Cardiopulmonary Resuscitation
During Pregnancy
David Caro and Stephen Topp
The incidence of maternal cardiopulmonary arrest during pregnancy is estimated to occur once in every 30,000 deliveries. Events leading to cardiopulmonary arrest in the pregnant patient (Table 5.1) include those found in the general population and those related specifically to pregnancy (1-6).
Maternal arrest is a dramatic and difficult situation that requires the practitioner to make rapid decisions and take defined actions in order to maximize survivability. The approach to any cardiopulmonary arrest victim, including those who are pregnant, follows a set of defined algorithms designed to maximize the likelihood of recovery in the event of a cardiopulmonary arrest (7,8).Cardiopulmonary resuscitation (CPR) refers to the application of both basic (BLS) and advanced (ALS) life support algorithms. Both BLS and ALS follow a streamlined format designed to intervene on life-threatening disorders that could potentially be reversed. A simple and easy-to-recall starting point is to approach each unstable or cardiopulmonary arrest victim in an “ABCDE” method, which is supported by multiple life support training courses (7,8). This ABCDE method becomes the basis for resuscitative evaluation, critical decision making, and intervention.
This chapter is designed to arm the practitioner with the tools necessary to manage the critically unstable patient or cardiopulmonary arrest victim. Cardiopulmonary physiology deserves special attention, especially in light of the dramatic alterations in cardiopulmonary physiology that accompany pregnancy and the unique fetal effects associated with maternal cardiac arrest and resuscitation. Discussion will then turn to BLS and ALS techniques, including critical equipment and medications. Finally, new resuscitation modalities will be reviewed to give a glimpse into recent advances in resuscitative technology.
UNIQUE ANATOMIC AND PHYSIOLOGIC CONSIDERATIONS
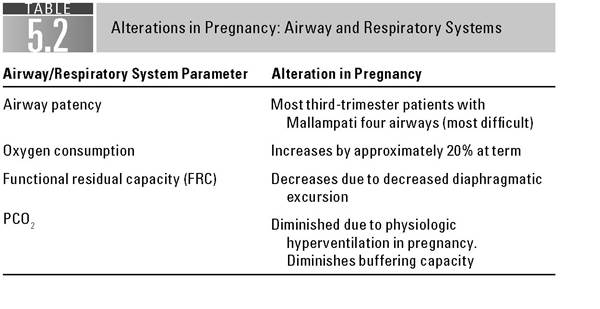
(SEE TABLES 5.2 AND 5.3)
Critical airway changes occur as the gravid patient approaches term. The most important is edema of the upper airway, causing a number of patients to go from a simple, straightforward laryngoscopic approach to a much more difficult one (9). The anesthesia method of analyzing airway difficulty includes the Mallampati assessment, which is a grading scale for a rapid assessment of the ease of laryngoscopy. Most women go from class 1 or 2 airways (easy intubations) to class 4 airways (most difficult intubations) by term (9). The practitioner must anticipate this during intubation attempts and have an alternative airway plan when attempting to control the airway.
The most critical respiratory concern is the contraction of maternal functional residual capacity when she nears term (9-11). The gravid uterus displaces abdominal contents superiorly and will encroach on the reserve of air in the lung bases. The result is lower vital capacity and lower physiologic oxygen reserve, even when fully pre-oxygenated with a nonrebreather mask for 5 to 8 minutes (9). This results in hypoxia developing more rapidly than expected and difficulty reoxygenating a pregnant patient, especially when lying flat (9).
