet, and exercise.
They should be able to describe appropriate screening protocols for cancer, cardiovascular disease, and osteoporosis.Clinical Case
A pleasant 57-year-old moderately obese, insulin-dependent diabetic, menopausal woman is seen for routine gynecologic care. She feels well generally but complains that she has constant perineal itching. Another physician has treated her for recurrent vulvovaginal candidiasis over the last 5 years, using topical antifungal and steroidal cream preparations. She is a 1-pack-per-day smoker who has unsuccessfully tried to quit multiple times in the past. On physical examination, you find hyphae on a KOH preparation from her vagina and also notice three areas of slight discoloration on both labia majora. You explain your concern about the relationship of continued vulvar pruritus and vulvar carcinoma and recommend a punch biopsy of one of the discolored areas of her labia. She consents, and two specimens are obtained. You also treat her with systemic and topical antifungal medications and suggest she see her internist to review her diabetic management. Again you discuss smoking cessation.
As the population ages, the health care needs of women will change, and thus the provision of primary and preventive care in the obstetric and gynecologic setting must evolve to meet these needs. The obstetrician–gynecologist is in a unique position to provide screening, preventive care, and counseling to women, which can have a positive impact on quality of life as well as morbidity and mortality.
 PREVENTIVE CARE
PREVENTIVE CARE
Preventive care is both beneficial and cost-effective over time.
Preventive medicine encompasses both primary and secondary prevention. In primary prevention, an attempt is made to eliminate or ameliorate risk factors for disease and, thus, prevent its occurrence or modify its severity. Primary prevention may include health education and behavioral interventions to promote a healthier lifestyle, including immunizations, fitness and nutrition, hygiene, smoking cessation, personal safety, and safe sex. Secondary prevention focuses on screening tests for diseases, which are performed when the patient is usually asymptomatic, allowing prompt intervention that reduces morbidity and mortality. Screening tests are performed as part of periodic health assessments (often called “annual examinations”) that afford an opportunity to evaluate and counsel patients based on their age and risk factors.Primary preventive care concerning sexually transmitted diseases (STDs) is found in Chapters 28 and 29. Similar care to increase the quality of life of newborn and mother before, during, and after pregnancy is found in Chapter 6.
IMMUNIZATIONS
In the United States, vaccination programs that focus on infants and children have reduced the occurrence of many childhood diseases. However, many adolescents and adults are still affected by vaccine-preventable diseases, such as influenza, varicella, hepatitis A, hepatitis B, measles, rubella, and pneumococcal pneumonia. Each year, it is estimated that pneumococcal infection, influenza, and hepatitis B cause as many as 45,000 deaths in adults. Obstetrician–gynecologists and other clinicians who provide primary care to women have opportunities to counsel women on the need for immunizations and may administer them or refer the patient to a facility that does provide them.
The clinician should attempt to gather a complete immunization history from each patient, including risk factors, indicating the need for immunization.
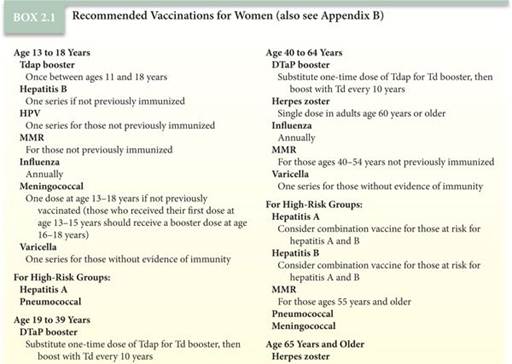
Previous vaccination records are particularly valuable if the patient is in doubt about her immunization history. In lieu of a clear history, the physician should assume that a patient has not been immunized and proceed accordingly. The recommended vaccinations for women are listed in Box 2.1. Because immunization recommendations do change, it is useful to know that the most current recommendations can be accessed at the Center for Disease Control’s (CDC) National Immunization Program Web page (www.cdc.gov/vaccines).Prevention of cervical neoplasia and cancer with the use of the human papillomavirus (HPV) vaccine is discussed in detail in Chapter 47. The American College of Obstetricians and Gynecologists (College) recommends the initial vaccination for girls ages 11 to 12 years. Although obstetrician–gynecologists do not routinely care for girls in this age group, they are in a unique position to advocate for the use of the vaccine for females ages 13 to 26 years (the catch-up vaccination period). During a health care visit with a girl or a woman in the age range for vaccination, an assessment of the patient’s HPV vaccine status should be conducted and documented in the patient record. The HPV vaccine is most effective when given before any exposure to HPV infection, but sexually active women who were exposed to HPV prior to vaccination can receive and benefit from the vaccine. Women should be informed that HPV immunization has been shown to be nearly 100% effective in the prevention of diseases related to the virus genotypes covered by the particular vaccine. This may include cervical intraepithelial neoplasia (CIN) and condylomatous vulvar disease. HPV vaccination should not be given during pregnancy but may be given to breastfeeding mothers.
SECONDARY PREVENTION: PERIODIC ASSESSMENT AND SCREENING
Periodic assessments conducted at regular intervals (i.e., annually) are an integral part of preventive health care and include screening, evaluation, and counseling.
