Contraception
Contraception is most commonly used to space pregnancies, rather than to avoid them permanently. Because of this, many methods of contraception are used which have a significant failure rate (50).
For example, one of the most popular forms of contraception is the male condom, and even with ‘perfect use' this is associated with 2 unintended pregnancies for every 100 women-years of use. A more typical failure rate is 15%. For more effective contraception, women most commonly use the combined oral contraceptive pill, which has a ‘perfect use' failure rate of 0.3 per 100 women-years, and a typical failure rate of 8%. However, even this high efficacy may not be adequate in women for whom an unintended pregnancy could be fatal (those in the high-risk groups). Moreover, both the oestrogen and progestogen component of the combined oral contraceptive confer a 3.5 times increased relative risk of thrombosis in users compared with non-users (51). The ‘low-dose progestogen-only pills' such as Micronor are considered medically safe in all forms of heart disease, but their failure rate is similar to that of the combined pill and they should not therefore be recommended for high-risk women when avoidance of pregnancy is a high priority. They also suffer from the disadvantage that the pregnancy rate after a single missed pill is substantially higher than with the combined oral contraceptive.As a result of these considerations, the three most widely used reversible forms of contraception in women with heart disease are the oral contraceptive progestogen-only pill Cerazette/Cerelle, containing desogestrel (75 mg), the progestogen implant (Nexplanon), and the progestogen intrauterine contraceptive device (LNG-IUS (Mirena)). Cerazette/Cerelle has a failure rate similar to that of the combined oral contraceptive pill, its major disadvantage being an increased incidence of progestogenic side effects such as irregular bleeding when compared with the low-dose progestogen-only pills.
The progestogen implant has the lowest failure rate of any form of contraception, 1 in 2000 women-years, and once inserted remains effective for at least 3 years. The major reason for discontinuation is irregular bleeding, which occurs in about 20%. The progestogen intrauterine contraceptive device has a failure rate of 1 in 500 women-years but has the advantage of commonly producing amen- orrhoea (useful in women prone to anaemia) and being effective for at least 5 years. The major disadvantage is a small (0.1%) risk of syncope during insertion, and therefore in women with cardiac disease it should only be inserted in an environment fully equipped for resuscitation, and preferably with an anaesthetist in attendance. The copper T intrauterine device is not recommended for routine use because of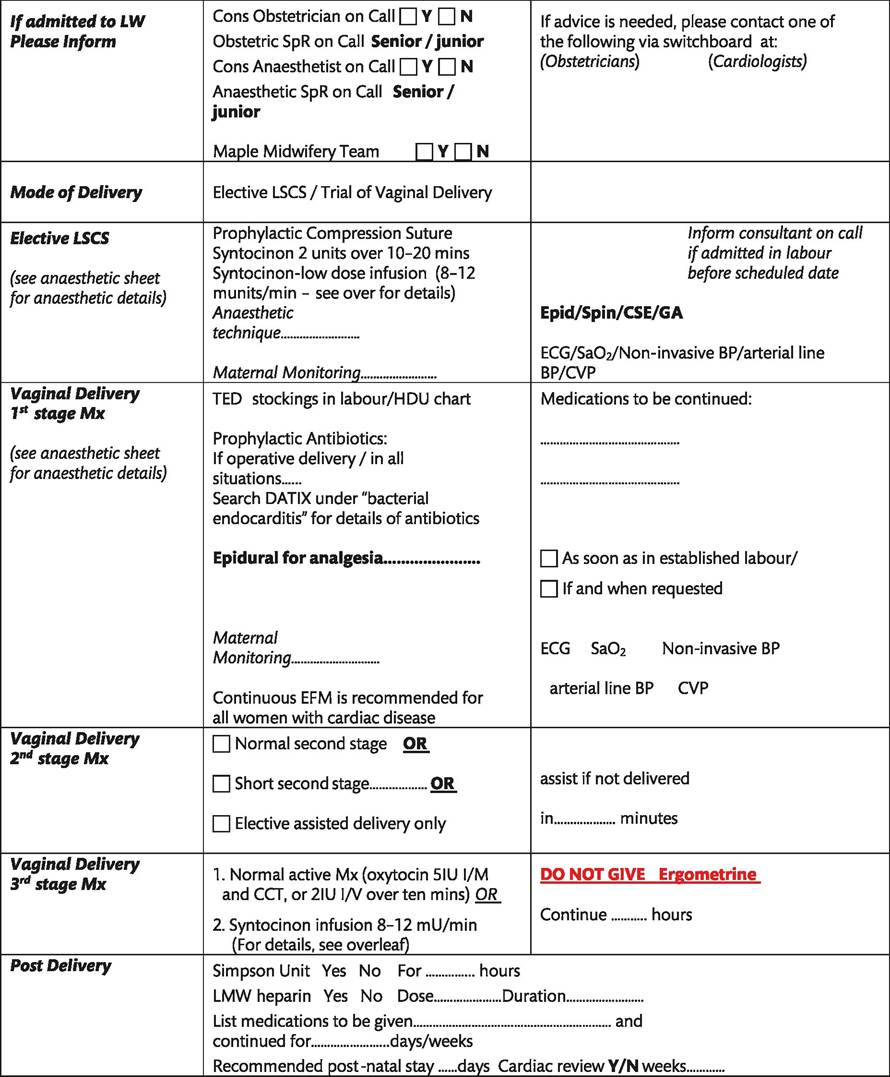
Figure 12.5 Example of a clinical management plan for delivery.