Common Etiologies of Cardiac Arrest During Pregnancy
Specifically associated with pregnancy
Pregnancy-induced cardiomyopathy
Pregnancy-induced hypertension (preeclampsia and eclampsia)
Obstetric hemorrhage
Amniotic fluid embolism
Iatrogenic
Hypermagnesemia
Anesthesia during delivery
Not specific to pregnancy
Preexisting cardiovascular disease
Myocardial infarction
Congenital heart disease
Acquired valvular disease
Arrhythmia
Pulmonary disease
Pulmonary embolism
Asthma
Aspiration pneumonia
Anaphylaxis and angioedema
Intracranial hemorrhage
Sepsis
Trauma
Electrical injury
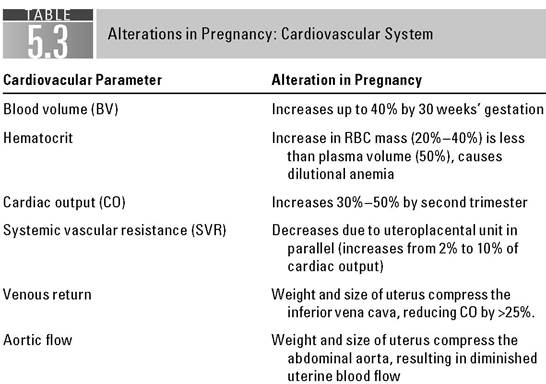
Maternal blood volume increases during pregnancy and serves to protect maternal cardiovascular physiology in the face of hypovolemia (11).
However, the uterine circulation is passive and dependent on normal maternal blood volume and flow, as it is in a parallel circuit with the maternal circulation (10). The gravid uterus also impacts maternal circulation by its size and weight. The uterus can compress the inferior vena cava and the distal aorta during later pregnancy. A critical maneuver to recall in the face of maternal shock or cardiac arrest is to either manually displace the uterus to the patient’s left or to roll the patient into the left lateral decubitus position. These maneuvers will serve to decompress the great vessels and augment cardiac return (1-3,6,10-14). Poor venous return from infradiaphragmatic vessels makes the femoral and saphenous sites poor choices for administering drugs and fluids during CPR (6,15), and furthermore, therapeutic resuscitation doses of vasopressors, especially a -adrenergic or combined a- and ^-adrenergic agents, may produce uteroplacental vasoconstriction, thereby further compromising already diminished uteroplacental blood flow (10).Some fetal physiologic changes are protected during maternal arrest. The oxyhemoglobin dissociation curve of fetal hemoglobin is shifted to the left when compared to maternal hemoglobin, yielding a greater oxygen saturation of fetal hemoglobin at any given partial pressure of oxygen (10,16). This enables the fetus to extract and carry a larger amount of oxygen at lower oxygen tension than the mother. The integrity of vital organs can be preserved for a limited period of time with this central redistribution of blood flow, but if asphyxia persists, such physiologic adjustments become inadequate, and neurologic damage or death of the fetus will occur (16,17).
It is also critical to remember that the best chance for fetal survival is with a resuscitated mother; however, experience with perimortem cesarean section indicates that fetal survival and neurologic outcome are best if delivery is performed within 5 minutes of maternal arrest (6,11,12,18,19).
If CPR is unsuccessful, then rapid cesarean section is the only hope for fetal viability above 24 weeks’ gestation (see Chapter 6).RESUSCITATION OVERVIEW
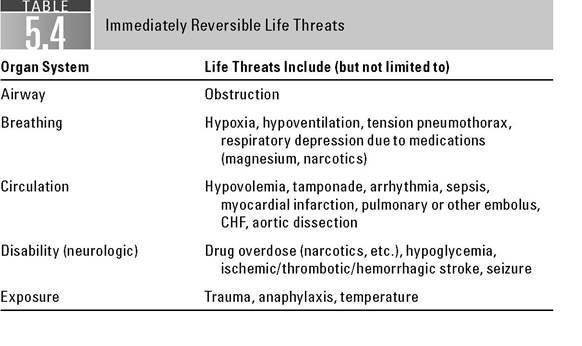
The approach to any unstable or unresponsive patient follows the ABCDE paradigm. Each letter in the mnemonic stands for a vital system that must be evaluated in the order that is designated. Any abnormality demands immediate intervention. The ABCDEs of resuscitation help identify reversible life threats that must be dealt with before moving on to the next system or a complete history and physical examination (Table 5.4).
