Chapter 1 The Woman’s Health Examination and Women’s Health Care Management
This chapter deals primarily with APGO Educational Topic Areas:
TOPIC 1 HISTORY
TOPIC 2 EXAMINATION
TOPIC 3 PAP SMEAR AND DNA PROBES/CULTURE
TOPIC 4 DIAGNOSIS AND MANAGEMENT PLAN
TOPIC 5 PERSONAL INTERACTION AND COMMUNICATION SKILLS
Students should be able to refine their communication and clinical care skills to take a pertinent and comprehensive medical history, assessing risk and patient adherence to health care recommendations.
They should be able to perform a comprehensive breast and pelvic exam, including performing a Pap smear and any appropriate screening. They should be able to use these evaluations to formulate a diagnosis and management plan, while communicating to the patient important findings and recommendations, incorporating the patient’s socioeconomic and cultural context.Clinical Case
On a pleasant, rather warm summer’s day, a 72-year-old woman comes to your office with her daughter for her “annual examination.” She is pleasant, happy, and alert, dressed in a brightly colored dress matched with a heavy sweater. Your notes indicate that she uses your office for her general as well as gynecologic health care and that it has been over 7 years since her last visit. Review of her records shows a pattern of general good health with two successful term pregnancies and a postpartum tubal ligation during her twenties followed at age 38 years by a diagnostic laparoscopy for pelvic pain that revealed 18-week–sized uterine fibroids and very mild endometriosis. She subsequently had a total abdominal hysterectomy without oophorectomy, and her mild endometriosis was successfully treated with nonsteroidal anti-inflammatory medications until an unremarkable menopause at age 49 years. All previous laboratory and imaging studies were normal. She is 5 ft 8 in. tall and weighs 165 lb, and her blood pressure is 112/65 mm Hg with normal pulse, temperature, and respirations.
Her interval history and review of systems is unremarkable with the exception of often feeling cold and complaining that her skin has of late felt dryer than previously. Her physical examination is unremarkable. She asks for her sweater while waiting for her examination, complaining that she is cold and tells you she is worried about being overweight since she has gained a few pounds over the last few years. Her daughter remarks that her mother complains constantly that the temperature of her room is set too low.Obstetrics was originally a separate branch of medicine, and gynecology was a division of surgery. Over time, an increasing knowledge of the pathophysiology of the female reproductive tract led to a natural integration of these two areas, and obstetrics and gynecology merged into a single specialty. After completing an approved residency, obstetrician–gynecologists may practice general obstetrics and gynecology (nonmalignant disorders of the reproductive tract and associated organ systems and family planning). They may also choose subspecialty practice by completing fellowships in any of the four recognized subspecialty areas of obstetrics and gynecology. Maternal–fetal medicine deals with high-risk pregnancies and prenatal diagnosis. Gynecologic oncology focuses on the treatment of malignancy of the reproductive tract and associated organ systems. Reproductive endocrinology–infertility addresses problems in conception and gynecologic endocrine disease. Female pelvic medicine and reconstructive surgery (often referred to as urogynecology) deals with advanced pelvic surgery and urologic problems involving the female urogenital system. In addition, advanced and minimally invasive surgical techniques are common to all areas of obstetrics and gynecology with the role of robotic surgery also developing rapidly.
Currently, many obstetrician–gynecologists also provide nonreproductive care for women throughout their lives. Thus, obstetrician–gynecologists must have additional knowledge and skills in the primary and preventive health care needs of women and must be able to identify situations where they may provide care and those in which referral to other specialists is appropriate.
The demographics of women in the United States are undergoing profound change. A woman born today will live 81 or more years, experiencing menopause at the age of 51 to 52 years. Unlike previous generations, women will spend more than one third of their lives in menopause. The absolute number and the proportion of all women over age 65 years are projected to increase steadily through 2040 (Fig. 1.1). These women will expect to remain healthy (physically, intellectually, and sexually) throughout their lives including their “menopause years.” Physicians must keep the needs of this changing population in mind in their practice of medicine, especially in the provision of primary and preventive care in obstetrics and gynecology.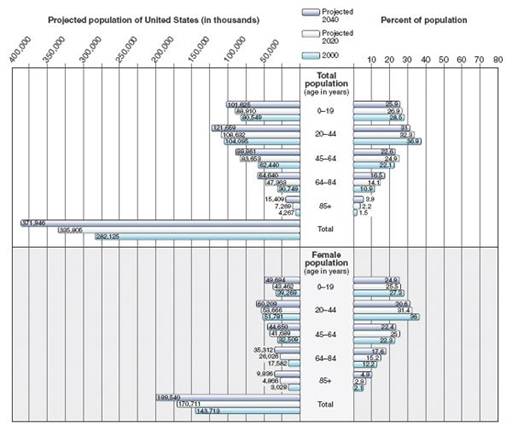
FIGURE 1.1. The U.S. population demographics. (Adapted from the U.S. Census Bureau.)
The care of women in their menopausal years will become an increasingly large part of the practice of obstetrics and gynecology in the 21st century.
Obstetrician–gynecologists must be able to establish an empathic, trusting professional relationship with patients and be able to perform a general and woman’s health history and physical examination, using this information to formulate a comprehensive management plan. Finally, obstetrician–gynecologists must fully understand the concepts of evidence-based medicine and incorporate them into their scholarship and practice in the context of a well-established pattern of lifelong learning and self-evaluation.
