2 Breast Diseases
Abigail D. Winder
Jill Edwardson
Breast cancer is a common and devastating health issue for many women. One in eight women will develop breast cancer in her lifetime. Benign breast disease can be difficult to differentiate from malignant breast disease, and it is crucial that the gynecologist be able to evaluate and treat breast disease (Fig.
2-1).ANATOMY
• The borders of the adult breast are the second and sixth ribs in the vertical axis and the sternal edge and midaxillary line in the horizontal axis. A small portion of breast tissue also projects into the axilla, forming the axillary tail of Spence.
• The breast is composed of three major tissues: skin, subcutaneous tissue, and breast tissue. The breast tissue, in turn, consists of parenchyma and stroma. The parenchyma is divided into 15 to 20 segments that converge at the nipple in a radial arrangement. There are between 5 and 10 collecting ducts that open into the nipple. Each duct gives rise to buds that form 15 to 20 lobules, and each lobule consists of 10 to 100 alveoli, which constitute the gland.
• The breast is enveloped by fascial tissue. The superficial pectoral fascia envelops the breast and is continuous with the superficial abdominal fascia of Camper. The undersurface of the breast lies on the deep pectoral fascia, covering the pectoralis major and serratus anterior muscles. Connecting the two fascial layers are fibrous bands (Cooper suspensory ligaments) that are the natural support of the breast.
• The principal blood supply to the breast is the internal mammary artery, constituting two thirds of the total blood supply. The additional third, which supplies primarily the upper outer quadrant, is provided by the lateral thoracic artery. Nearly all of the lymphatic drainage of the breast is to the axillary nodes. The internal mammary nodes also receive drainage from all quadrants of the breast and are an unusual, but potential, site of metastasis.
• The majority of abnormalities in the breast that result in biopsy are due to benign breast disease. Benign abnormalities can result in pain, a mass, calcifications, and nipple discharge. Similar findings can be present in malignant disease.
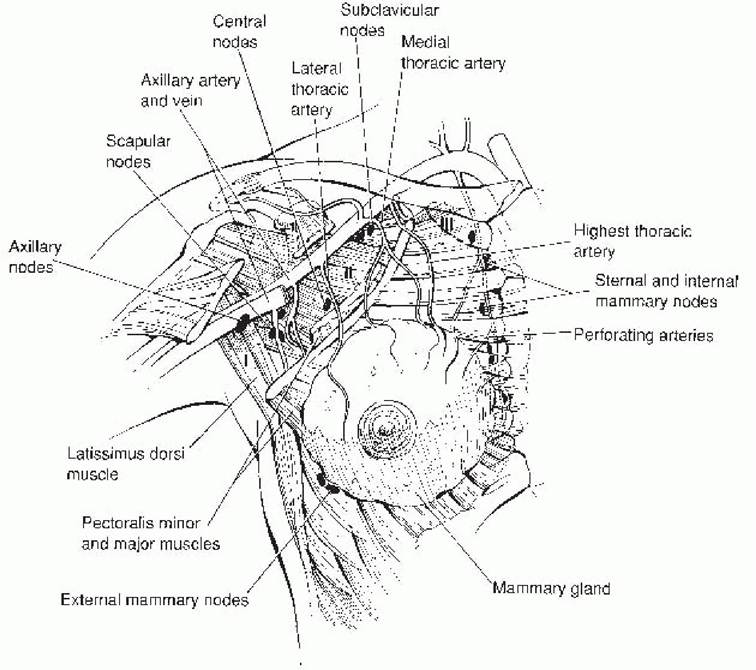
Figure 2-1. Anatomy of the breast. Roman numerals (I, II, III) indicate axillary lymph node levels. (From Green VL. Breast diseases: benign and malignant. In Rock JA, Jones HW, eds. TeLindeS Operative Gynecology, 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2008, with permission.)
• For the purposes of delineating metastatic progression, the axillary lymph nodes are categorized into levels. Level I lymph nodes lie lateral to the outer border of the pectoralis minor muscle, level II nodes lie behind the pectoralis minor muscle, and level III nodes are located medial to the medial border of the pectoralis minor muscle.
SCREENING AND DIAGNOSIS
The main screening modalities include clinical breast exam, breast self-exam, and screening mammography (Table 2-1). Diagnostic modalities include diagnostic mammography and breast biopsy (including fine needle, core, and excisional). Additional diagnostic modalities include ultrasound and magnetic resonance imaging (MRI).
Breast Exam
• The clinical breast examination (CBE) should be part of the gynecologic examination (Fig. 2-2) and is best for detecting tumors greater than 2 cm in size. The National Breast and Cervical Cancer Early Detection Program found that CBE detects approximately 5% of cancers that are not visible on mammography. Also, it offers an opportunity to demonstrate the technique of breast self-examination and to encourage women to perform this examination on a regular basis. The examination consists of:
P.18
TABLE 2-1 Breast Cancer Screening Techniques and Guidelines
Screening recommendations differ for patients with a family or personal history of breast cancer.
aA summary of guidelines can be found at the National Guideline Clearinghouse. Available at: http://www.guideline.gov.USPSTF, U.S. Preventive Services Task Force; ACOG, American College of Obstetricians and Gynecologists; ACS, American Cancer Society; NCI, National Cancer Institute.