BASIC LIFE SUPPORT
Airway assessment in a crisis includes a quick check to hear if the patient can phonate. A phonating patient has a patent airway. Stridor, snoring, and/or gurgling respiratory sounds should raise concern that the airway is compromised. A cardiac arrest victim may have no spontaneous respirations and will then need BLS maneuvers and bag-mask ventilation to ensure airway patency. BLS airway maneuvers include the chin-lift and jaw-thrust techniques as well as the Heimlich maneuver in out-of-hospital arrest (8,20-22).
The chin lift consists of the use of index and long fingers to pull a supine patient’s chin toward the ceiling, thereby pulling the base of the tongue off of the hypopharynx. The jaw thrust consists of using the index and long fingers of both hands to apply anterior pressure behind both angles of the mandible to cause the same effect (9,12). Use the jaw-thrust technique if there is a concern for cervical spine trauma. Either of these maneuvers helps to alleviate airway obstruction caused by loose pharyngeal musculature. The practitioner or an assistant then applies a bag-mask device attached to a high-flow oxygen source to the patient’s face and delivers two breaths to determine if the patient has chest rise. Chest rise reassures that the airway is patent. No chest rise means that an airway obstruction is present and must be relieved; the initial maneuver would then be repositioning the airway, along with better bag-mask seal.
If this is unsuccessful, then another airway-clearing maneuver should be considered.The Heimlich maneuver consists of quick, forceful thrusts to the upper abdomen directed in a posterior/superior vector in an attempt to force air in the
lungs upward through the trachea to dislodge a foreign body. This maneuver is carried out with the rescuer standing behind a standing victim, with arms wrapped around the victim’s abdomen and hands grasped in an overlapping fist. The fists are traditionally placed at a level superior to the umbilicus but below the xiphoid process. Quick, posterior/superior pulls then are applied in an attempt to clear the airway. Alternatively, a supine patient can be straddled, hands can be clasped with fingers interlocked, and the palm heels used to create quick pushes along the same vector. A practitioner with advanced airway equipment can also perform laryngoscopy accompanied by MaGill forceps when faced with an airway obstruction, with the MaGill used to extract any foreign body encountered (9,12,22,23).
Breathing assessment includes the observation of presence, speed, and depth of spontaneous respiration. Regular respiratory rates for the nonpregnant patient are from 12 to 16; in the gravid patient, the base respiratory rate increases above 20 (11). Patients without spontaneous respiration require oxygenation and ventilator support with bag-mask ventilation. Basic breathing support for spontaneously breathing patients might include oxygen by nonrebreather mask or bag-mask ventilation timed with ventilatory effort. Listen to both lung fields to determine that they are equal. Unequal breath sounds could identify a tension or spontaneous pneumothorax that would require needle decompression with a large-bore angio- cath (12 or 14 gauge in the second intercostal space in the midclavicular line of the affected side) for relief (12).
Circulation assessment includes determination of pulse rate and rhythm along with blood pressure estimation.
Patients will tend to lose peripheral pulses before femoral or carotid; if radial pulses are present, the patient has a minimum blood pressure of at least 70 mm Hg (24). An absence of pulses mandates the start of chest compressions.Chest compressions should occur with the patient supine on a flat surface, with the uterus displaced to the right by an assistant (1,6,12). Alternatively, the patient can be placed in a 15- to 30-degree left lateral decubitus position. Although placing the patient in the true left lateral decubitus position will make manual chest compressions clumsy and ineffective, placing the patient in a 15-degree left lateral tilt position through the use of either a backboard or a tilt table may provide an acceptable alternative to manual uterine displacement without significantly compromising chest compressions (1,2,4,12). Compressions should be 1.5 to 2in. deep and should be at a rate of approximately 100 bpm (8,25). Once started, compressions should continue with minimal interruption while ALS maneuvers occur (see below) (8,15,22).
