1 Primary and Preventive Care
Hannah Anastasio
Silka Patel
Obstetrician-gynecologists are in a unique position to interact with women across the reproductive and age spectrum and are seen by many patients as the sole provider of primary and preventive health care.
The responsibilities of a primary care physician include screening and treatment of selected diseases, counseling, and providing immunizations. Additionally, common nongynecologic conditions that the obstetrician-gynecologist (ObGyn) should be familiar with include asthma, allergic rhinitis, respiratory tract infections, gastrointestinal disorders, urinary tract disorders, headache, low back pain, and skin disorders.SCREENING AND TREATMENT
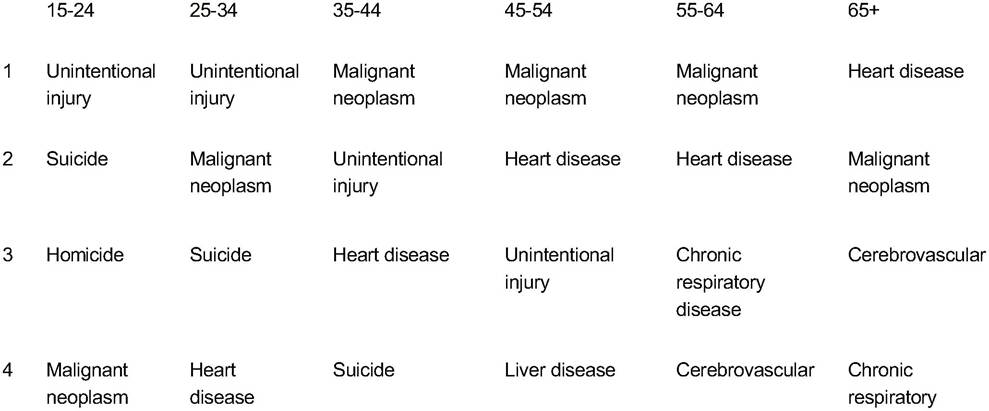
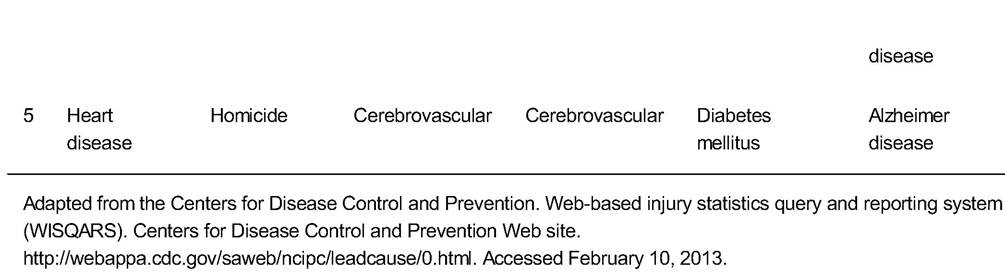
• The majority of deaths among women younger than the age of 65 years are preventable or have modifiable risk factors (Table 1-1).
• Primary prevention is identification and control of risk factors before disease occurs
• Secondary prevention is early diagnosis of disease to reduce morbidity/mortality
• A condition which is a good target for screening should have the following:
• A significant effect on the quality and quantity of life
• An acceptable and available treatment
• An asymptomatic period during which detection and treatment significantly reduce the risk for morbidity and mortality
• An incidence sufficient to justify the cost of the screening
• An asymptomatic phase during which treatment yields therapeutic results superior to those obtained by delaying treatment until symptoms develop
• The screening test should be:
• Acceptable to patients and available at a reasonable cost
• Reasonably accurate with acceptable sensitivity and specificity
î Test sensitivity: percentage of patients with the disease who test positive
î Test specificity: percentage of patients without disease who test negative
P.2
TABLE 1-1 Leading Causes of Death among Females of All Races in the United States (2010)
P.3
CANCER
Screening for Breast Cancer
• See Chapter 2.
• Breast cancer is the most common cancer in women, with a lifetime incidence of 12%. For those at average risk, the American College of Obstetricians and Gynecologists (ACOG), the American Cancer Society (ACS), and the National Comprehensive Cancer Network (NCCN) recommend routine mammography annually beginning at age 40 years. The U.S. Preventive Services Task Force (USPSTF), in contrast, recommends biennial screening between ages 50 and 74 years. In addition, ACOG recommends regular clinical breast examinations in all women as well as breast self-examination in high-risk women.