This chapter directly addresses the initial or “new patient visit” for gynecology and primary/preventive care as well as a first visit for obstetric care (a “new OB” visit). Subsequent return visits are generally shorter and more focused. Obtaining complete information is an essential basis of good health care. Age-appropriate health care screening as well as preventive and primary health care are discussed in Chapter 2.
An up-to-date comprehensive medical record should include information from history taking, physical examination, and laboratory and radiology testing. Information from referrals and other medical services outside the purview of the obstetrician–gynecologist should be integrated into the medical record. The American College of Obstetricians and Gynecologists (College) offers a form called the Woman’s Health Record to assist health care providers in their daily practice (Appendix A). It also includes screening recommendations and coding information.The patient encounter begins with an appropriate greeting, which deserves special attention because of the importance of initial impressions at the start of the patient–physician partnership. A handshake is commonly used. Surnames should generally be used insofar as first names are more appropriate for a friendship rather than professional relationship. A good greeting might be, “Hello Ms. Smith. I’m Dr. Jones. How may I help you today?” Or, “What brought you to the office today?”
Such a friendly but neutral greeting allows the patient to frame her response in a comfortable environment, be it a problem, a concern, or another issue.
 ESTABLISHING AN EFFECTIVE PATIENT–PHYSICIAN PARTNERSHIP
ESTABLISHING AN EFFECTIVE PATIENT–PHYSICIAN PARTNERSHIP
High-quality health care outcomes are facilitated by the use of a patient–physician partnership. Communication in which the physician demonstrates empathy and sympathy is characteristic of such a partnership. Using empathic communication skills, a physician strives to “project” himself or herself into the patient’s life and imagine the situation from the patient’s point of view. Thus, empathy goes beyond sympathy wherein the physician knows the patient’s emotions from his or her side of the partnership but does not view or feel them from the unique perspective of the patient. Empathic communication promotes the physician’s fullest understanding of the patient’s situation, which improves trust, the quality of information (and, thus, diagnostic accuracy), patient compliance with the decisions the patient and physician make, and the satisfaction of both the patient and physician.
Seemingly counterintuitively, the use of empathic communication through the patient encounter actually shortens the time of the visit because when a patient’s emotional concerns are not acknowledged by the physician, the patient will continue to make multiple attempts to express these concerns until they are addressed, often lengthening the visit in the process. Empathic communication is a learned skill that facilitates a good patient–physician partnership and the most efficient use of the time available for patient encounters.Another characteristic of the good patient–physician partnership is that the physician spends about the same amount of time listening as talking during the first two thirds of a patient visit. This kind of communication, called motivational interviewing, replaces the traditional approach of “advice giving” and gives way to “reflective listening.” The patient is encouraged to talk, and the physician actively listens, reflecting back to the patient what has been heard. Because the information gained is of better quality and the patient’s needs are met during the encounter, time-consuming “late-arising concerns” (significant issues brought up after a degree of closure has been reached on the primary problems) are less likely to occur. Building a strong and trusting patient–physician partnership is central to good women’s health care.
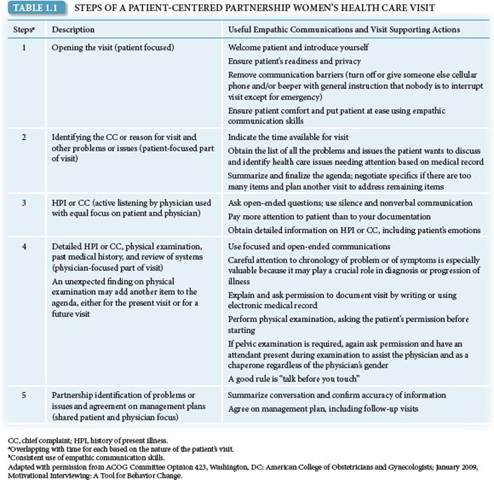
The steps of this kind of patient–physician partnership partnership and visits follow a productive pattern outlined in Table 1.1.
THE WOMAN’S HEALTH EVALUATION: HISTORY AND PHYSICAL EXAMINATION
When organized effectively, data gathered in a woman’s health evaluation is critical in facilitating patient management. Record keeping is now turning to electronic medical records, whose advantages include elimination of both transcription errors and illegible information, automated follow-up with reminders of tests and consultations, simultaneous creation of billing information, and organization and rapid availability of an entire patient’s chart.
Medical History
The medical history includes the chief complaint (CC), problem, or concern; history of present illness (HPI); a past history that includes a gynecologic history, obstetric history, family health history, and social history; and a review of system (ROS).
Chief Complaint
The CC is a concise statement describing the symptom, problem, condition, diagnosis, physician-recommended return, or other reasons for the patient visit. A CC may not be present if the patient is seeing the obstetrician–gynecologist for preventive care.
History of Present Illness
HPI is a chronologic description of the development of the patient’s CC. Establishing chronology can be important because chronological organization often suggests a specific disease or narrows consideration of illness to an organ system. Sometimes, the onset of symptoms is easily identified because of its abruptness. In other cases, the onset is insidious, making it difficult for a patient to identify a specific time. When the onset of symptoms is slow, patients are often unable to accurately identify when the symptom began. Asking in the context of a recognizable date prior to the visit (for example, a holiday) will often allow the patient to provide better chronological information. This technique may be useful in any history taking, not just for the CC.