Recommendations for periodic health assessments and screening vary by age group and are based on risk factors as well as epidemiologic information (see Appendix B). This care starts with a thorough medical history, physical examination, and appropriate laboratory testing. The history, physical examination, and results of laboratory tests help guide interventions and counseling and may reveal additional risks that require targeted screening or evaluation.The recommendations presented in Appendix B have been selected from a variety of sources. These recommendations take into account factors such as the leading causes of morbidity and mortality in each age group as well as chronic health conditions that limit activity of adults (e.g., arthritis or other musculoskeletal disorders and circulatory disorders) that become more prevalent as women age.
Characteristics of Screening Tests
The principle behind routine screening is to detect the presence of disease in asymptomatic individuals without specific risk factors. Disease detection in this sojourn time interval allows maximum decrease in morbidity and mortality. The diseases screened for should be prevalent in the population and amenable to early intervention. Screening tests are currently available for a variety of cancers, metabolic disorders, and STDs. Examples of screening tests are the Pap test and mammography.
Not every disease can be detected by screening, and screening is not cost-effective or feasible for every disease. The concepts of sensitivity and specificity are used to describe the efficacy of screening tests in detecting a disorder. The sensitivity of a test is the proportion of affected individuals that test positive on the screening test. The specificity is the proportion of unaffected individuals that test negative on the screening test. An effective screening test should be both sensitive (it has a high detection rate) and specific (it has a low false-positive rate). Other criteria for effective screening tests pertain to the population being tested and the disease itself (Box 2.2).
Cancer Screening
The Pap smear (cervical cancer) and mammography (breast cancer) are the only recognized effective screening tests for gynecologic cancers. There is no screening test with the requisite sensitivity and specificity to detect ovarian cancer. Women should be educated about the unique early signs and symptoms of ovarian cancer that may aid in earlier diagnosis (see Chapter 50). Likewise, screening tests are not available for endometrial, vaginal, or vulvar cancers. A history of postmenopausal bleeding (endometrial cancer) or chronic and persistent vulvar itching (vulvar cancer) may be useful, but for these neoplasms, as well as for cervical cancer, a tissue biopsy is needed to identify either frank invasion or a precursor lesion.
Endometrial, vulvar, and vaginal biopsies are not screening tests.

BOX 2.2 Criteria for Screening Tests
Criteria for the Disease
• Asymptomatic period long enough to allow detection
• Prevalent enough to justify screening
• Treatable; treatment in an asymptomatic stage (preferably a superior treatment)
• Sufficient effect on quality and/or length of life
Criteria for the Test
• Sensitive
• Specific
• Safe
• Affordable
• Acceptable to patients
Criteria for the Population to Be Tested
• High disease prevalence
• Accessible
• Compliant with testing and treatment
Breast Cancer
Breast cancer is the most common cancer among women in the United States after skin cancer. It has a lifetime risk of 12.5%, and it is the second leading cause of cancer-related death in women. It is important that clinicians assess each patient’s breast cancer risk by taking a thorough history, because the recommendations for screening differ based on risk factors. A computer program called the Breast Cancer Risk Assessment Tool (http://www.cancer.gov/bcrisktool/) is available to estimate a patient’s risk of developing breast cancer (see Chapter 33).
For women at average risk, there are two major screening examinations for breast cancer: clinical breast examination and screening mammography. The College recommends:
• An annual clinical breast examination for all women ages 40 years and older and every 1 to 3 years for women ages 20 to 39 years (Women at high risk for breast cancer ages 20–39 years may be considered for annual clinical breast examination.)
• Screening mammography annually starting at age 40 years
The American Cancer Society recommends:
• Clinical breast examinations every 1 to 3 years for women between ages 20 and 39 years at average risk
• Annual clinical breast examination and screening mammography starting at age 40 years for women at average risk
Breast self-examination is not universally recommended; instead, breast self-awareness is to be encouraged and supported by physicians. Ultrasound and magnetic resonance imaging (MRI) have no current role in screening women at average risk but are used as adjunctive tests. These imaging modalities are used for the assessment of palpable masses. MRI is also recommended, in addition to yearly mammography, for women at very high risk (greater than 20% lifetime risk according to family history risk assessment or who have a first-degree relative with BRCA1 or BRCA2 gene mutation).
Cervical Cancer
Cervical intraepithelial neoplasia is the precursor lesion to cervical cancer. CIN may regress spontaneously, but, in some cases, CIN 2 and CIN 3 progress to cancer over time. Exfoliative cytology, specifically the Pap test (either slide or liquid based) with or without high-risk HPV identification, allows early diagnosis in most cases. The reduction in mortality from cervical cancer since the Pap test was introduced in the 1940s is testimony to the success of this screening program.
The following are recommendations for cervical cancer screening for women based on the U.S. Preventive Services Task Force as well as the American Cancer Society, the American Society for Colposcopy and Cervical Pathology, and the American Society for Clinical Pathology. These guidelines apply to the general population but not to women at high risk (i.e., women with a history of cervical cancer or diethylstilbestrol exposure or women who are immunocompromised).
• Younger than 21 years: should not be screened regardless of age of sexual initiation or other risk factors.
• Ages 21 to 29 years: recommend screening every 3 years with cytology.
• Ages 30 to 65 years: recommend screening every 3 years with cytology or every 5 years with cytology and HPV testing (co-tests).