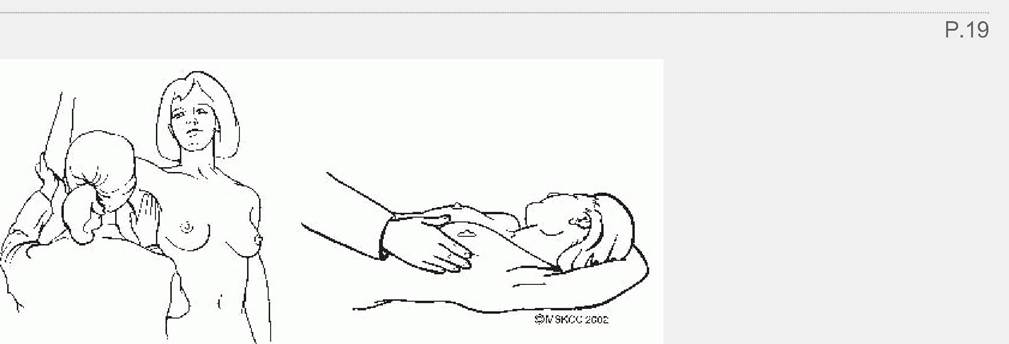
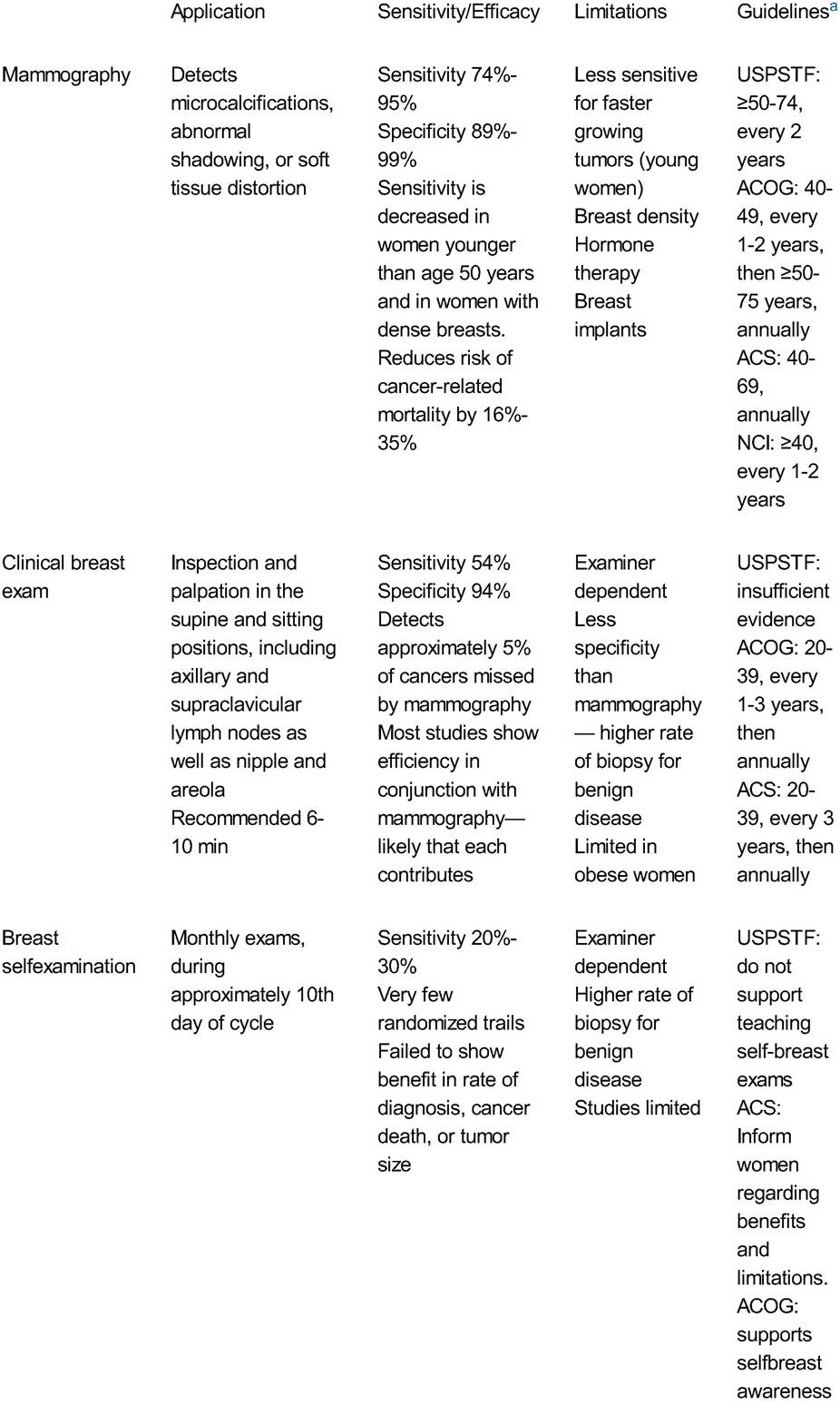
Figure 2-2. Breast examination. (From Scott JR, Gibbs RS, Karlan BY, et al. Danforth’s Obstetrics and Gynecology, 9th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2003:892-893, with permission.)