Past History
Past history includes information about medical, surgical, or emotional diseases and/or treatments the patient has had, including the diagnosis, the medical and/or surgical treatment, and the results. Questions about previous surgery of any kind should include the name of the procedure; indication; when, where, and by whom the surgery was performed; and the results. How operative notes may contain useful information is exemplified by the issue of pelvic adhesions. A previous surgeon describing findings consistent with the effects of a pelvic inflammation should prompt the physician to ask specifically about a history of sexually transmitted diseases (STDs), such as gonorrhea, herpes, Chlamydia, genital warts (condylomata), hepatitis, acquired immune deficiency syndrome, herpes, and syphilis as well as about vaginitis and vaginal discomfort. Vaginitis and STDs are often confused. Careful history taking is needed to differentiate vaginitis or vulvitis from pelvic inflammatory disease. This can avoid delay in appropriate evaluation and treatment, which can have long-term impact on a woman’s reproductive health.
Explaining the differences while obtaining this history is an excellent opportunity to use empathic and motivational communication skills to build and enhance the patient physician partnership. The patient’s immunization history should be obtained because it may contain especially important information as worldwide travel becomes more common.
Gynecologic History
The gynecologic history includes the menstrual history, which begins with menarche, the age at which menses began. The basic menstrual history includes the following:
• Last menstrual period
• Length of periods (number of days of bleeding)
• Number of days between periods
• Any recent changes in periods
Episodes of bleeding that are “light but on time” should be noted as such, because they may have diagnostic significance. Sometimes women disregard such an episode when asked when they last had a menstrual period, so it is often useful to specifically ask if there had been any “light” bleeding, which may represent an actual ovulatory cycle. Determining a last menstrual period may be made difficult by an episode of “light vaginal bleeding.” Specific questioning is often helpful in understanding whether a woman’s last menstrual cycle was normal or abnormal. Estimation of the amount of menstrual flow can be made by asking whether the patient uses pads or tampons, how many are used during the heavy days of her flow, and whether they are soaked or just soiled when they are changed. It is normal for women to pass clots during menstruation, but normally they should not be larger than the size of a dime. Specific inquiry should be made about irregular bleeding (bleeding with no set pattern or duration), intermenstrual bleeding (bleeding between menses), and postcoital bleeding (bleeding immediately after coitus).
The menstrual history may include premenstrual symptoms, such as anxiety, fluid retention, nervousness, mood fluctuations, food cravings, variations in sexual feelings, and difficulty sleeping. Cramps and discomfort during menses are common but abnormal when they interfere with daily activities of living or when they require more analgesia than provided by non–narcotic analgesia. Menstrual pain is mediated through prostaglandins and should be responsive to nonsteroidal anti-inflammatory drugs. Inquiry about duration (both how long the patient has noted this pain and how long each episode of pain lasts), quality, radiation of the pain to areas outside the pelvis, and association with body position or daily activities completes the pain history.
The term menopause refers to the cessation of menses for greater than 1 year. Perimenopause is the time of transition from menstrual to nonmenstrual life when ovarian function begins to wane, often lasting 1 to 2 years. Significant and disruptive perimenopausal symptoms are often very disturbing and require focused attention when they are identified. Timely specific treatment is often indicated. The perimenopausal period often begins with increasing menstrual irregularity and varying or decreased flow and is associated with hot flushes, nervousness, mood changes, and decreased vaginal lubrication with sexual activity as well as altered libido (see Chapter 41).
The gynecologic history includes known gynecologic illnesses and how they were treated. The history also lists surgeries the woman has had, including what was done, why it was done, when it was done, and by whom. These details are often available by obtaining copies of the surgical dictations (operative reports), which often provide crucial diagnostic information.
The gynecologic history also includes a sexual history. Taking a sexual history is facilitated by behaviors, attitudes, and direct statements by the physician that project a nonjudgmental manner of acceptance and respect for the patient’s lifestyle. A good opening question is, “Please tell me about your sexual partner or partners.” This question is gender neutral, leaves the issue of number of partners open, and also gives the patient considerable latitude for response. However, these questions must be individualized to each patient.
Data that should be elicited in the sexual history include whether the patient is currently or ever has been sexually active, the lifetime number of sexual partners, the partners’ gender/s, and the patient’s current and past methods of contraception. A patient’s contraceptive history should include the method currently used, when it was begun, any problems or complications, and the patient’s satisfaction with the method. Previous contraceptive methods and the reasons they were discontinued may prove relevant. If no contraceptive actions are being taken, inquiry should be made as to why, which may include the desire for conception or concerns about contraceptive options as understood by the patient. Finally, patients should be asked about behaviors that put them at high risk for the acquisition of human immunodeficiency virus, hepatitis, or other sexually transmitted infections.
Obstetric History
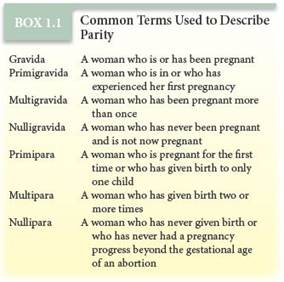
The basic obstetric history includes the patient’s gravidity, or number of pregnancies (Box 1.1). A pregnancy can end in a live birth, miscarriage, premature birth (less than 37 weeks of gestation), or an abortion. Details about each live birth are noted, including birthweight of the infant, sex, number of weeks at delivery, and type of delivery. The patient should be asked about any pregnancy complications, such as diabetes, hypertension, and preeclampsia, and whether she has a history of depression, either before or after a pregnancy. A breastfeeding history is also useful information.
If a patient has a history of infertility (generally defined as failure to conceive for 1 year with sufficiently frequent sexual encounters), questions concerning both partners should cover previous diseases or surgery that may affect fertility, pregnancy histories (previous children with the same or other partners), duration that conception has been attempted, and the frequency and timing of sexual intercourse. In older women, in the face of waning fertility, an infertility evaluation is often initiated prior to a couple’s inability to conceive for a full year.