• Older than 65 years: recommend against screening in women with adequate negative prior screening (three consecutive negative cytology results or two consecutive negative co-tests in 10 years) and no history of CIN 2 or greater within the last 20 years. Screening should not be resumed for any reason, even with report of a new sex partner.
• After hysterectomy for benign conditions with removal of the cervix: recommend against screening for vaginal cancer without any history of CIN 2 or greater. Screening should not be resumed for any reason, even with report of a new sex partner.
• Women with a history of CIN 2, CIN 3, or adenocarcinoma in situ should continue screening for a total of 20 years after spontaneous regression or appropriate management of CIN 2, CIN 3, or adenocarcinoma in situ, even if it extends the screening past age 65 years.
• HPV vaccinated: should not change guidelines.
• Annual gynecologic examination is appropriate even if screening is not performed at each visit.
Colorectal Carcinoma
With nearly 75,000 new cases of colorectal cancer annually in women and over 25,000 deaths, colorectal cancer is the third leading cause of cancer death in women after lung cancer and breast cancer. Because early detection (preinvasive or early invasive stage) allows effective management for most patients, screening is appropriate and recommended.
Screening for colorectal cancer is recommended for all women at average risk, starting at age 50 years. The preferred method is colonoscopy performed every 10 years.
Other acceptable screening tests include:
• Annual fecal occult blood testing (FOBT) or fecal immunochemical testing (FIT)
• Flexible sigmoidoscopy every 5 years
• Double-contrast barium enema every 5 years
• Computed tomography colonography (virtual colonoscopy) every 5 years
• Stool DNA, interval not established
Flexible sigmoidoscopy will miss right-sided lesions, which may account for up to 65% of advanced colorectal cancers in women. Both FOBT and FIT require two or three stool samples collected by the patient at home and returned for analysis. Screening by FOBT of a single stool sample from a rectal examination by the physician is not adequate for the detection of colorectal cancer and is not recommended. Different recommendations apply to women at increased risk and at high risk.
Sexually Transmitted Diseases
Appropriate STD screening in nonpregnant women depends on the age of the patient and the assessment of risk factors (Box 2.3). Because of the risk that STDs pose in pregnancy, pregnant women are routinely screened for syphilis, HIV, chlamydia, and gonorrhea (see Chapter 29).
Human Immunodeficiency Virus
The demographics of the HIV epidemic have changed over the last two decades. Prevalence has increased among adolescents, women, persons who reside outside metropolitan areas, and heterosexual men and women. Many are not aware that they are infected.
HIV testing is recommended for all women, and targeted testing is recommended for women with risk factors. Although women of reproductive age should be tested at least once in their lifetime, there is no consensus regarding repeat testing. Obstetrician–gynecologists should review their patient’s risk factors annually and assess the need for retesting. Repeat HIV testing should be offered at least annually to women who:
BOX 2.3 Risk Factors for Sexually Transmitted Diseases
• History of multiple sex partners
• Sexual partner with multiple sexual contacts
• Sexual contact with individuals with culture-proved STD
• History of repeated STDs
• Attendance at clinics for STDs
American College of Obstetricians and Gynecologists. Annual Women’s Health Care.http://www.acog.org/About_ACOG/ACOG_Departments/ Annual_Womens_Health_Care.
• Are injection drug users
• Have sex partners who are injection drug users or are HIV infected
• Exchange sex for drugs or money
• Have been diagnosed with another STD in the last year
• Have had more than one sex partner since their most recent HIV test
Obstetrician–gynecologists should also encourage women and their prospective sex partners to be tested prior to initiating a new sexual relationship. Periodic retesting could be considered even in the absence of risk factors, depending on clinical judgment and the patient’s wishes.
The most common screening test is the enzyme-linked immunosorbent assay (ELiSA), which is performed on a blood sample. There are also ELISA tests that use saliva or urine. A positive (reactive) ELISA must be confirmed by a supplemental test, such as the Western blot, to make a positive diagnosis.
Chlamydia Infection
Infection caused by Chlamydia trachomatis is the most commonly reported bacterial STD in the United States and is often asymptomatic. Over 1.3 million cases were reported to the CDC in 2010, a rate of 426 per 100,000, and it is estimated that another 1.7 million cases go undiagnosed. If untreated, chlamydia can cause significant long-term complications, including infertility, ectopic pregnancy, and chronic pelvic pain. Diagnosing chlamydia promptly is necessary to prevent these complications. The College recommends annual screening for chlamydia in sexually active women ages 25 years and younger. Asymptomatic women ages 26 years and older who are at high risk for infection should be routinely screened. Nucleic acid amplification tests (NAATs) of endocervical swab specimens can identify infection in asymptomatic women with high specificity and sensitivity. NAATs of vaginal swabs and urine samples have comparable sensitivity and specificity.
Gonorrhea Infection
Over 309,000 cases of gonorrhea were reported in 2010, a rate of 100.8 per 100,000. It is estimated that the same number went unreported. Infection can be symptomatic with cervicitis and vaginal discharge, or it may be asymptomatic. Gonorrhea may lead to pelvic inflammatory disease, which is associated with long-term morbidity due to chronic pelvic pain, ectopic pregnancy, and infertility.
The College recommends annual screening for gonorrhea in sexually active women ages 25 years and younger. Asymptomatic women ages 26 years and older who are at high risk for infection should be routinely screened. Screening can be done by cervical cultures or by newer techniques, such as NAATs and nucleic acid hybridization tests that have better sensitivity with comparable specificity (see Chapter 29).