• Inspection and palpation of the breasts in the supine and sitting positions, with hands above the head and then on the hips. The supine position flattens the breast tissue against the chest, allowing for a more thorough exam.
• Observation of the contour, symmetry, and vascular pattern of the breasts for signs of skin retraction, edema, or erythema in each of the previously mentioned positions
• Systematic palpation of each breast, the axilla, and supraclavicular areas in a circular motion using light, medium, and deep pressures. Use the pads of the three middle fingers to palpate for masses. A vertical strip pattern appears more thorough than concentric circles. To ensure that all breast tissue is examined, cover a rectangular area bordered superiorly by the clavicle, laterally by the midaxillary line, and inferiorly by the bra line.
• Evaluation for nipple discharge, crusting, or ulceration
• For the anatomic location and description of tumors or disease, the surface of the breast is divided into four quadrants and the numbers of the face of a clock are used as reference points (Fig. 2-3). A finding may be described as “a hard mass palpated in the upper inner quadrant of the right breast at the 2 o'clock position, approximately 2 cm from the nipple.”
• The clinical use of breast self-examination is controversial (see Table 2-1). Breast self-awareness is a woman's awareness of the normal appearance and feel of her breasts and may or may not include breast self-examination.
She is encouraged to discuss any changes in her breasts with her health care provider.Mammography
• Although mammography remains the primary screening modality for breast cancer, as well as mammography for women older than age 35 years. The primary value of mammography is to provide reassurance. Patients with no dominant mass can be reassured.
• In most cases, mastalgia resolves spontaneously, although sometimes only after months or years. Restriction of methylxanthine-containing substances (e.g., coffee, tea) has not been shown to be superior to placebo, but some patients may note relief.
P.23 Pain from a macrocyst may be relieved with aspiration. Symptomatic relief may be achieved with a supportive brassiere, acetaminophen, or a nonsteroidal antiinflammatory drug (NSAID). Finally, cyclic pain may be partially relieved with oral contraceptives, thiazide diuretic, danazol, or tamoxifen.
Breast Mass
• Evaluation of a palpable breast mass requires a careful personal history, family history, physical examination, and radiographic examination. A breast mass reported by the patient should undergo the same evaluation, even if it fails to be appreciated on physical exam.
• In general, breast tissue can be lumpy and irregular. The following are characteristics concerning for cancerous lesions: single, hard, immobile, irregular margins, and >2 cm. In the majority of cases, cancerous masses are painless, but 10% of patients with cancer present with some symptoms of breast discomfort. Symptoms that may be associated with breast cancer include nipple discharge, nipple rash or ulceration, diffuse erythema of the breast, adenopathy, or symptoms associated with metastatic disease.
• Diagnostic mammography is recommended in the evaluation of any woman older than age 35 years with a palpable breast mass. Findings suspicious for cancer on mammography include increased density, irregular margins, spiculation, or an accompanying cluster of microcalcifications (Fig.
2-4).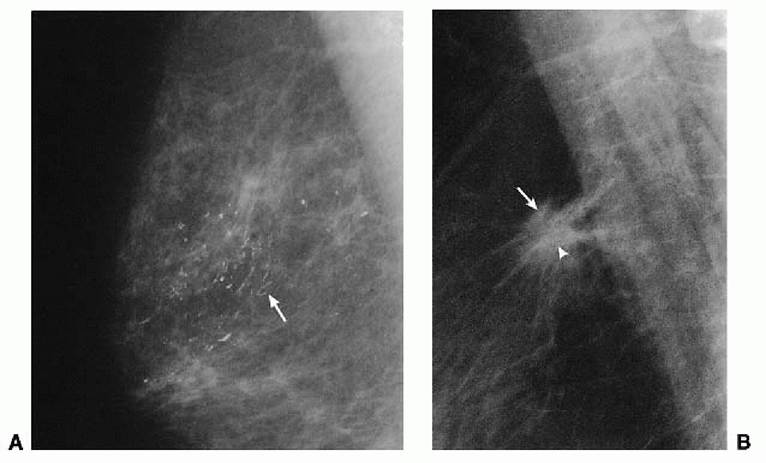
Figure 2-4. (A) A 53-year-old woman with bloody discharge from the nipple. Mediolateral view of the right breast demonstrates casting calcifications involving a large part of the breast extending to the nipple. The calcifications are nonuniform, irregular, and branched (arrow), and they form a dot-dash linear pattern. They are aligned with the ductal system. (B) A 60-yearold woman with a palpable mass and no other pertinent history. Mediolateral view of the right breast reveals a spiculated mass (arrow) with architectural distortion. Within the center of the mass, irregular (pleomorphic) microcalcifications are present (arrowhead). The diagnosis is carcinoma, largely DCIS, of comedo type (A) and invasive ductal carcinoma, not otherwise specified (B). (From Pope TL Jr. Aunt Minnie’s Atlas and Imaging Specific Diagnosis, 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2003:329, with permission.)