Family History
The family history should list illnesses occurring in first-degree relatives, such as diabetes, cancer, osteoporosis, and heart diseases. Information gained from the family history may indicate a genetic predisposition for a hereditary disease. This information may guide selection of specific tests or other interventions for the surveillance of the patient and perhaps other family members.
Preconceptional Counseling and Care Preconception care can improve the outcome of pregnancy by planning conception itself as well as by identifying and managing illness before conception. This reduces the potential ill effects of preexisting illness on the mother and fetus.
Social History
Patients should be asked about behaviors and lifestyle issues that may potentially affect their health and increase their risk. The outcome of this discussion provides a meaningful basis for counseling and interventions. All patients should be asked about the following issues:
• Tobacco use
• Alcohol use: amount and type
• Use of illegal drugs and misuse of prescription drugs
• Intimate partner violence
• Bullying
• Sexual abuse
• Health hazards at work and at home; seatbelt use
• Nutrition, diet, and exercise, including folic acid and calcium intake
• Caffeine intake
Questions can also be asked about whether the patient has an advance directive and whether she is interested in organ donation.
Review of Systems
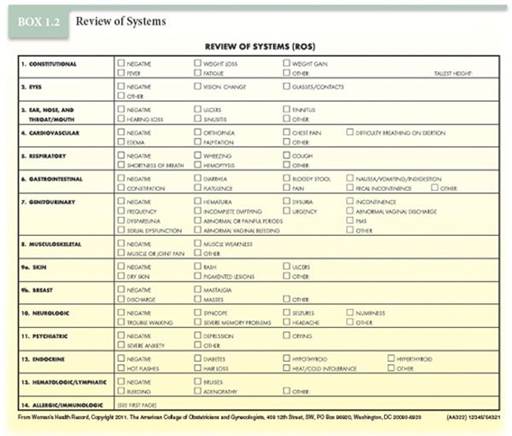
The ROS is an inventory of body systems, obtained through a series of questions, which seeks to identify symptoms that the patient has experienced or is experiencing (Box 1.2). Equally important are pertinent negatives, information derived from focused leading questions seeking the presence or absence of symptoms of illness. Pertinent negatives are often as important as positive responses in the ROS. For example, the ROS for urinary tract infection (UTI) and bladder function might include these questions, “Are you urinating more frequently than usual? How often? Does it burn when you urinate?” Increasingly frequent urination and pain with urination are often symptoms of UTI. “Do you feel you have completely emptied your bladder after you urinate? Do you lose urine accidentally when you laugh, sneeze, or cough?” These screening questions can identify problems with bladder function and pelvic support (see Chapter 30).
Physical Examination
The physical examination encompasses an evaluation of a patient’s overall health as well as a breast and gynecologic examination. The general physical examination serves to detect abnormalities suggested by the medical, surgical, or gynecologic history as well as unsuspected problems. Specific information the patient gives during the history should guide the physician to areas of physical examination that may not be surveyed in a routine screening. The extent of the examination is generally determined by the patient’s complaints, what is being medically managed by other clinicians, and what is medically indicated from history. Areas that are included in this general examination are listed in Box 1.3. Three of these are of special importance to obstetric and gynecologic care: the breast examination, the abdominal examination, and the pelvic examination. Any request for a chaperone to also attend the physical examination should be met, regardless of the physician’s sex or whether the request is made by the patient or the physician. When chaperones are present during the physical examination, the physician should provide a separate opportunity for private conversation between him or herself and the patient.
Vital Signs
Vital signs start every physical examination: temperature; pulse; blood pressure; height; weight; and a derived value, the body mass index (see Chapter 2). Prehypertension is a relatively new blood pressure category (Table 1.2). Women with prehypertension require closer evaluation, and alterations of lifestyle are advised. Because women with prehypertension are more likely to become hypertensive and have increased risk of hypertensive end-organ damage, referral to an internist or family medicine physician may be advisable.
Breast Examination
The breast examination by a physician remains the best means of early detection of breast cancer when combined with appropriately scheduled mammography. The results of the breast examination may be expressed by description or diagram, or both, usually with reference to the quadrants and tail region of the breast or by allusion to the breast as a clock face with the nipple at the center (Fig. 1.2).
The breasts are first examined by inspection, with the patient’s arms at her sides, and then with her hands pressed against her hips, and/or with her arms raised over her head (Fig. 1.3). If the patient’s breasts are especially large and pendulous, she may be asked to lean forward so that the breasts hang free of the chest, facilitating inspection. Tumors often distort the relations of these tissues, causing disruption of the shape, contour, and symmetry of the breast or position of the nipple. Some asymmetry of the breasts is common, but marked differences or recent changes deserve further evaluation.