• ACOG and the Society of Gynecologic Oncology recommend referral for genetic counseling and BRCA testing in patients with 20% or greater chance of having an inherited predisposition to developing breast or ovarian cancer. This includes women with the following family history:
• Women with a personal history of both breast and ovarian cancer
• Women with ovarian cancer and a close relative with ovarian cancer or premenopausal breast cancer
• Women with breast cancer at age 50 years or younger as well as either a close relative with ovarian cancer or breast cancer in a man at any age
• Women of Ashkenazi Jewish ancestry with a diagnosis of breast cancer at age 40 years or younger or with ovarian cancer at any age
• Women with close relative with known BRCA1 or BRCA2 mutation
• Additionally, further genetic risk assessment may be helpful in the following women (estimated to have between 5% and 10% risk of having an inherited predisposition toward developing breast or ovarian cancer):
• Breast cancer at age 40 years or younger
• Primary peritoneal, ovarian, or fallopian tube cancer at any age
• Breast cancer at age 50 years or younger and a close relative with breast cancer at age 50 years or younger
• Ashkenazi Jewish ancestry with breast cancer at or before age 50 years
• Breast cancer at any age in addition to two close relatives with breast cancer (any age)
• Unaffected women with a close relative that meets any of the previous criteria
• Women at high risk for breast cancer, such as those with BRCA1 or BRCA2 mutations, may undergo prophylactic mastectomies to reduce their risk of breast cancer.
Screening for Lung Cancer
• Lung cancer, the second most common cancer in women, is the leading cause of cancer-related death. In 2009, in the United States, 95,784 women were diagnosed and 70,387 died from lung cancer.
• Risk factors include cigarette smoking (associated with 90% of lung cancers), radiation therapy, environmental toxins such as asbestos, and pulmonary fibrosis.
• The majority of studies examining screening modalities for lung cancer (via chest x-ray, sputum cytology, or computed tomography [CT] scan) have failed to show a mortality benefit from early detection of lung cancer. In 2011, the National Lung Screening T rial was the first to show approximately a 20% mortality benefit in asymptomatic heavy smokers (>30 pack-year history) screened with low-dose CT scans. The 2013 ACS recommendation (in abstract form) is that providers discuss lung cancer screening with a low-dose helical CT of the chest for patients between
P.4 ages 55 and 74 years with at least a 30 pack-year smoking history. At this time, the recommendation is that providers and patients have an informed discussion about the current data regarding lung cancer screening and use shared decision making to decide whether to initiate lung cancer screening.
• Smoking may confer a greater relative risk for women than men; however, many of the early studies on lung cancer screening did not include women. It is theorized that screening in women may have different outcomes due to higher rates of peripherally located adenocarcinoma.
• Smoking cessation, as well as continued abstinence in nonsmokers, is the single most important modifiable risk factor for lung cancer.
Screening for Colorectal Cancer
• Colorectal cancer is the third most commonly diagnosed cancer and the third leading cause of cancer in women, with an annual incidence of 38.9 per 100,000. Most colorectal cancers have a long latency period and are curable or easily treatable if detected at an early stage.
• Risk factors include a family history of colorectal cancer, a personal history of colon polyps or cancer, a personal history of inflammatory bowel disease, and the genetic syndromes familial adenomatous polyposis and hereditary nonpolyposis colon cancer (HNPCC).
High-risk individuals should be screened with colonoscopy beginning at earlier ages depending on risk.• Women with a diagnosis of HNPCC should initiate screening at age 20 to 25 years or 10 years before the youngest age of colon cancer diagnosis in the family.
• The USPSTF recommends screening for colorectal cancer for all persons aged 50 years and older. The American College of Gastroenterology recommends beginning screening at age 45 years in African Americans due to higher incidence and earlier age of onset.
• Many screening protocols exist, including flexible sigmoidoscopy every 5 years, colonoscopy every 10 years, double-contrast barium enema every 5 years, CT colonography every 5 years, guaiac-based fecal occult blood test annually (two samples from each of three consecutive stools), fecal immunochemical test annually, and stool DNA test. The 2008 U.S. Multi-Society Task Force on Colorectal Cancer guidelines support any of the aforementioned regimens; ACOG encourages colonoscopy but ultimately recommends shared decision making to determine which screening modality the patient is most likely to comply with.