P.24
• In women younger than age 35 years, ultrasonography may be used to distinguish a simple cyst from a more worrisome complex cyst, solid mass, or tumor.
• Fine-needle aspiration, core needle biopsy, or excisional biopsy can be used for ultimate tissue diagnosis of the palpable mass. Bloody fluid yielded on aspiration or persistence of a mass after aspiration should prompt excisional biopsy or surgical consultation.
• The combination of physical examination, mammography, and fine-needle aspiration biopsy is referred to as
triple diagnosis. Fewer than 1% of breast cancers are missed using this diagnostic approach.
• Benign breast masses include fibroadenomas, breast cysts, or fat necrosis.
• Fibroadenoma is the most common mass lesion found in women younger than 25 years of age. Growth is gradual, and occasional cystic tenderness may be present. If the lesion is palpable, increasing in size, or psychologically disturbing, core or excisional biopsy should be considered.
Conservative treatment may be appropriate for small lesions that are not palpable and have been identified as fibroadenomas. Carcinoma within a fibroadenoma is a rare occurrence. A rare malignant tumor that can be confused with fibroadenoma is cystosarcoma phyllodes, which is treated by wide resection with negative margins. Local recurrence is uncommon, and distant metastasis is very rare.• Breast cysts can be found in premenopausal or postmenopausal women. Physical examination cannot distinguish cysts from solid masses. Ultrasonography and cyst aspiration are diagnostic. Simple cysts have a thin wall with no internal echoes and are benign. In these cases, no further therapy is required. Complex cysts have a thickened wall or internal septation and are considered suspicious. Complex cysts generally undergo some form of biopsy. If a cyst does not resolve with aspiration, yields a bloody aspirate, recurs within 6 weeks, or is complex on ultrasound evaluation, surgical consultation should be obtained.
• Fat necrosis is frequently associated with breast trauma resulting in a breast mass. It can occur after breast biopsy, infection, duct ectasia, reduction mammoplasty, lumpectomy, and radiotherapy for breast carcinoma. Fat necrosis is most common in the subareolar region. This process can be difficult to distinguish from breast cancer on both physical examination and mammography. The lesion needs to be evaluated like any other palpable breast lesion. Only a benign histologic appearance affords reassurance.
Breast Infections
• Puerperal mastitis is an acute cellulitis of the breast in a lactating woman. Mastitis usually occurs in the early weeks of breast-feeding. On inspection, cellulitis is often present in a wedge-shaped pattern over a portion of the breast skin, and tissue is warm, red, and tender. The infection is around rather than within the duct system, leading to the absence of purulent discharge from the nipple. Patients may present with high fevers, chills, flu-like malaise, and body aches. The most common causal organism is Staphylococcus aureus. Prompt initiation of antibiotic therapy, usually with dicloxacillin (500 mg by mouth four times a day for 10 days), reduces the risk of abscess formation. Aggressive emptying of the affected breast is an important treatment. The patient should be encouraged to continue breast-feeding or pumping to promote drainage. Warm compresses and manual pressure are also beneficial. Microbiologic culture is indicated if the mastitis does not resolve or if an abscess develops. The latter case also warrants incision and drainage.
P.25
• Nonpuerperal mastitis is an uncommon, subareolar infection. In contrast to puerperal mastitis, nonpuerperal mastitis is usually a polymicrobial infection and the woman is generally not systemically ill. Antibiotic coverage typically includes clindamycin or metronidazole, in addition to a beta-lactam antibiotic. All breast inflammation must raise concern for inflammatory breast cancer, and the threshold for performing a skin biopsy should be low, particularly in the elderly population. Failure to respond to antibiotic treatment should prompt biopsy in any patient. Finally, the patient should be up-to-date with mammography screening.
NIPPLE DISCHARGE
• Nipple discharge is a common complaint and finding on examination of the breast. Nipple discharge is usually benign (95% of cases). The causes of discharge range from physiologic to endocrine-related to pathologic. See Figure 2-5 for an algorithm for evaluation of nipple discharge.