Syphilis
Syphilis is not a common disease in the United States, but the rate has increased over the last few years. About 13,774 cases of primary and secondary syphilis were diagnosed in 2010, which translates to a rate of 7.9 cases per 100,000. Overall increases were seen primarily in men; in women, the rate is 1.1 cases per 100,000.
Syphilis is a systemic disease caused by the bacterium Treponema pallidum. If untreated, syphilis may progress from a primary infection characterized by a painless ulcer (chancre) to secondary and tertiary infections. Signs and symptoms of secondary infection include skin manifestations and lymphadenopathy; tertiary infection may cause cardiac or ophthalmic manifestations, auditory abnormalities, and gummatous lesions. Serologic tests may be negative in the early stages of infection.
The College recommends annual syphilis screening for women at increased risk (see Box 2.3). All pregnant women should be serologically screened as early as possible in pregnancy and again at delivery. Due to the possibility of a false-negative result in early stages of infection, patients who are considered at high risk or who are from areas of high prevalence should be retested at the beginning of the third trimester.
Screening is done with nontreponemal tests such as the Venereal Disease Research Laboratory test or rapid plasma reagin. These tests are followed by confirmatory treponemal tests such as T. pallidum particle agglutination. The specificity of the nontreponemal tests may be reduced in the presence of other conditions, such as pregnancy, collagen vascular disease, advanced cancer, tuberculosis, malaria, and rickettsial diseases.
Metabolic and Cardiovascular Disorders
Routine screening can also be applied to noninfectious and noncancerous diseases, such as metabolic disorders and cardiovascular disease. Women should be evaluated for lifestyle issues and risks based on a history and physical examination. In many cases, early identification of risk factors and appropriate interventions are key components of disease prevention.
Osteoporosis
osteoporosis affects approximately 13% to 18% of American women ages 50 years and older, and another 37% to 50% have osteopenia, or low bone mineral density (BMD). Osteoporosis-associated fracture, especially of the hip and spine, are leading causes of morbidity and mortality, increasing in proportion to age. Osteoporosis is a complication of menopause that is largely preventable with screening strategies, lifestyle modifications, and pharmacologic interventions.
BMD is an indirect measure of bone fragility. BMD is measured using dual-energy x-ray absorptiometry of the hip or the lumbar spine. The results are expressed in standard deviations compared with a reference population stratified by age, sex, and race. The T-score is expressed as the standard deviation from the mean peak BMD of a normal, young adult population; and the Z-score is expressed as the standard deviation from the mean BMD of a reference population of the same sex, race, and age as the patient. Z- and T-scores are used for hip and spine measurements. The World Health Organization (WHO) defines a normal BMD T-score as ≥−1. Osteopenia (low bone mass) is defined as a T-score between −1 and −2.5. Osteoporosis is defined as a T-score ≤−2.5. Because of variance in the measurements obtained by the different commercial devices and at different sites, T- and Z-scores cannot be used as true screening tests, but they are good predictors of the risk of fracture. When these scores indicate low bone mass, the fracture risk assessment tool (FRAX) can be used in women older than age 40 years to predict their risk of fracture in the next 10 years. Developed in collaboration with WHO, FRAX can be used to guide decisions about interventions including lifestyle changes and medical therapy to prevent or slow bone loss.
The College recommends BMD testing for all postmeno-pausal women starting at age 65 years. BMD testing should also be performed in younger postmenopausal women who have at least one risk factor for osteoporosis (Box 2.4). In addition, postmenopausal women who experience a fracture should have BMD testing to ascertain if they are osteoporotic; if so, treatment for osteoporosis is added to the therapy for the fracture. Certain diseases or medical conditions (e.g., Cushing disease, hyperparathyroidism, hypophosphatasia, inflammatory bowel disease, lymphoma, and leukemia) and certain drugs (e.g., phenobarbital, phenytoin, corticosteroids, lithium, and tamoxifen) are associated with bone loss. Women with these conditions or taking these drugs may need to be tested more frequently.
BOX 2.4 When to Screen for Bone Density Before Age 65 Years
Bone density should be screened in postmenopausal women younger than 65 years if any of the following risk factors are noted:
• Medical history of a fragility fracture
• Body weight less than 127 lb
• Medical causes of bone loss (medications or diseases)
• Parental medical history of hip fracture
• Current smoker
• Alcoholism
• Rheumatoid arthritis
American College of Obstetricians and Gynecologists. Osteoporosis, Practice Bulletin No. 129. Washington, DC: American College of Obstetricians and Gynecologists; September 2012.