Other BLS circulatory support activities include the establishment of large bore (18 gauge or higher) peripheral intravenous access sites, usually in the ante- cubital fossae. The patient should be attached to an automated external defibrillator (AED) if the practitioner is unfamiliar with defibrillation (21,26,27). TheAED should be turned on and then compressions should stop temporarily, allowing the machine to analyze the patient’s cardiac rhythm and deliver counter shock if required. A patient who has suffered cardiac arrest from ventricular fibrillation requires prompt electric countershock using current Basic (BCLS) and Advanced (ACLS) Cardiac Life Support guidelines (26,27). Current guidelines recommend either monophasic defibrillation at 200, 300, and then 360J for the initial three shocks, with all subsequent shocks at 360J or biphasic defibrillation at 100, 200, and 200J for the first shocks, with all subsequent shocks at 200J (26). Newer defibrillators (e.g., the LifePack 12®) are biphasic. There is no contraindication to external defibrillation during pregnancy, and direct current (DC) countershocks of up to 400J have been used in pregnant patients without adverse fetal effects (6,28,29).
Neurologic assessment typically includes determination of unresponsiveness or level of alertness. If the patient is conscious, a quick determination of motor, verbal, and eye-opening responses to verbal and/or painful stimuli gives the team a baseline neurologic status to follow throughout the resuscitation (12,30,31). Reversible causes of neurologic depression can mimic cardiac arrest and should be investigated. Common reversible causes include hypoglycemia and drug overdoses (especially narcotics) (31).
Finally, as the resuscitation proceeds, a full examination of the patient is completed to ensure that obvious life-threatening hemorrhage, trauma, or other injuries do not exist.
ADVANCED LIFE SUPPORT
A complete description of advanced airway techniques is beyond the scope of this chapter. The reader is referred to an alternative text for a full discussion of emergency airway management (9). Some specific tools and strategies bear mentioning, as full term patients are by definition difficult airways.
Emergent laryngoscopy and intubation are daunting tasks. Familiarity with intubation equipment is a necessity. A standard intubation in a pregnant patient must take into account the various physiologic changes that make laryngoscopy difficult. Paralytics can be used for intubation in the pregnant patient, but assessment of airway difficulty is important, as rapid decline in oxygenation can occur and intubation attempts might fail, necessitating a surgical airway (9).
A wide variety of alternative airway equipment exists, in addition to standard bag-mask devices and laryngoscopes. The most important for this discussion include the supraglottic airway devices and the bougie. Supraglottic devices are attractive alternative airways, as they require minimal training, can be inserted blindly, and provide a means for rapid oxygenation and ventilation (9,23). These devices include the laryngeal mask airway (LMA)®, the intubating LMA®, and the King LT airway®, among others. Each has an inflatable cuff at the end of the device designed to be seated over the glottis, which allows for ventilation when attached to a bag device. These devices have been included in the American Heart Association ACLS algorithm due to their ease of use and high success rates in establishing a means of oxygenation and ventilation (9,23).
The bougie is an aid to standard laryngoscopy and endotracheal intubation. Various forms of bougies exist. The two most common are made of solid plastic or of gum elastic. The bougie functions as an intubation guide to be used in difficult airways when the vocal cords are unable to be seen while performing direct laryngoscopy but some other glottis structure or the epiglottis is visualized. It has an angled tip that allows the practitioner to “hook” under the epiglottis and advance forward into the trachea. The practitioner then uses tactile sensation to feel the bougie gently bounce along the tracheal cartilage rings to confirm that it is in the airway, or alternatively, one can feed the bougie until it stops in a bronchus (and therefore confirms it is in the airway). Lack of tracheal ring “bumping” felt through the bougie as it advances or lack of defined endpoint as the bougie is inserted means that the device is not in the airway (9). An endotracheal tube can then be advanced over the bougie into the airway.