• Physiologic secretion from the nipple during examination or nipple stimulation is a common occurrence. As many as 50% to 80% of women in their reproductive years can express one or more drops of fluid. This benign discharge is usually nonspontaneous, bilateral, and serous in character. If the remainder of the breast exam is normal, reassurance is sufficient, and no further workup is necessary.
• Galactorrhea is milk production unrelated to nursing or pregnancy and is typically a bilateral, multiductal discharge. Several endocrine abnormalities give rise to galactorrhea, such as dopamine inhibitors, hypothalamic/pituitary disease, hypothyroidism, postthoracotomy syndrome, and chronic renal failure. Chronic breast stimulation or exogenous estrogen via oral contraceptive pills may cause galactorrhea. One third of cases are idiopathic. Evaluation includes a careful history reviewing medications and recent trauma/stimulation of the breast and physical exam. Questioning includes symptoms of amenorrhea, hypothyroid disease, visual field changes, or new-onset headaches which may suggest the underlying cause of the galactorrhea. Further evaluation includes a prolactin level, thyroid function tests, and brain MRI if the prolactin level is elevated. Prolactin levels may be falsely elevated after meals, after breast examination, or based on diurnal variation.
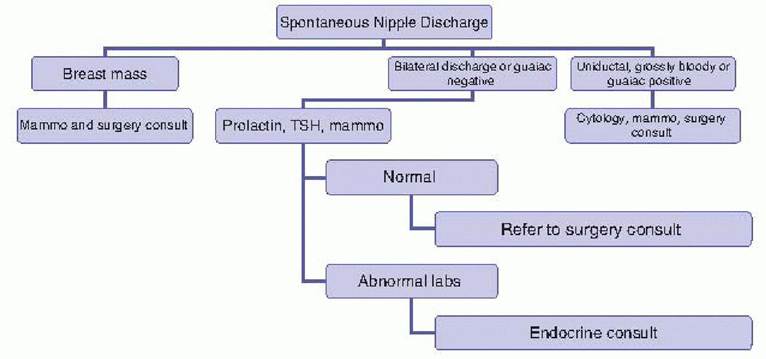
Figure 2-5. Algorithm for evaluation of nipple discharge. Mammo, mammogram; TSH, thyroid-stimulating hormone.
P.26
• Pathologic discharge is typically unilateral and spontaneous. It may be greenish gray, serous, or bloody.
Causes of pathologic discharge are carcinoma, intraductal papilloma (straw-colored), duct ectasia, and fibrocystic changes. Only 5% of pathologic discharge is caused by carcinoma. A physical exam should attempt to identify the area of the breast and the specific duct from which the discharge is expressed. Skin lesions or an associated mass may be identified. If the fluid is not grossly bloody, guaiac testing may be performed to identify subtle bloody fluid. If grossly bloody or guaiac positive, cytology is performed; otherwise, the sensitivity of cytology is very low for malignancy. In addition, imaging with bilateral mammography is required. If the patient is younger than 35 years, ultrasound may also be used.
BREAST CANCER
Breast cancer is the most common cancer affecting women in the United States and second only to lung cancer in cancer mortality for women. Median ages of diagnosis and of death are 61 and 69 years, respectively. Primarily due to improved screening, the prevalence of breast cancer has doubled in the past 50 years. The lifetime risk of breast cancer for a woman is 12.7% (about one in eight).
Risk Factors
• The most commonly used model to determine breast cancer risk is the Gail model. The number of first- degree relatives with breast cancer, age at menarche, age at first live birth, number of breast biopsies, and presence of atypical hyperplasia on a breast biopsy are its components. Its accuracy is limited as it omits a detailed family history of breast and ovarian cancers and underestimates the risk in African American women and overestimates the risk in Asian American women. This model should not be used in women who have a personal history of breast cancer or women who are known gene mutation carriers.
• Age is the primary risk factor for breast cancer (Table 2-3). Approximately 95% of breast cancers occur in women older than 40 years of age.
| TABLE 2-3 Age-Specific Probabilities of Developing Invasive Breast Cancer | |
| Age | Probability of Developing Breast Cancer in the Next 10 Years |
| 20 | 1:1,681 |
| 30 | 1:232 |
| 40 | 1:69 |
| 50 | 1:42 |
| 60 | 1:29 |
| 70 | 1:27 |
| Lifetime 1:8 | |
| From American Cancer Society. Breast Cancer Facts and Figures 2011-2012. Atlanta, GA American Cancer Society, 2012. | |
P.27
• Family history and genetic predisposition: Family history confers an increased risk for breast cancer, specifically with a history of premenopausal breast cancer in a first-degree relative, male breast cancer, bilateral breast cancer, or a combination of breast and ovarian cancers within a family.