Women should be counseled on the risks of osteoporosis and related fractures and the following preventive measures:
• Adequate calcium consumption (1,000–1,300 mg/day, depending on age) using dietary supplements if dietary sources are not adequate
• Adequate vitamin D consumption (600–800 international units daily, depending on age) and exposure to the natural sources of this nutrient
• Regular weight-bearing and muscle-strengthening exercises to reduce falls and prevent fractures
• Smoking cessation
• Moderation of alcohol intake
• Fall prevention strategies
Diabetes Mellitus
Diabetes mellitus is a group of disorders that share hyperglycemia as a common feature. Even when symptoms are not present, the disease can cause long-term complications. Ideally, it should be detected and treated in its early stages. A screening fasting blood glucose test is recommended for women beginning at age 45 years and every 3 years thereafter. Screening should begin at a younger age or more frequently in individuals with risk factors, which include being overweight (body mass index [BMI] ≥25), first-degree relative with diabetes mellitus, habitual physical inactivity, high-risk race or ethnicity, having given birth to a newborn weighing more than 9 lb, history of gestational diabetes, hypertension high-density lipoprotein cholesterol level less than 35 mg/dL, triglyceride level greater than 250 mg/dL, history of impaired glucose tolerance or impaired fasting glucose, polycystic ovary syndrome, history of vascular disease, and other clinical conditions associated with insulin resistance. In 2009, the American Diabetes Association endorsed the use of HgbA1c as the favored test for the diagnosis of diabetes.
Thyroid Disease
Thyroid disease is often asymptomatic and, if untreated, can lead to serious medical conditions including the appearance of dementia in older adults. Because hypothyroidism in older women can present as dementia, thyroid-stimulating hormone levels should be tested every 5 years starting at age 50 years in women without risk factors.
Earlier or more frequent screening should may be appropriate in women with a strong family history of thyroid disease or with an autoimmune disease (evidence of subclinical hypothyroidism may be related to unfavorable lipid profiles).
Hypertension
It is estimated that approximately 30% of adults ages 20 years and older have hypertension, which is defined as a systolic blood pressure of ≥140 mm Hg or a diastolic blood pressure of ≥90 mm Hg. Hypertension is one of the most important risk factors for heart disease and cerebrovascular accidents, two of the three leading causes for mortality among women. Hypertension is also a leading cause of mortality. About a third of those with hypertension do not know they have it. Because hypertension is often asymptomatic, the College recommends screening for hypertension annually for women and girls ages 13 years and older, regardless of blood pressure level. Prehypertension (120–139/80–90) should prompt a review for comorbid conditions and more frequent evaluation of blood pressure.
Lipid Disorders
Coronary heart disease (CHD) is a leading cause of death for both men and women in the United States and accounts for approximately 500,000 deaths each year. Abnormal cholesterol levels have been linked to atherosclerosis as well as cardiovascular and cerebrovascular disease. Physicians and patients alike should be reminded that a 1% reduction in serum cholesterol levels results in a 2% reduction in CHD rates. Lipid levels are monitored by measuring low-density lipoprotein, high-density lipoprotein, and triglycerides. Approximately one in five adult Americans has a high total cholesterol level (≥240 mg/dL).
Current guidelines recommend that women without risk factors have a lipid profile assessment every 5 years, beginning at age 65 years in women without risk factors. Earlier screening may be appropriate in women with risk factors. Risk factors for high cholesterol are a family history of familial hyperlipidemia, family history of premature (age younger than 50 years for men and younger than 60 years for women) cardiovascular disease, personal or family history of peripheral vascular disease, obesity, diabetes mellitus, and multiple CHD risk factors (e.g., tobacco use and hypertension).
Obesity
Obesity is associated with increased risk for heart disease, type 2 diabetes, hypertension, certain types of cancer (e.g., endometrial, colon, and breast), sleep apnea, osteoarthritis, gallbladder disease, and depression. Measurement of height and weight and the calculation of a BMI are recommended as part of the periodic assessment (Box 2.5). Obese people with a BMI of 30 or more have up to twofold increased risk of death. Behavioral therapy is the most common treatment, although bariatric surgery is an option to be considered in those who are morbidly obese and have proven refractory to treatment.
BOX 2.5 Body Mass Index
• BMI alt=image>
3. Nonmaleficence follows from beneficence, obliging the physician to not harm or cause or allow injury to the patient. The well-known maxim primum non nocere (“first do no harm”) comes from this ethical principle. This also includes the physician’s obligation to maintain medical competence through study, application, and enhancement of medical knowledge and skills as well as to address and rehabilitate any behavior that diminishes the physician’s capability to practice, such as substance abuse. Moreover, the physician should avoid any discrimination on the basis of race, color, religion, national origin, political viewpoints, financial status, or any other factor as well as to eschew any conflicts of interest. The application of these principles consists of balancing benefits and harms, both intentional harms and those that can be anticipated to arise despite the best intentions (e.g., unwanted adverse effects of medication or complications of surgical treatment).
4. Justice is the physician’s obligation to render to the patient what is due or owed. It is the most complex of the ethical principles, in part because of the physician’s role in the allocation of limited medical resources. Justice is the obligation to treat equally those who are alike or similar according to whatever criteria are selected. Individuals should receive equal treatment, unless scientific and clinical evidence establishes that they differ in ways that are relevant to the treatments in question.
Steps for Ethical Clinical Management
Using a stepwise, systematic approach to a difficult clinical situation, based on an ethical foundation has been consistently found to benefit patients, their families, physicians, the health care system (including the hospital), and society. An example of such an application is found in Box 3.1.
BOX 3.1 One Case Study: Five Approaches
Although the several approaches to ethical decision making may all produce the same answer in a situation that requires a decision, they focus on different, though related, aspects of the situation and decision. Consider, for instance, how they might address interventions for fetal well-being if a pregnant woman rejects medical recommendations or engages in actions that put the fetus at risk.