Screening for Endometrial Cancer
• See Chapter 47.
• No routine screening is recommended for asymptomatic women. Certain highrisk groups (those with known or prior endometrial hyperplasia or patients with HNPCC) may undergo screening, such as endometrial biopsy, pelvic ultrasound, dilation and curettage, or a combination of these. All episodes of postmenopausal bleeding should be investigated. Additionally, in premenopausal obese women with a significant change in bleeding pattern, endometrial sampling should be considered.
Screening for Skin Cancer
• Melanoma is the seventh leading cancer in women; risk factors include light skin tone and ultraviolet ray exposure, particularly childhood sunburns. People with between 50 and 100 typical nevi or large congenital nevi are also at increased risk (relative risk of 5 to 17 and >100, respectively).
P.5
• Although there are no consensus guidelines for total skin examination, ACOG recommends evaluation in those patients at high risk. All patients should be educated regarding sunscreen use and ultraviolet ray avoidance. In particular, all atypical vulvar lesions should be thoroughly investigated (see Chapter 44.)
• Guidelines regarding suspicious lesions are as follows:
• Asymmetry
• Border irregularities
• Color variegation
• Diameter >6 mm
• EnlargementZEvolution of color change, shape, or symptoms
Screening for Ovarian Cancer
• See Chapter 48.
• No North American expert group recommends routine screening for ovarian cancer. Instead, a careful family history and an annual pelvic exam are recommended for all women.
• Women at high risk for ovarian cancer, such as those with BRCA1 or BRCA2 mutations, may undergo prophylactic bilateral salpingo-oophorectomy to reduce their risk of ovarian cancer.
Screening for Cervical Cancer
• See Chapter 46.
• Routine screening for cervical cancer with either liquid-based or conventional Papanicolaou (Pap) testing is recommended starting at age 21 years, regardless of age of first sexual activity. The ACS and ACOG have suggested that women between the ages of 21 and 30 years should be screened with cytology alone every 3 years, provided the patient does not have a history of cervical intraepithelial neoplasia grade 2 (CIN 2) or worse, is not HIV positive or immunocompromised, and has no history of diethylstilbestrol exposure. Routine human papillomavirus (HPV) testing is not recommended in this age group given the high incidence of transient asymptomatic infection. Women ages 30 to 65 years should be screened every 5 years with cotesting (cytology and HPV testing). Alternatively, Pap screening with cytology alone (without HPV testing) every 3 years may be performed, but cotesting is preferable. After age 65 years, no further screening is recommended if the patient has had adequate negative screening for the past 10 years.
Women with prior loop electrosurgical excision procedure/cryotherapy should continue agebased screening for at least 20 years from procedure.• ACOG and the USPSTF both agree that cervical cancer screening may be discontinued for women who have had a total hysterectomy for benign indications and no history of CIN 2 or worse.
• Women with abnormal Pap smears should be managed per the American Society for Colposcopy and Cervical Pathology guidelines.
• There are currently two U.S. Food and Drug Administration-approved vaccines for the primary prevention of cervical cancer. Cervarix protects against high-risk HPV strains 16 and 18 known to cause cervical cancer, and Gardasil protects against HPV 6, 11, 16 and 18 conferring additional benefit against HPV strains known to cause genital warts. ACOG recommends universal vaccination of women against these HPV strains before initiation of sexual activity (as early as age 9 years) as well as in sexually active women up to age 26 years. Women who have received HPV vaccination should be screened for cervical cancer using the same schedule as unvaccinated women.
P.6
HEART AND VASCULAR CONDITIONS
Screening for Coronary Heart Disease
• Rates of coronary heart disease (CHD) in women increase with age, ranging between 5% and 15%. Risk factors include hypertension, dyslipidemia, diabetes, smoking, and family history of premature CHD (age risk of a CHD event. The Framingham model was updated by the National Cholesterol Education Program (NCEP) Adult T reatment Panel III (ATP III) and adjusts for the following variables: age, gender, low-density lipoprotein cholesterol, high-density lipoprotein (HDL) cholesterol, blood pressure, diabetes, and smoking. The USPSTF recommends against routine screening of asymptomatic low-risk patients (defined as 45 years if they are at increased risk of CHD (level A evidence). Screening of highrisk women aged 20 to 45 years is recommended (level B evidence), and screening of low-risk women is neither recommended nor discouraged (level C evidence). Recommended screening interval is every 5 years, but a shorter interval should be considered in patients at increased risk for dyslipidemia or with previous borderline results.