• BRCA1 and BRCA2 are tumor suppressor genes with autosomal dominant inheritance. Inheriting BRCA1 or BRCA2 confers a 40% to 85% lifetime risk of breast cancer, yet these cases account for micropapillary, cribriform, and comedo. DCIS can also be graded as low, intermediate, or high. DCIS is an early, noninfiltrating form of breast cancer with minimal risk of metastasis and an excellent prognosis with surgical therapy with or without radiation therapy. The goal of treatment of DCIS is to prevent the development of invasive breast cancer. With the increased use of mammography, DCIS is being diagnosed more often.
• Invasive cancer: The two most common types of invasive cancers are lobular and ductal. Infiltrating lobular carcinoma is a variant associated with microscopic lobular architecture. These carcinomas account for 10% to 15% of invasive breast cancers, are often multifocal, have a higher incidence of bilaterality, and are less evident on mammography. Infiltrating ductal carcinoma accounts for 60% to 75% of all tumors. These cancers account for a group of tumors classified by cell type, architecture, and pattern of spread. These
include mucinous, tubular, and medullary carcinomas.
Staging and Prognostic Factors
• The tumor-node-metastasis (TNM) staging system for breast cancer from the American Joint Committee on Cancer uses tumor size, axillary node status (incorporating sentinel nodes), and metastasis status (Tables 2-4 and 2-5). Prognosis is strongly correlated with tumor size and node status. Expression of estrogen and progesterone receptors in tumor tissue is associated with a better prognosis and can assist in systemic treatment. Other prognostic factors include tumor grade, tumor size, and expression of the human epidermal growth factor receptor 2 (HER2∕neu) oncogene.
• HER2∕neu is a gene encoding transmembrane receptors for growth factors, thus regulating cellular growth and differentiation. Overexpression of this oncogene leads to a more aggressive subtype of breast cancer, which tends to be poorly differentiated and high grade. They have high rates of lymph node involvement and are more resistant to conventional chemotherapy. All newly diagnosed invasive breast cancer patients should have HER2 status checked.
Treatment
Early detection is the key to improved survival (Table 2-6). In general, clinical stage I, IIA, or IIB, and certain patients with clinical stage IIIA disease (T3N0) are considered early stages of breast cancer. These patients are generally treated with surgery to the breast and regional lymph nodes with or without radiation therapy. Systemic therapy may be offered based on primary tumor characteristics, such as hormone and HER2 receptor status, lymph node involvement, and tumor size and grade. Treatment for locally advanced breast cancers (clinical stage IIIA with T0 to T3, N2 disease, or T4 disease) includes multimodal therapy.
P.29
TABLE 2-4 TNM Classification of Breast Cancer
Notation Description
Tumor size
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
Tis Carcinoma in situ: intraductal carcinoma, LCIS, or Paget disease of the nipple with no tumor
T1 Tumor 2 cm in greatest dimension
T1a T umor 0.5 cm in greatest dimension
T1b T umor >0.5 cm but 1 cm in greatest dimension
T1c Tumor >1 cm but 2 cm in greatest dimension
T2 T umor >2 cm but 5 cm in greatest dimension
T3 T umor >5 cm in greatest dimension
T4 T umor of any size with direct extension to the chest wall or skin
T 4a Extension to the chest wall
T4b Edema (including peau d’orange) or ulceration of the skin of the breast or satellite skin
T 4c Both T 4a and T 4b
T4d Inflammatory carcinoma
Lymph node metastases
NX Regional lymph nodes cannot be assessed (e.g., previously removed)
N0 No regional lymph node metastasis
N1 Metastasis to movable ipsilateral axillary lymph node(s)
N2 Metastasis to ipsilateral axillary lymph node(s), fixed to one another or other structures
N3 Metastasis to ipsilateral internal mammary lymph node(s)
Distant metastases
M Presence of distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis (including metastasis to ipsilateral supraclavicular lymph node[s])
TNM, tumor-node-metastasis.
From American Cancer Society. How is cancer staged?
http://www.cancer.org/Cancer/BreastCancer/DetailedGuide/breast-cancer-staging. Accessed May 13, 2013.
Surgical or Local Treatment
• Mastectomy involves the complete surgical removal of breast tissue. Mastectomy is recommended if the disease is multicentric, invades skin and chest wall, or has inflammatory features or if negative margins cannot be achieved with breast preservation. Radical mastectomy includes removal of the breast, overlying skin, pectoralis major and minor, and the entire axillary contents. The modified radical
mastectomy includes removal of the entire breast and underlying fascia of the pectoralis major muscle and levels I and II of the axillary lymph nodes. A total or simple mastectomy removes the breast with the nipple areolar complex but without lymph nodes. “Skin-sparing” mastectomy provides superior cosmetic results and may be appropriate for patients with DCIS; stage I, II, or III breast cancer; or for prophylactic mastectomy. Nipple-sparing mastectomy is controversial in the treatment of breast cancer. Any type of mastectomy can be performed with or without immediate reconstruction.