its failure rate of 1 in 120 women-years, but it can be useful for post- coital contraception because inserting it within 7 days of unprotected intercourse prevents implantation in the great majority of cases.
Sterilization can also be considered if the woman is sure she does not want children, or if she considers her family is complete. Male sterilization can be inappropriate if the woman's life expectancy is substantially reduced because he may wish to have a pregnancy with a future partner. The commonest form of female sterilization, clipping the fallopian tubes at laparoscopy, is contraindicated because the generation of a carbon dioxide pneumoperitoneum can compromise cardiac function in susceptible women. However, there is a more recent form of sterilization in which coils are inserted into the base of the fallopian tubes via a hysteroscope (Essure). This can be performed under sedation as an outpatient provided resuscitation facilities are immediately available in case of syncope. Occasionally, salpingectomy at caesarean section is appropriate. Clearly, all forms of reversible contraception require detailed counselling before they are undertaken.
Please inform the Consultant Obstetrician on call if there is departure from planned management or if unexpected clinical situations develop in women with cardiac disease
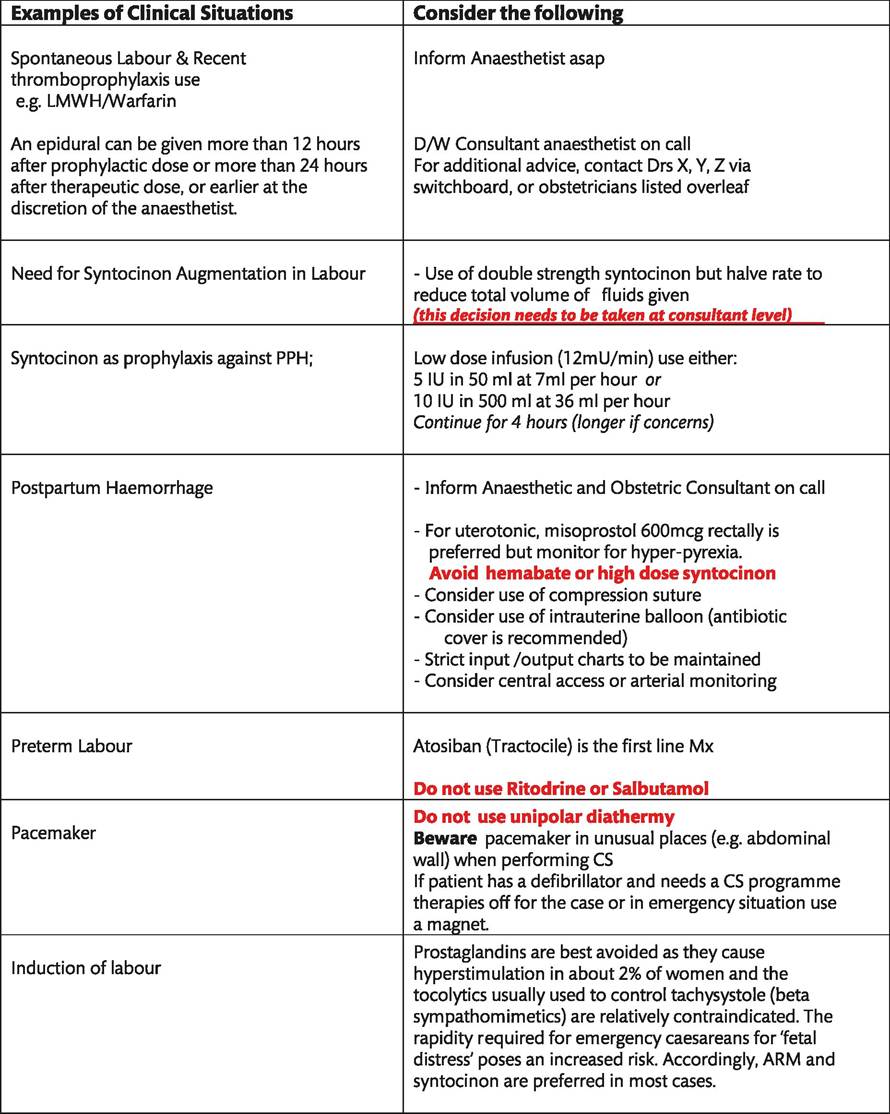
Figure 12.5 Continued