• Table 1-2 summarizes NCEP/ATP III treatment recommendations. Goal cholesterol level depends on number and severity of risk factors for CHD. CHD equivalents include peripheral arterial disease, abdominal aortic aneurysm, diabetes mellitus, and symptomatic carotid artery disease. Other risk factors (non-CHD equivalents) include smoking, hypertension (>140/90 mm Hg or requiring antihypertensive), low HDL (45 years, women >55 years).
• Lifestyle changes include limiting fat intake (particularly trans and saturated fat), increasing dietary fiber and plant sterol intake, weight loss, and increasing physical activity.
• The most commonly used pharmacologic treatment for dyslipidemia include bile acid-binding resins, statins, nicotinic acid, fibric acid derivatives, and cholesterol absorption inhibitors. Treatment choice depends on the particular lipid profile; however, statins are the drug of choice for cardioprotection.
Screening for Hypertension
• Hypertension (defined as blood pressure >140/90 mm Hg or requiring antihypertensive medication) is a leading risk factor for CHD, congestive heart failure,
P.7 stroke, ruptured aortic aneurysm, renal disease, and retinopathy. Suboptimal blood pressure has been reported as the number one risk factor for death worldwide.
TABLE 1-2 NCEP/ATP III Cholesterol Treatment Guidelines (2002)
| Risk Group | LDL Goal (mg/dL) | LDL Level to Start Lifestyle Changes (mg/dL) | LDL Level to Start Drug Therapy (mg/dL) |
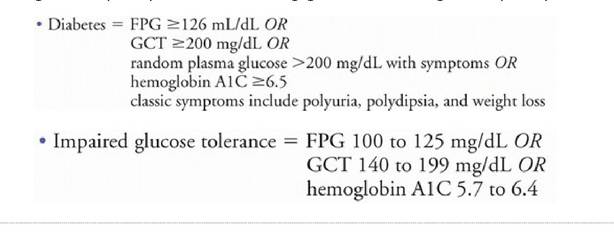
| CHD or risk equivalent | in firstdegree relative, non-Caucasian ethnicity, history of gestational diabetes or delivering a baby >9 pounds, inactivity, dyslipidemia, polycystic ovarian syndrome, and vascular disease. • Screening tests: fasting plasma glucose (FPG) or a 2-hour, 75-g glucose challenge test (GCT), and hemoglobin A1C.
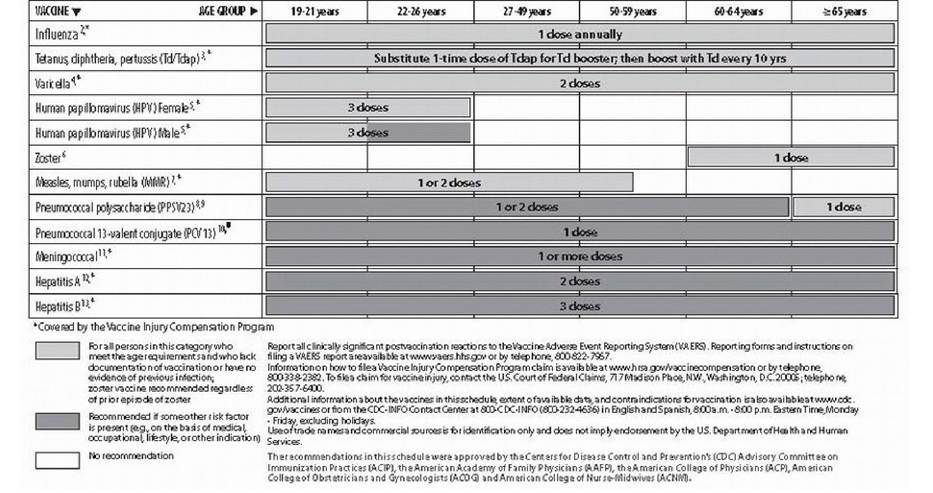
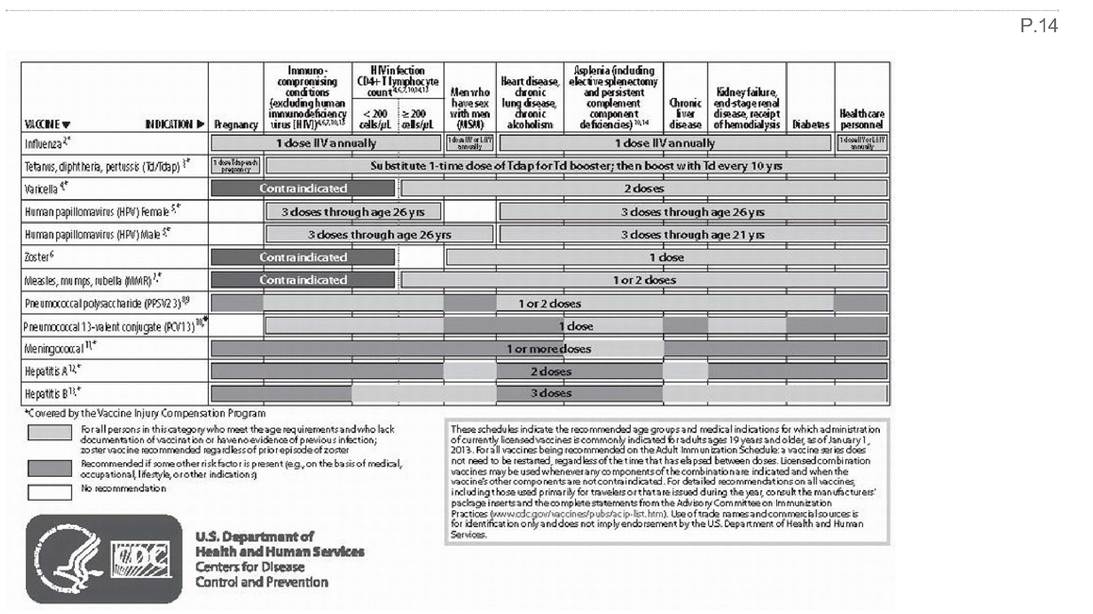
• Patients with impaired glucose tolerance should be referred for counseling on weight loss, diet, and exercise; medical therapy may be initiated in high-risk obese patients. • Upon diagnosis of diabetes, screening should be performed to evaluate for retinopathy, nephropathy, neuropathy, CHD, cerebrovascular disease, peripheral artery disease, and dental disease. Screening for Thyroid Disorders • See Chapter 13. • The USPSTF does not recommend screening asymptomatic people for hypothyroidism. ACOG recommends screening women older than 50 years with thyroidstimulating hormone levels every 5 years. This should also be considered in younger patients with autoimmune disease or strong family history of thyroid disease. Counseling on Nutrition • The 2010 United States Department of Agriculture Dietary Guidelines recommend consumption of a variety of nutrient-dense foods and beverages (such as fruits, vegetables, whole grains, and fat-free or low-fat dairy products and seafood). Additionally, they recommend limiting the intake of saturated and trans fats, sodium, cholesterol, added sugars, and refined grains. Specific recommendations include: • Adults older than age 50 years should consume supplemental vitamin B12 either in the form of fortified foods or dietary