A principle-based approach would seek to identify the principles and rules pertinent to the case. These might include beneficence–nonmaleficence to both the pregnant woman and her fetus, justice to both parties, and respect for the pregnant woman’s autonomous choices. These principles cannot be applied mechanically. After all, it may be unclear whether the pregnant woman is making an autonomous decision, and there may be debates about the balance of probable benefits and risks of interventions to all the stakeholders as well as about which principle should take priority in this conflict. Professional codes and commentaries may offer some guidance about how to resolve such conflicts.
A virtue-based approach would focus on the courses of action to which different virtues would and should dispose the obstetrician–gynecologist. For instance, which course of action would follow from compassion? From respectfulness? And so forth. In addition, the obstetrician– gynecologist may find it helpful to ask more broadly: Which course of action would best express the character of a good physician?
An ethic of care would concentrate on the implications of the virtue of caring in the obstetrician–gynecologist’s special relationship with the pregnant women and with the fetus. In the process of deliberation, individuals using this approach generally would resist viewing the relationship between the pregnant woman and her fetus as adversarial, acknowledging that most of the time women are paradigmatically invested in their fetus’ well-being and that maternal and fetal interests usually are aligned. If, however, a real conflict does exist, the obstetrician–gynecologist should resist feeling the need to take one side or the other. Instead, he or she should seek a solution in identifying and balancing his or her duties in these special relationships, situating these duties in the context of a pregnant woman’s values and concerns, instead of specifying and balancing abstract principles or rights.
To take one example, in considering a case of a pregnant woman in preterm labor who refuses admission to the hospital for bed rest or tocolytics, Harris combines a care or relational perspective with a feminist perspective to provide a “much wider gaze” than a principle-based approach might:
The clinician would focus attention on important social and family relationships, contexts or constraints that might come to bear on [a] pregnant [woman’s] decision making, such as her need to care for other children at home or to continue working to support other family members, or whatever life project occupied her, and attempt to provide relief in those areas….[Often] fetal well-being is achieved when maternal well-being is achieved.
As this example suggests, a feminist ethics approach would attend to the social structures and factors that limit and control the pregnant woman’s options and decisions in this situation and would seek to alter any that can be changed. It also would consider the implications any intervention might have for further control of women’s choices and actions—for instance, by reducing a pregnant woman, in extreme cases, to the status of “fetal container” or “incubator.”
Finally, a case-based approach would consider whether there are any relevantly similar cases that constitute precedents for the current one. For instance, an obstetrician– gynecologist may wonder whether to seek a court order for a cesarean delivery that he or she believes would increase the chances of survival for the child-to-be but that the pregnant woman continues to reject. In considering what to do, the physician may ask, as some courts have asked, whether there is a helpful precedent in the settled consensus of not subjecting a nonconsenting person to a surgical procedure to benefit a third party, for instance, by removing an organ for transplantation.
Harris LH. Rethinking maternal-fetal conflict: gender and equality in perinatal ethics. Obstet Gynecol 2000;96:786–91. In American College of Obstetricians and Gynecologists. Ethical Decision Making in Obstetrics and Gynecology. ACOG Committee Opinion 309. Washington DC: American College of Obstetricians and Gynecologists, 2007.
There are six steps in the decision-making process.
1. Identify the decision makers. The first step in clinical management is to answer the question: “Whose decision is it?” The patient is presumed to have the capacity to choose among evidence-based, medically acceptable management alternatives or to refuse treatment. Capacity depends on the patient’s ability to understand information and appreciate the implications of the information presented and may vary among individuals. Capacity must not be confused with competence (authority to make decisions). Competence is a narrow legal determination made by health care professionals with expertise in this determination (psychologists, psychiatrists, or others), by attorneys, or by a judge. Understanding the difference between patient capacity and patient competency is crucial in emotion-filled, difficult clinical decision-making situations. If a patient is determined to be legally incompetent, or if the physician believes the patient does not have the capacity for decision making, a surrogate decision maker must be identified. In the absence of a durable power of attorney, family members may be called on to render proxy decisions. In some situations, the court may be called upon to appoint a guardian. A surrogate decision maker should strive to make the decision that the patient would have wanted or, if the patient’s wishes are not known, that will promote the best interests of the patient. In emergency situations, physicians may have to assume this role for a limited time while an appropriate decision maker is identified. In the obstetric setting, a pregnant woman is considered the appropriate decision maker for the fetus that she is carrying.
2. Collect data in as objective a manner as possible. Consultation is often useful to facilitate this task.
3. Identify and evaluate all medically appropriate management options.
4. Systematically evaluate these options. After elimination of any unethical options, the remaining choices are reviewed, and the “best management” is chosen. The values of the patient generally will be the most important consideration as decision making proceeds.
5. Identify ethical conflicts and set priorities, then select the option that can best be justified.
6. Reevaluate the decision after it is acted on based on the clinical outcomes. If the management did not adequately resolve the problem, a reevaluation of all the information and another management plan may be used. Valuable questions at this time include, “Was the best possible decision made?” and “What lessons can be learned from the discussion and resolution of the problem?”
It is important for the individual physician to find or develop guidelines for decision making that can be applied consistently in facing ethical dilemmas. The American College of Obstetricians and Gynecologists (College) and many other such professional organizations provide guidelines that often facilitate this important task for physicians.