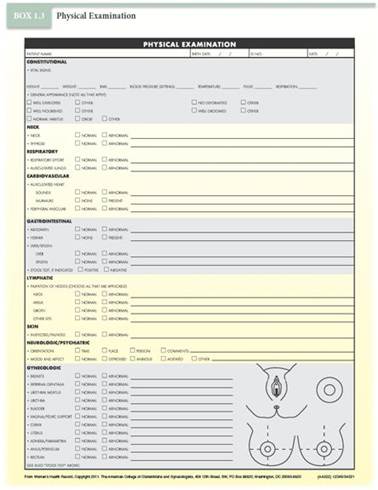
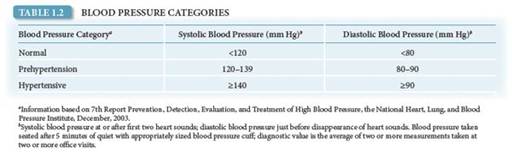
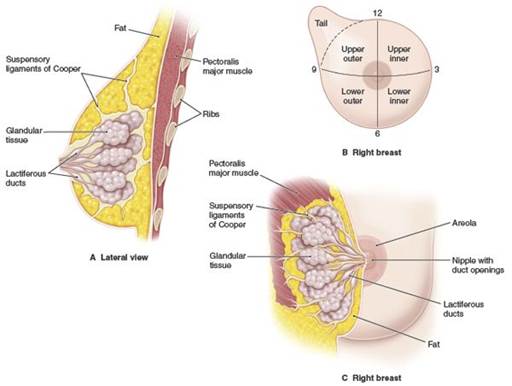
FIGURE 1.2. Clinical anatomy and associated examination schema of the breast.
Discolorations or ulcerations of the skin of the breast, areola, or nipple, or edema of the lymphatics that causes a leathery puckered appearance of the skin (referred to as peau d’orange or “like the skin of an orange”) are abnormal. A clear or milky breast discharge is usually bilateral and associated with stimulation or elevated prolactin levels (galactorrhea). Bloody discharge from the breast is abnormal and usually unilateral; it usually does not represent carcinoma, but rather inflammation of a breast structure with intraductal papilloma is often found. Evaluation is necessary to exclude malignancy. Pus usually indicates infection, although an underlying tumor may be encountered.
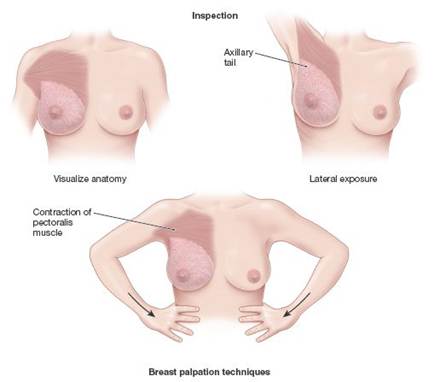
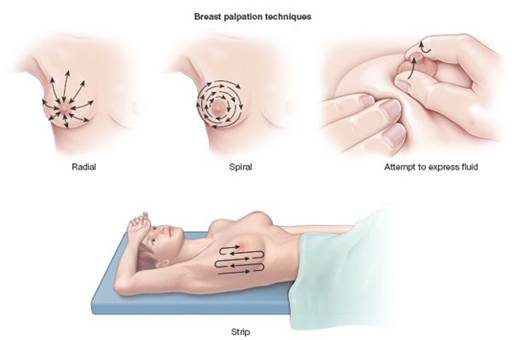
FIGURE 1.3. Breast examination. Regardless of your preferred method, accuracy is attained by systematic practice and by ensuring full coverage of the breast tissue, including the axillary tail.
Very large breasts may pull forward and downward, causing upper back pain and stooped shoulders. Disabling pain and posture are usually considered appropriate indications for insurance to cover breast reduction surgery (reduction mammoplasty).
Palpation follows inspection, first with the patient’s arms at her sides and then with the arms raised over her head. This part of the examination is usually done with the patient in the supine position. The patient may also be seated, with her arm resting on the examiner’s shoulder or over her head, for examination of the most lateral aspects of the axilla. Palpation should be done with slow, careful maneuvers, using the flat part of the fingers rather than the tips. The fingers are moved up and down in a wavelike motion, moving the tissues under them back and forth, so that any breast masses that are present can be more easily felt. The examiner should decide upon a specific pattern of examination (e.g., in spiral, radial, and longitudinal strips) and become facile with it so as to routinely include the entire breast, including the axillary tail. If masses are found, their size, shape, consistency (i.e., soft, hard, firm, and cystic), and mobility as well as their position should be determined. Women with large breasts may have a firm ridge of tissue located transversely along the lower edge of the breast. This is the inframammary ridge and is a normal finding.
The examination is concluded with gentle pressure inward and then upward at the sides of the areola to express fluid. If fluid is noted on inspection or is expressed, it should be sent for culture and sensitivity and cytopathology.
Counseling Breast Self-Awareness
Current recommendations emphasize that physicians encourage women to develop greater breast self-awareness, which may, for some women, include breast self-examination (BSE). Breast self-awareness is generally defined as a woman’s awareness of the normal appearance and feel of her breasts. The awareness of something being wrong has been shown to correlate with 50% to 70% of women subsequently being found to have breast cancer. Thus, enhanced breast self-awareness is associated with an increased likelihood of earlier detection of breast cancer.
This may be especially important for women who have had a recent “normal physician breast examination” or negative mammogram and yet actually have breast cancer. Encouraging breast self-awareness may include BSE if desired and may be of value in women at higher risk for breast cancer (e.g., first-degree relatives with breast cancer). Routine teaching of BSE is no longer generally recommended because it is associated with a high incidence of false-positive findings, leading to unnecessary testing including breast biopsy. For a woman who does request instruction in BSE, emphasis should be placed on observing her breasts in a mirror with her arms raised, looking for changes in the shape or contour of her breasts or discolorations. This is followed by gentle systematic palpation of the breasts with the flat of her fingers, including up into the armpits, wherein lies the axillary tail of the breast. Abnormal findings may include lumps, bumps, changes in breast texture, and unusual discomfort. When gentle squeezing of the nipples expresses blood or pus, this abnormal finding should be reported to the physician.