supplements. • Pregnant women and women of childbearing age should consume foods high in iron and folic acid. At least 400 μg of supplemental folic acid per day is recommended in women capable of or considering becoming pregnant. Preferably, ironrich foods should be taken with vitamin C to enhance absorption. • Older adults, people with darker skin tones, and those with minimal exposure to sunlight should consume at least 600 to 800 IU/day of supplemental vitamin D. Recommended daily for postmenopausal women is 1,200 mg of calcium, either in the form of calcium-rich foods or dietary supplements. • Estimated caloric requirement for nonpregnant adult women varies between 1,800 and 2,400 kcal based on level of activity. Counseling on Obesity • The 2007-2008 National Health and Nutrition Examination Survey reported that 35.5% of adult women are obese (body mass index [BMI] ≥30 kg/m2). It is estimated that 64.1% of American women are either overweight (BMI ≥25 kg/m2) or obese. • Obesity is associated with an increased risk of morbidity including type 2 diabetes, hypertension, infertility, heart disease, gallbladder disease, uterine cancer, and colon cancer. • Screening for obesity should include calculation of BMI, measurement of waist circumference, and evaluation of overall risk due to comorbid conditions. • BMI is a measure of obesity which correlates with body fat content. • Underweight = BMI Health maintenance visits should include assessment for domestic violence using direct interview, patient questionnaires, or both (preferably while the patient is alone). Screening and Counseling for Substance Abuse • The 2011 National Survey on Drug Use and Health found that 8% of Americans use illicit drugs, 27% engage in binge drinking, and 28% use tobacco products. • All patients should be questioned on substance abuse; a number of screening tools exist (e.g., the CAGE questions, AUDIT-C, TWEAK, and CRAFFT questionnaires). • The CAGE questionnaire has been shown to lack sensitivity among women and minorities. Therefore, ACOG recommends modified version, the TACE questionnaire, with a positive screen being 2 or more points: • Tolerance: How many drinks does it take to feel high? (more than two drinks = 2 points) • Annoyed: Have people annoyed you by criticizing your drinking? (positive response = 1 point) • Cut down: Have you ever felt you ought to cut down your drinking? (positive response = 1 point) • Eye opener: Have you ever had a drink first thing in the morning to steady your nerves or get rid of a hangover? (positive response = 1 point) • The USPSTF recommends counseling for reducing alcohol abuse; brief 15-minute counseling interventions have been shown to reduce hazardous drinking. • The USPSTF strongly recommends screening for tobacco use and counseling for cessation as it has been shown that 1 to 3 minutes of counseling significantly increases abstinence rates. • Medical interventions include nicotine replacement therapy, bupropion, and varenicline. COUNSELING • The routine health maintenance visit is an ideal time to counsel patients regarding many health-related behaviors. • Several techniques for brief physician counseling have been