TABLE 2-5 TNM Staging System for Breast Cancer
| Stage | T umor Size | Lymph Node Metastases | Distant Metastases |
| 0 | Tis | N0 | M0 |
| I | T1 | N0 | M0 |
| IIa | T0 | N1 | M0 |
| T1 | N1 | M0 | |
| T2 | N0 | M0 | |
| IIb | T2 | N1 | M0 |
| T3 | N0 | M0 | |
| IIIa | T0 | N2 | M0 |
| T1 | N2 | M0 | |
| T2 | N2 | M0 | |
| T3 | N1, N2 | M0 | |
| IIIb | T4 | Any N | M0 |
| Any T | N3 | M0 | |
| IV | Any T | Any N | M1 |
TNM, tumor-node-metastasis. From American Cancer Society. How is cancer staged? http://www.cancer.org/Cancer/BreastCancer/DetailedGuide/breast-cancer-staging. Accessed May 13, 2013.
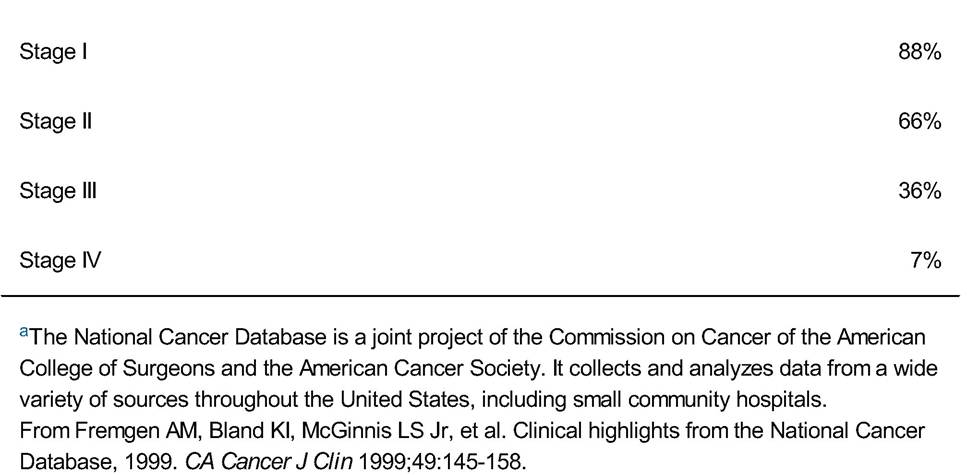
TABLE 2-6 Prognosis by Stage: 10-Year Breast Cancer Survival Based on the National Cancer Databasea

P.31
• In breast-conserving therapy (BCT), a wide local excision or lumpectomy is performed to achieve a 1- to 2-mm negative histologic margin. Adjuvant radiation therapy (RT) is required. Radiation is delivered to the entire breast with a possible boost dose to the lumpectomy bed. Trials comparing BCT + RT and mastectomy show comparable survival rates.
• Assessing axillary lymph node status is important in prognosis, staging, and treatment planning. However, potential complications of axillary dissection include lymphedema (10% to 15%), pain, numbness, or weakness of the affected arm.
• Evaluation of the clinically suspicious axillary node can be accomplished with ultrasound plus fine-needle aspiration or core biopsy.
• Sentinel lymph node biopsy has evolved into the method of choice for axillary node staging in the clinically negative axilla. The sentinel lymph node is identified using radioactive tracer or dye injected into the periareolar region of the breast. When the isotope and dye are used in combination, the positive predictive value of sentinel node biopsy approaches 100%.
• RT, although most often administered as part of BCT, can also be used for other indications.
Systemic Therapy
• Systemic therapy given before surgery is termed neoadjuvant therapy and is often recommended for patients with locally advanced disease. Adjuvant therapy, which is given after surgery, is typically recommended to patients with hormone receptor-positive breast cancer, positive lymph node findings, or other high-risk characteristics.
• Hormonal therapy is the most frequently recommended adjuvant systemic therapy and is aimed at targeting estrogen receptor- and/or progesterone receptor-positive breast cancer. Tamoxifen, a selective estrogen receptor modulator, has been used most commonly. Hormone therapy results in a 26% annual reduction in the risk of recurrence and a 14% annual reduction in the risk of death from breast cancer. Tamoxifen is administered at 20 mg/day for at least 5 years. It is associated with a twofold increased risk of endometrial cancer. Therefore, abnormal uterine bleeding in a premenopausal woman or any postmenopausal bleeding in a woman taking tamoxifen should be assessed with endometrial sampling. However, routine imaging or endometrial sampling is not recommended for tamoxifen users.
• Aromatase inhibitors (e.g., letrozole, anastrozole, and exemestane) are potent inhibitors of estrogen synthesis and are therefore only used in postmenopausal women. They have been shown to be more effective than tamoxifen in treating breast cancer, with virtually no risk of endometrial hyperplasia and a reduced risk of thromboembolic events when compared to tamoxifen. Side effects include osteoporosis, myalgias, elevated cholesterol, and joint pain. These agents are effective as first-line agents or as second-line agents in patients whose cancer has progressed during or after tamoxifen therapy.