Pelvic Examination
An empty bladder is necessary for a comfortable and thorough pelvic examination. If needed, a “clean-catch” urine specimen is obtained from the mid-portion of her urinary stream after the patient has wiped her external genitals with the supplies provided. This kind of urine specimen may be used for urine culture with sensitivity testing as well as chemical testing. Abdominal and pelvic examinations require relaxation of the muscles. Techniques that help the patient to relax include encouraging the patient to breathe in through her nose and out through her mouth, gently and regularly, rather than holding her breath, and helping the patient to identify specific muscle groups (such as the abdominal wall or the pelvic floor) that need to be looser.
Communication with the patient during the examination is important. Everything that is going to happen during the pelvic examination should be explained before it occurs. Following the precept “talk before you touch” avoids anything unexpected.
An abrupt or stern command such as “Relax now; I’m not going to hurt you” may raise the patient’s fears, whereas a statement such as “Try to relax as much as you can, although I know that is a lot easier for me to say than for you to do” sends two messages: 1) that the patient needs to relax, and 2) that you recognize that it is difficult, both of which demonstrate patience and understanding. Saying something such as “Let me know if anything is uncomfortable, and I will stop and we will try to do it differently” tells the patient that there might be discomfort but that she has control and can stop the examination if discomfort occurs. Likewise, stating “I am going to touch you now” is helpful in alleviating surprises. Using these statements demonstrates that the examination is a cooperative effort, further empowering the patient in facilitating care.
Position of the Patient and Examiner
The patient is asked to sit at the edge of the examination table, and an opened draping sheet may be placed over the patient’s lap and knees. If a patient requests that a drape not be used, the request should be honored.
Positioning the patient for examination begins with the elevation of the head of the examining table to approximately 30° from horizontal. This serves three purposes: 1) it allows eye contact between the patient and physician and facilitates communication between the patient and physician during the entire examination; 2) it relaxes the abdominal wall muscle groups, making abdominal and pelvic examinations easier; and 3) it allows the physician to observe the patient for responses to the examination, which may provide valuable information (e.g., the nonverbal communication of wincing as evidence of discomfort during the abdominal and bimanual examinations). The physician or an assistant should help the patient lie back, slide down to the end of the examination table until her buttocks are at the edge of the table, place her feet in the footrests, bend her knee, and open her legs (lithotomy position) as shown in Figure 1.4. After the patient is in position, a drape may be placed over the patient’s legs and adjusted so that it does not obscure the clinician’s view of the perineum or obscure eye contact between patient and physician.

FIGURE 1.4. Lithotomy position during a pelvic examination.
The physician should sit at the foot of the examining table, with the examination lamp adjusted to shine on the perineum. The lamp is optimally positioned in front of the physician’s chest a few inches below the level of the chin, at approximately an arm’s length distance from the perineum. The physician should glove both hands. After contact with the patient, there should be minimal contact with equipment such as the lamp.
Inspection and Examination of the External Genitalia
The pelvic examination begins with the inspection and examination of the external genitalia. Inspection should include the mons pubis, labia majora, labia minora, perineum, and perianal area. Inspection continues as palpation is performed in an orderly sequence, starting with the clitoral hood, which may be pulled back to inspect the glans proper. The labia are spread laterally to allow inspection of the introitus and outer vagina. The urethral meatus and the areas of the urethra and Skene glands should be inspected. The sequence of inspection and then palpation should be included in the thorough examination of the external genitalia. The forefinger is placed an inch or so into the vagina to gently milk the urethra. A culture should be taken of any discharge from the urethral opening. The forefinger is then rotated posteriorly to palpate the area of the Bartholin glands between that finger and the thumb (Fig. 1.5).
Speculum Examination
The next step is the speculum examination. The parts of the speculum are shown in Figure 1.6. There are two types of specula in common use for the examination of adults.

FIGURE 1.5. Palpation of the Bartholin, urethral, and Skene glands. (A) Palpation of urethral and Skene glands and “milking” of urethra. (B) Palpation of Bartholin glands.

FIGURE 1.6. The vaginal speculum. (A) Parts of the vaginal speculum. (B) Types of vaginal specula.
The Pederson speculum has flat and narrow blades that barely curve on the sides. The Pederson speculum works well for most nulliparous women and for postmenopausal women with atrophic, narrowed vaginas. The Graves speculum has blades that are wider, higher, and curved on the sides; it is more appropriate for most parous women. Its wider, curved blades keep the looser vaginal walls of multiparous women separated for visualization. A Pederson speculum with extra narrow blades may be used for visualizing the cervix in pubertal girls. Selection of the correct type of speculum is a key aspect of the comfortable and complete speculum examination. The speculum should be warmed either with warm water or by holding it in the examiner’s hand. In some settings, the speculum is already stored on a heating pad. Warming the speculum is done for the comfort of the patient and to aid with insertion.
Speculum insertion should take into account the normal anatomic relations. As illustrated in Figure 1.7, by inserting the speculum along the axis of the vagina, minimal force is needed, and comfort is maximized. Until recently, the use of lubricants was avoided because of interference with cytologic interpretation, although this is less of a concern with liquid-based Pap test techniques. Situations that may require lubricant use are encountered infrequently and include examination of some prepubertal girls, some postmenopausal women, and patients with irritation or lesions of the vagina.