developed, including the five a’s model: • Assess for problem. • Advise making a change. • Agree on action to be taken. • Assist with self-care support to make the change. • Arrange follow-up to support the change. • It is important to recognize a patient's state of readiness, as an estimated 80% of people are unprepared to commit to a lifestyle change at initial encounter. The Stages of Change Model includes the following: • Precontemplation: no intention of changing behavior. Goal of counseling = introduce ambivalence. • Contemplation: considering making a change. Goal of counseling = explore both sides of the patient's attitude and help resolve behavior. • Preparation: resolved to make a change. Goal of counseling = identify successful strategies for change. • Action: making a change in behavior. Goal of counseling = provide solutions to deal with specific relapse triggers. • Maintenance: committed to change. Goal of counseling = solidify the patient's commitment to a continued change. IMMUNIZATIONS Immunizations are an integral component of primary and preventive health care. A patient's vaccination history should be reviewed at regular intervals and updated as appropriate (see Figs. 1-1 and 1-2). OTHER PRIMARY CARE PROBLEMS • Urinary tract infections: For uncomplicated cystitis, a 3-day course of trimethoprim-sulfamethoxazole is generally the first-line recommendation. Alternatives include fluoroquinolones or nitrofurantoin. Empiric antibiotic treatment without urine culture is appropriate in the nongravid patient if the patient displays dysuria and has urine leukocytes and nitrites present on urinalysis. The presence of fever or costovertebral angle tenderness is suggestive of an upper tract infection which requires more aggressive treatment. See Chapter 16. • Upper respiratory infections: Typically viral in origin, mild upper respiratory infections should be treated supportively with rest, hydration, humidifier, and overthe-counter pharmacologic interventions (cough suppressants and decongestants). Antibiotics are not recommended as first line for treatment of uncomplicated upper respiratory illnesses. The presence of secondary bacterial infection is suggested by persistence of rhinosinusitis symptoms for 7 to 10 days and purulent nasal discharge, unilateral tooth, facial or maxillary sinus pain, or worsening symptoms after initial improvement. Patients with severe pain, fever, and failure of improvement after a period of observation should be treated with narrow-spectrum antibiotics such as amoxicillin, trimethoprim-sulfamethoxazole, or a macrolide for 10 to 14 days. See Chapter 15. Recommended Adult Immunization Schedule—United States -2013 Note:ThdsQrdcommondatIons must Bdrdadvzlththdfootnotdsthat follow containing number of doses, Intervals BdtvzeQn doses, a nd Qtherlmportant Information.
Figure 1-1. Recommended U.S. adult immunization schedule by vaccine and age group, 2013. (Adapted from Centers for Disease Control and Prevention. Recommended U.S. adult immunization schedule by vaccine and age group, 2013. Centers for Disease Control and Prevention Web site. http://www.cdc.gov/vaccines/schedules/index.html. Accessed February 10, 2013.)