• Biologic therapy: Trastuzumab (Herceptin) is a genetically engineered monoclonal antibody to the HER2 protein. Its use concurrently with chemotherapy in HER2-positive breast cancers results in significant improvement in disease-free and overall survival. There is, however, an increased risk of congestive heart failure and decreased left ventricular ejection fraction in patients receiving trastuzumab, so routine cardiac monitoring is recommended.
P.32
• Chemotherapy has been shown to improve overall survival and reduce the odds of death by 25% in selected patients. The decision to use cytotoxic chemotherapy depends on tumor histology, tumor size, nodal status, genomic profiling, and benefit-risk calculators.
Metastatic or Advanced Disease
• Although breast cancer is uncommonly found to be metastatic at the time of presentation, approximately one third of patients subsequently develop distant metastatic disease. Median survival for patients with metastatic disease is 18 to 24 months, but fewer than 5% live beyond 5 years. Breast cancer metastasizes to the bone, liver, and brain. The goal of therapy in metastatic disease is prolongation of survival and palliation of symptoms. Treatments typically include endocrine therapy, chemotherapy, or biologic therapy. Surgery or radiation could be considered for recurrence limited to one organ.
Prevention
• Chemoprevention includes treatment with tamoxifen and raloxifene. Appropriate candidates for prophylactic endocrine therapy include women older than age 35 years with a history of LCIS, DCIS, or atypical ductal or lobular hyperplasia; women older than age 60 years; women between ages 35 and 59 years with Gail model risk of breast cancer ≥1.66% over 5 years; or women with known BRCA1 or BRCA2 mutations who do not undergo prophylactic mastectomy. Prophylactic tamoxifen reduces the risk for estrogen receptor-positive breast cancer in women without previous breast cancer but does not impact overall survival.
• Raloxifene is a selective estrogen receptor modulator that reduces the incidence of hormone-positive breast cancer in postmenopausal women but like tamoxifen has no effect on survival. It is slightly less effective than tamoxifen in preventing breast cancer but has lower risks of uterine cancer/hyperplasia and thromboembolic disease. Its use has not been studied in premenopausal women.
• Aromatase inhibitors are currently being evaluated in clinical trials for the primary prevention of breast cancer.
• Surgical prevention can be considered in two groups of women: (a) patients positive for BRCA1 or BRCA2 and (b) patients with a strong family history suggestive of hereditary breast cancer but negative for BRCA1 or BRCA2. Surgical prevention includes contralateral mastectomy, prophylactic bilateral mastectomy, and bilateral salpingo-oophorectomy. Prophylactic bilateral mastectomies have been shown to reduce the risk of breast cancer by 90%. This is increased to 95% if combined with a bilateral salpingo-oophorectomy.
Pregnancy and Breast Cancer
• Pregnancy-associated breast cancer is diagnosed during pregnancy, in the first postpartum year, or any time during lactation. Breast cancer is the most common cancer in pregnancy, with an incidence of 1 in 3,000 gestations. The average patient age is 32 to 38 years. Breast cancer can be especially difficult to diagnose during pregnancy and lactation (secondary to increased glandular breast tissue), which may lead to a delay in diagnosis. Thus, cancers are often found at a later stage in pregnant women or immediately postpartum. Mammograms may be performed safely during pregnancy. Pregnant patients do as well as their nonpregnant counterparts at a similar disease stage.
P.33
• T reatment during pregnancy is generally the same as that for nonpregnant patients. The tumor can usually be fully excised or mastectomy performed during pregnancy. The agents used to identify the sentinel lymph node are not approved in pregnancy and therefore, axillary dissection is commonly performed. Initiation of chemotherapy is generally considered safe after the first trimester. Radiotherapy should be avoided until after delivery. No evidence has been reported that aborting the fetus or interrupting the pregnancy leads to improved outcome.
SUGGESTED READINGS
American College of Obstetricians and Gynecologists. Practice bulletin no. 122: breast cancer screening. Obstet Gynecol 2011;118:372-382.
American College of Obstetricians and Gynecologists. Practice bulletin no. 103: hereditary breast and ovarian cancer syndrome. Obstet Gynecol 2009;113:957-966.
Leach MO. Breast cancer screening in women at high risk using MRI. NMR Biomed 2009;22:17-27.
Speroff L, Fritz MA, eds. The breast. In Clinical Gynecologic Endocrinology and Infertility. Philadelphia, PA: Lippincott Williams & Wilkins, 2005:573-620.
More on the topic 2 Breast Diseases:
- 2 Breast Diseases
- Chapter 33 Disorders of the Breast
- EVALUATING CREDENTIALS and GRANTING PRIVILEGES ^57 ^95 ^186