Sometimes, however, a medical or surgical management results in an adverse and/or unexpected outcome. Offering the physician’s best, honest understanding of what happened and why to the patient (and her family and other stakeholders) is a clear ethical responsibility of physicians, as is the clear documentation of this discussion in the medical record. When the patient or patient’s family questions this explanation, the specter of medical liability (sometimes misidentified as medical malpractice) looms.
 MEDICAL LIABILITY
MEDICAL LIABILITY
When an outcome is perceived to be less than optimal, a medical liability action (i.e., lawsuit) could ensue. Such situations are best prevented by the practice of evidence-based medicine as well as clear, honest, and complete communication between patient and physician. Appropriately detailed documentation in the medical record is very important.
Informed Consent
Providing “informed consent” is actually a process, which is a component of the care that should be provided by all physicians every day with every patient. Simply stated, it involves the physician apprising a woman of the various options available for both her preventive care and specific problems. The process of informed consent is the responsibility of the physician and cannot be delegated to others. Discussion should also cover the findings and information that is presently known as well as any further investigations that may be recommended, including their indications, risks, benefits, and alternatives. The patient should also be made aware that she has the option of no treatment. If another physician’s assistance is desired, a consultation or referral may be of benefit. Throughout these discussions, the patient is given opportunity to ask questions which the physician answers fully. This process spans each action of every physician from giving an aspirin for a headache to major surgery. In actual practice, informed consent is of particular importance as part of major management decisions and procedures, such as childbirth and surgery. Appropriate documentation of the process includes the signing of an informed consent form that states that the above process has been followed and that the patient agrees to the suggested management plan (or to no treatment at that time). The patient, a witness, and, usually, the physician sign the document, which is placed in the medical record. Often a copy is given to the patient.
Sometimes, however, the patient or family still questions the decisions and outcomes. In this circumstance, medical liability litigation may ensue.
Medical Liability Action
Medical liability action can be a significant source of fear and anxiety for the physician. Understanding the components of such an action is helpful, as is the recognition that in the current system of jurisprudence, a lawsuit can be brought by the patient or family irrespective of the actual quality of medical care rendered. Obtaining assistance from resources such as the “risk manager” of the health care system or practice as well as legal counsel is vital.
The components of a legal action vary from state to state, but some are common in most situations:
• A certificate of merit, a short written statement, usually by a physician knowledgeable in the issues of the action, saying that there is sufficient information to support a medical liability action, must be approved by a court in order for litigation to proceed.
• The plaintiff(s) (the patient or sometimes the family of the patient) and the defendant(s) (the physician[s], hospital[s], and/or health care system involved in the case) are identified.
• The plaintiff files a complaint specifying what the plaintiff believes to be wrong and why.
• Counsel for both parties requests the medical records and any other relevant information (laboratory records, billing and financial records, and some communications). Some information is considered exempt (privileged, i.e., it cannot be used) such as communications with counsel.
• Expert witnesses are retained by both parties. They are expected to be knowledgeable about the medicine involved in the case. The opinions of these individuals are theoretically to be based solely on the medical information and their knowledge of the issues. They should not be influenced by who retains them or how much they are paid for their services. In practice, experts often serve as advocates for the client represented by the attorney who hired the expert. Many professional organizations now provide guidelines for these individuals. The College does publish such guidelines.
Differentiating between Maloccurrence and Malpractice
Medical maloccurrence is defined as undesirable outcome irrespective of the quality of care provided. For an outcome to be considered medical malpractice, it must be demonstrated to have resulted from negligence (i.e., the care provided fell below the expected standard of care). Medical malpractice differs from medical maloccurrence by the demonstration of negligence.
After review of all available information and the opinions of the expert witnesses, counsel for the plaintiff and defendant have three primary options: 1) agree upon a settlement, with a specific financial compensation being given to the plaintiff, usually not involving public disclosure; 2) agree that the case for malpractice is inadequate with the result that the complaint is withdrawn (“dropped”) usually without public disclosure; and 3) disagree about whether or not malpractice has occurred, resulting in the matter being taken to court where a trial ensues.
The many evidence-based guidelines for clinical care are often improperly considered standards of care.
PATIENT SAFETY
In the Institute of Medicine report, “To Err Is Human: Building a Safer Health System in 2000,” patient safety and medical errors were noted to play a significant role in patient injury and death. As a result, patient safety and error reduction have become paramount for health care professionals and health care systems.
Definitions of Patient Safety
There are several widely distributed definitions of patient safety. The leading safety organizations and their definitions are noted below.
• The institute of Medicine: Freedom from accidental injury, ensuring patient safety, involves the establishment of operational systems and processes that minimize the likelihood of errors and maximize the likelihood of intercepting them when they occur.
• National patient Safety Foundation: The avoidance, prevention, and amelioration of adverse outcomes or injuries stemming from the processes of health care, including errors, deviations, and accidents. Safety emerges from the interactions of the components.
• Agency for Healthcare Research and Quality and the National Quality Forum: This is a type of process of structure whose application reduces the probability of adverse events resulting from exposure to the health care system across a range of diseases and procedures. Despite the seemingly various definitions of patient safety, several themes are present. These are operational systems, processes, and structures that serve to minimize the likelihood of an error. These then come together to create a culture of safety. “Achieving a culture of safety requires an understanding of the values, beliefs, and norms about what is important in an organization and what attitudes and behaviors related to patient safety are expected and appropriate” (AHRQ Publication No. 04-0041, September 2004).