Figure 1-2. Recommended vaccinations indicated for adults based on medical and other indications schedule, 2013. (Adapted from Centers for Disease Control and Prevention. Recommended U.S. adult immunization schedule by vaccine and age group, 2013. Centers for Disease Control and Prevention Web site. http://www.cdc.gov/vaccines/schedules/index.html. Accessed February 10, 2013.) P.15 Asthma: In addition to monitoring lung function and reducing exposure to triggers, pharmacologic treatment is conducted in a stepwise fashion. Mild intermittent asthma may be treated with quick-acting inhaled beta-agonists such as albuterol. For mild persistent asthma, add a low-dose inhaled glucocorticoid or leukotriene blocker. Patients with moderate persistent asthma may be treated with medium-dose inhaled glucocorticoid plus long-acting inhaled beta-agonist or a high-dose inhaled glucocorticoid. Severe, acute asthma exacerbations may necessitate oral or intravenous corticosteroids or inpatient admission. In addition to vital signs and physical examination, measurement of peak flow can help direct changes in pharmacologic therapy in patients with asthma. Patients with severe asthma should be referred to a pulmonologist or allergist for further management. See Chapter 15. SUGGESTED READINGS American College of Obstetricians and Gynecologists. Practice bulletin no. 122: breast cancer screening. Obstet Gynecol 2011;118:372-382. American College of Obstetricians and Gynecologists Committee on Gynecologic Practice. Committee opinion no. 482: colonoscopy and colorectal cancer screening strategies. Obstet Gynecol 2011;177:766-771. American College of Obstetricians and Gynecologists Committee on Gynecologic Practice. Committee opinion no. 534: wellwoman visit. Obstet Gynecol 2012;120:421-424. American College of Obstetricians and Gynecologists Committee on Practice Bulletins— Gynecology. ACOG practice bulletin number 129: osteoporosis. Obstet Gynecol 2012;120:718-734. American College of Obstetricians and Gynecologists; Society of Gynecologic Oncologists. ACOG practice bulletin no. 103: hereditary breast and ovarian cancer syndrome. Obstet Gynecol 2009;113:957-966. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2012;35(suppl 1):S64-S71. American Gastroenterological Association. American Gastroenterological Association medical position statement on obesity. Gastroenterology 2002;123:879. Centers for Disease Control and Prevention web site: http://www.cdc.gov/. Accessed February 10, 2013. Chobanian AV, Bakris GL, Black HR, et al. The seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. JAMA 2003;289:2560-2572. Flegal KM, Carroll MD, Ogden CL, et al. Prevalence and trends in obesity among US adults, 1999-2008. JAMA 2010;303(3):235-241. Levin B, Lieberman DA, McFarland B, et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. Gastroenterology 2008;134(5):1570-1595. National Cholesterol Education Program Expert Panel on Detection, Evaluation, and T reatment of High Blood Cholesterol in Adults (Adult T reatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult T reatment Panel III) final report. Circulation 2002;106(25):3143-3421. U.S. Department of Health and Human Services, Agency for Healthcare Research and Quality. U.S. Preventive Services Task Force (USPSTF): an introduction. Agency for Healthcare Research and Quality Web site. http://www.ahrq.gov/professionals/clinicians-providers/guidelines-recommendations/uspstf/index.html. Accessed February 10, 2013. U.S. Department of Health and Human Services; U.S. Department of Agriculture. Dietary Guidelines for Americans, 2010. 7th ed. Washington, DC: U.S. Government Printing Office. http://www.dietaryguidelines.gov. Accessed February 10, 2013. Wender R, Fontham ET, Barrera E Jr, et al. American Cancer Society lung cancer screening guidelines. CA Cancer J Clin 2013;63(2):107-117. World Health Organization Collaborating Centre for Metabolic Bone Diseases. WHO Fracture Risk Assessment Tool (FRAX). World Health Organization Collaborating Centre for Metabolic Bone Diseases Web site. http://www.shef.ac.uk/FRAX/tool.jsp. Accessed February 10, 2013.
More medical literature on Medic.Studio
More on the topic 1 Primary and Preventive Care:
-
Infectious diseases -
Internal diseases -
Obstetrics and Gynaecology -
Pediatrics -
Veterinary medicine -
-
Conflictology -
Ecology -
Economy -
Finance -
History -
Law -
Medicine -
Philosophy -
Religious studies -
|
 P.9
P.9