Most physicians find that control of pressure and movement of the speculum are facilitated by holding the speculum with the dominant hand. The speculum is held by the handle with the blades completely closed. The first two fingers of the opposite hand are placed on the perineum laterally and just below the introitus; pressure is applied downward and slightly inward until the introitus is opened slightly. If the patient is sufficiently relaxed, this downward pressure on the perineum causes the introitus to open, allowing for easier insertion of the speculum. The speculum is initially inserted in a horizontal plane with the width of the blades oblique to the vertical axis of the introitus. The speculum is then directed posteriorly at an approximately 45° angle from horizontal; the angle is adjusted as the speculum is inserted, so that the speculum slides into the vagina with minimal resistance. If the patient is not relaxed, posterior pressure from a finger inserted in the vagina sometimes relaxes the perineal musculature.

FIGURE 1.7. Speculum insertion.
As the speculum is inserted, a slight continuous downward pressure is exerted so that distension of the perineum is used to create space into which the speculum may advance. Taking advantage of the distensibility of the perineum and vagina posterior to the introitus is a crucial concept for the efficient and comfortable manipulation of the speculum examination (and later for the bimanual and rectovaginal examination). Pressure superiorly causes pain in the sensitive area of the urethra and clitoris. The speculum is inserted as far as it will go, which, in most women, means insertion of the entire speculum length. The speculum is then opened in a smooth and deliberate fashion. With slight tilting of the speculum, the cervix slides into view between the blades of the speculum. The speculum is then locked into the open position using the thumbscrew. Failure to find the cervix most commonly results from not having the speculum inserted far enough, often due to fear of causing patient discomfort. Keeping the speculum fully inserted while opening the speculum does not result in discomfort.
When the speculum is locked into position, it usually stays in place without being held. For most patients, the speculum is opened sufficiently by use of the upper thumbscrew. In some cases, however, more space is required. This may be obtained by gently expanding the vertical distance between the speculum blades by the use of the screw on the handle of the speculum. With the speculum in place, the cervix and the deep lateral vaginal vault may be inspected and specimens obtained. Before obtaining samples for the Pap test, the patient should be told that she may feel a slight “scraping” sensation but no pain. Specimens are collected to fully evaluate the transformation zone, where cervical intraepithelial neoplasia is more likely to be encountered. Specimens are obtained from the exocervix and endocervix and either plated on slides, which are immediately fixed with a preservative spray, or placed in a liquid collection medium (Fig. 1.8).
Speculum withdrawal also allows for inspection of the vaginal walls. After telling the patient that the speculum is to be removed, the blades of the speculum are opened slightly by putting pressure on the thumb hinge, and the thumbscrew is completely loosened. Opening the speculum blades slightly before starting to withdraw the speculum avoids pinching the cervix between the blades. The speculum is withdrawn approximately 1 in. before pressure on the thumb hinge is slowly released. The speculum is withdrawn slowly enough to allow inspection of the vaginal walls. The blades of the speculum are naturally brought together by vaginal wall pressure. As the end of the speculum blades approaches the introitus, there should be no pressure on the thumb hinge, as otherwise the anterior blade can flip up, hitting the sensitive vaginal, urethral, and clitoral tissues.
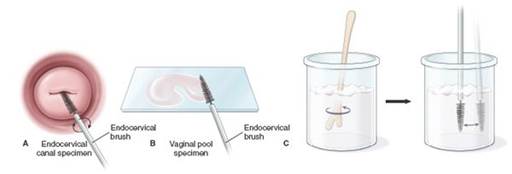
FIGURE 1.8. Pap smear collection. (A) Obtaining endocervical portion of Pap smear. (B) Spread specimen before fixation within 10 seconds. (C) Placement of specimens in liquid collection medium.
Bimanual Examination
The bimanual examination uses both a “vaginal” hand and an “abdominal” hand to entrap and palpate the pelvic organs. The bimanual examination begins by exerting gentle pressure on the abdomen approximately halfway between the umbilicus and the pubic hair line with the abdominal hand, while inserting the index and middle fingers of the vaginal hand into the vagina to approximately 2 in. and gently pushing downward, distending the vaginal canal. The patient is asked to feel the muscles being pushed on and to relax them as much as possible. Then both the index and middle fingers are advanced into the vagina until they rest at the limit of the vaginal vault in the posterior fornix behind and below the cervix. A great deal of space may be created by posterior distension of the perineum. Occasionally, only the index finger of the vaginal hand can be comfortably inserted.
During the bimanual examination, the pelvic structures are “caught” and palpated between the abdominal and vaginal hands. Whether to use the dominant hand as the abdominal or vaginal hand is a question of personal preference. A common error in this part of the pelvic examination is failure to make effective use of the abdominal hand. Pressure should be applied with the flat part of the fingers, not the fingertips, starting midway between the umbilicus and the hairline, moving downward in conjunction with upward movements of the vaginal hand. The bimanual examination continues with the circumferential examination of the cervix for its size, shape, position, mobility, and the presence or absence of tenderness or mass lesions (Fig. 1.9).

FIGURE 1.9. Bimanual examination of the uterus and adnexa.
Bimanual examination of the uterus is accomplished by lifting the uterus up toward the abdominal fingers so that it may be palpated between the vaginal and abdominal hands. The uterus is evaluated for its size, shape, consistency, configuration, and mobility; for masses or tenderness; and for position. The uterus may tilt on its long axis (from cervix to fundus, version) yielding three positions (anteverted, midposition, and retroverted). It may also tilt on a shorter axis (from just above or at the area of the lower uterine segment, flexion) yielding two positions (anteflexed and retroflexed) (see Fig. 4.12). The retroverted, retroflexed uterus has three particular clinical associations: 1) it is especially difficult to estimate gestational age by bimanual examination, 2) it is associated with dyspareunia and dysmenorrhea, and 3) its position behind and below the sacral promontory may lead to the obstetric complication of uterine inculcation. Cervical position is often related to uterine position. A posterior cervix is often associated with an anteverted or midposition uterus, whereas an anterior cervix is often associated with a retroverted uterus. Sharp flexion of the uterus, however, may alter these relations.