Error Reduction by Consideration of Patient Safety Issues
Key components and issues of patient safety and error reduction are as follows:
• Medication errors
• Surgical errors
• Improved communication within the health care team, particularly hand-offs
• Improved communication with patients
Medication Errors
Most medical errors are associated with the use of medications. Poor or illegible handwriting, use of nonstandard abbreviations, unchecked allergies or interactions, verbal orders, and the use of a trailing zero following a decimal point when assigning doses are all major contributors to medication errors. Although computerized physician order entry systems can reduce some of the errors, attention to the above issues by the prescribing provider must occur for medication errors to decline.
Surgical Errors
Although less frequent than medical errors, surgical errors often appear more egregious. These include an incorrect operation or procedure, wrong site of surgery, or wrong patient. A rigorous and standardized preoperative verification process, which includes the patient’s participation, is designed to reduce surgical errors. Once the patient reaches the operating room, all operating room personnel participate in a “time-out” to confirm the critical aspects of the case. Patient safety is also the focus of accurate counts of surgical instruments, needles, and sponges at the end of the surgical procedure.
Improved Health Care Team Communication Hand-Offs
A hand-off, or sign-out, is the transfer of patient information from one responsible provider or team to another. Hand-offs should be interactive with the opportunity for the receiving provider/s to ask questions and clarify points of care. Using standardized medical terminology avoids errors in communication.
The setting for hand-offs must be free of distractions to enhance communication and decrease interruptions. Patient confidentiality must be maintained, and only those involved in the care of the patient should be privy to protected health care information.
The hierarchy of personnel, particularly in teaching settings, may also interfere with the transfer of important information. Every member of the health care team that is present should be encouraged to participate. The method of communication may be a significant barrier to the effective transfer of vital information. Structured forms of communication, such as the situation-background-assessment-recommendation technique, should be considered.
Critical attention to all aspects of patient hand-off is crucial to the development of a culture of safety.
Improved Communication with Patients
Establishing a partnership and creating a meaningful dialogue is paramount to the physician–patient relationship. Improving communication with patients, listening to their concerns, and facilitating active partnerships should be central to any patient safety strategy. Providers should speak slowly; use nonmedical language; and not only allow but encourage questions.
Informed consent is a process of communication—not merely a form or sheet of paper that requires a signature. With informed consent, the patient should understand her diagnosis, recommended treatment, potential complications, and treatment options. In reality, clinical decision making is a continuum with the physician leading the discussion on one end and patients making the decision on the other end.
Physicians need to inform patients how test results will be communicated, in both outpatient and inpatient locations. Lab results tracking strategies should be developed for the office and may include logbooks or computer prompts. The goal should be to communicate every test result to the patient on a timely basis. When the patient is hospitalized, the physician is obligated to use the hospital information system and inform the patient of results and their meaning when they become available.
Improved communication with patients helps strengthen the physician–patient relationship that has been shown to increase patient satisfaction, increase diagnostic accuracy, increase compliance with therapeutic recommendations, and improve quality of care.
Clinical Follow-Up
At the patient’s first visit, you determine that she does not use female vaginal hygiene products, has not changed her bathing materials including soap, and has no allergies. Her medical history is negative, including, specifically, diabetes. Her pelvic examination is negative with no discharge, lesions, etc. You perform a series of screening and diagnostic tests. Upon her return visit, you note that all the tests were negative. She again complains that the discharge continues. Your repeat pelvic examination with wet preparations is again unrewarding. Because of the association of recurrent symptoms of foul-smelling vaginal discharge without diagnosis with the possibility of sexual abuse, or perhaps even assault, you use your best empathic communication skills to probe this issue further. Initially, she is quite resistant, reminding you of her legal rights and your peril in proceeding with further unimportant questions. Although you are aware that this strongly stated request is entirely consistent with her ethical right of autonomy, you are simultaneously aware of your ethical responsibilities of beneficence, understanding the growing harm with failure to recognize an episode or episodes of sexual violence. She begrudgingly gives permission for your office counselor to join the discussion and, finally, the young lady discloses a sexual assault by a coworker after an office happy hour 3 days before the first visit to her general physician when T. vaginalis was discovered. Tearfully, she said that she had told nobody of the assault because she was ashamed that she had not taken the obvious precautions to prevent such an attack. She continues that she is sure that you are failing to find the “dirty” infection she knows she still has. You and your staff immediately begin therapy for her now recognized rape trauma syndrome, assuring her she is not at fault and supporting her desire for health. You indicate that you will remain available to her and arrange a follow-up visit, but with support she agrees to an immediate visit to a rape treatment program that your staff arranged for later in the day. You also receive permission to disclose this information to the rape trauma program and also to her general physician. She further agrees that she needs to make a police report that you know will be part of the first evaluation she will receive at the trauma center. While remaining deeply distressed, she is able to indicate some hope for the future, noting that so many people are offering help without any indication of judgment of “her behavior.”
thePoint Visit http://thepoint.lww.com/activate for an interactive USMLE-style question bank and more!
More on the topic Chapter 2 The Obstetrician– Gynecologist’s Role in Screening and Preventive Care:
- 1 Primary and Preventive Care
- Long-term health consequences in women with polycystic ovary syndrome
- Chapter 1 The Woman’s Health Examination and Women’s Health Care Management