The bimanual examination technique varies somewhat with the position of the uterus. Examination of the anterior and midposition uterus is facilitated with the vaginal fingers lateral and deep to the cervix in the posterior fornix. The uterus is gently lifted upward to the abdominal fingers and a gentle side-to-side “searching” motion of the vaginal fingers is combined with steady pressure and palpation by the abdominal hand to determine the characteristics of the uterus.
Examination of the retroverted uterus may be more difficult. In some cases, the vaginal fingers may be slowly pushed below or at the level of the uterine fundus, after which gentle pressure exerted inward and upward causes the uterus to antevert, or at least to move “upward,” somewhat facilitating palpation. Then, palpation is accomplished as in the normally anteverted uterus. If this cannot be done, a waving motion with the vaginal fingers in the posterior fornix must be combined with an extensive rectovaginal examination to assess the retroverted uterus.
Bimanual examination of the adnexa to assess the ovaries, fallopian tubes, and support structures begins by placing the vaginal fingers to the side of the cervix, deep in the lateral fornix. The abdominal hand is moved to the same side, just inside the flare of the sacral arch and above the pubic hairline. Pressure is then applied downward and toward the symphysis with the abdominal hand, at the same time lifting upward with the vaginal fingers. The same movements of the fingers of both hands used to assess the uterus are used to assess the adnexal structures, which are brought between the fingers by these maneuvers to evaluate their size, shape, consistency, configuration, mobility, and tenderness as well as to palpate for masses. Special care must be taken when examining the ovaries, which are sensitive even in the absence of pathology. The ovaries are palpable in normal menstrual women approximately half of the time, whereas palpation of ovaries in postmenopausal women is less common.
Rectovaginal Examination
When indicated, a rectovaginal examination forms part of the complete pelvic examination on initial and annual examination as well as at interval examinations whenever clinically indicated (e.g., when there is suspicion of a posterior pelvic mass or in the evaluation of chronic pelvic pain).
The rectovaginal examination is begun by changing the glove on the vaginal hand and using a liberal supply of lubricant. The examination may be comfortably performed if the natural inclination of the rectal canal is followed: upward at a 45° angle for approximately 1 to 2 cm, then downward (Fig. 1.10). This is accomplished by positioning the fingers of the vaginal hand as for the bimanual examination, except that the index finger is also flexed. The middle finger is then gently inserted through the rectal opening and inserted to the “bend” where the angle turns downward. The index (vaginal) finger is inserted into the vagina, and both fingers are inserted until the vaginal finger rests in the posterior fornix below the cervix, and the rectal finger rests as far as it can go into the rectal canal. Asking the patient to bear down as the rectal finger is inserted is not necessary and may add to the tension of the patient. Palpation of the pelvic structures is then accomplished, as in their vaginal palpation. The uterosacral ligaments are also palpated to determine if they are symmetrical, smooth, and nontender (as normally) or if they are nodular, slack, or thickened. The rectal canal is evaluated, as are the integrity and function of the rectal sphincter. After palpation is complete, the fingers are rapidly but steadily removed in a reversal of the sequence of movements used on insertion. Care should be taken to avoid contamination of the vagina with fecal matter.

FIGURE 1.10. Rectovaginal examination.
At the conclusion of the pelvic examination, the patient is asked to move back up on the table and, thereafter, to sit up.
 DIAGNOSIS, MANAGEMENT, AND CONTINUITY OF CARE
DIAGNOSIS, MANAGEMENT, AND CONTINUITY OF CARE
Depending on the reason for the patient’s visit—either for a specific medical problem or for a preventive examination, further assessments and management plans are established. If a problem exists, the history and physical findings help establish a differential diagnosis (i.e., a list of possible underlying causes of the problem). Tests are ordered to try to further identify the most likely diagnosis. A presumptive diagnosis is made, and a management plan agreed upon between the patient and physician. Amelioration of symptoms and other evidence of treatment success confirm the diagnosis. If unsuccessful, the physician is led to further evaluation and consideration of new management plans.
If the patient has had a preventive health care examination, issues that arise during the history and physical examination and a long-term plan for addressing these issues should be discussed. The patient and physician agree on a plan of action, which may include behavior modification, lifestyle modification, referral to another physician or health care or social services professional, or referral to community resources including the possible use of faith resources. Screening tests and immunizations that are appropriate for the patient should also be administered (see Chapter 2).
Clinical Follow-Up
You assure her of her good general health and recommend age-appropriate screening examinations. Discussion of her weight using height and weight tables does not initially reassure her, but she is more reassured after an explanation of her normal calculated body mass index and how it is more accurate in evaluating her weight. You perform the standard screening examinations she should have had by her age, including complete blood count, metabolic panel with lipids, and thyroid-stimulating hormone (TSH) as well as mammogram and bone density studies, and express the hope that you may be able to help with her constantly feeling cold. Subsequently, her overdue TSH is found to be significantly elevated. With thyroid hormone replacement, much of her sensation of feeling cold resolves over the next few months with a commensurate improvement in the quality of her life.
thePoint Visit http://thepoint.lww.com/activate for an interactive USMLE-style question bank and more!