Advanced ventilatory support includes the use of medications, noninvasive positive pressure devices, and mechanical ventilation. Various combinations of advanced medications are employed for respiratory distress depending on the underlying cause of the problem. ^2-Agonists, anticholinergic agents, and steroids are employed in asthmatics. Nitroglycerin is employed in congestive heart failure patients. In severe respiratory difficulty, the use of noninvasive positive pressure devices for those requiring ventilatory support can at times avert intubation (9,12). Depending on the cause of respiratory distress, various medications can be employed in an attempt to help improve physiologic parameters. Once the decision to intubate has been made, mechanical ventilation becomes the mainstay of therapy. Various modes of ventilation exist. A frequently used mode immediately following intubation is synchronized intermittent mandatory ventilation (SIMV). The practitioner sets the rate of breaths to be given, the tidal volume to be given (5 to 7 mL/kg), the FiO2 (usually started at 100%), and any pressure support (usually started at 10 cm H2O) and positive end expiratory pressure (usually started at 5 cm H2O) needed to maintain oxygenation (10,12). A full discussion of ventilator devices and parameters is beyond the scope of this chapter, and the reader is encouraged to further investigate a critical care textbook for a more in-depth discussion.
CARDIAC RHYTHM ANALYSIS
Advanced cardiac life support measures require familiarity with cardiac rhythm analysis and the treatment of underlying rhythm abnormalities. Tachyarrhythmias, bradyarrhythmias, and cardiac arrest may occur during pregnancy and each has the abilit y to pose a substantial risk to the mother and the fetus. Although clinically significant or lethal arrhythmias are uncommon in the premenopausal female (32), when compared to their nongravid cohorts, pregnant females are more vulnerable to cardiac arrhythmias (33). Prompt identification and treatment of these rhythm disturbances are of utmost importance to both the mother and the fetus.
Basic Rhythm Analysis
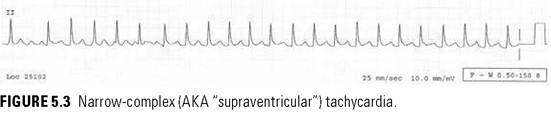
When attempting to analyze an EKG or rhythm on a bedside monitor, it is important to recognize a few key points about the rhythm’s appearance. It is helpful to determine the rate of the rhythm (fast versus slow) and if it is regular or irregular. A slow rate is 100 bpm, but this will vary according to the stage of pregnancy. A rate >150 is definitely abnormal. The timing or intervals between the beats determine whether the rhythm is regular or irregular. Next, determine if the QRS complex is wide or narrow. The normal appearance of the QRS complex on an EKG or bedside monitor will be “narrow,” meaning between 0.06 and 0.11 seconds, or three small boxes on the EKG paper. Any QRS greater than three small boxes is termed “wide complex” and is abnormal. Finally, the origin of the rhythm should be sought. A “sinus” rhythm originates in the SA node and correctly travels down the conduction system to the ventricles. This is denoted on the EKG by the P wave, normally a single, upward deflection just preceding the QRS complex. If no P wave is present, the rhythm has origin outside of the normal conducting system (i.e., foci within the atria or ventricles).
Bradyarrhythmias
Symptomatic bradycardia is a rare occurrence during pregnancy (33). Sinus bradycardia is a slow (usually hearts, metabolic derangements such as thyroid disease or alcohol intoxication should be sought. Additionally, other acute cardiac conditions such as pericarditis, mitral stenosis, or pulmonary embolus should be considered. In general, AFib is a narrow-complex, irregularly irregular rhythm with a rate that can vary from normal to tachycardic. In contrast, atrial flutter is usually a narrow-complex, regular rhythm with a varying rate. As with SVT, unstable AFib and atrial flutter are safely treated with synchronized DC cardioversion. For stable patients, rate control is usually achieved with β-blockers, calcium channel blockers, or digoxin.
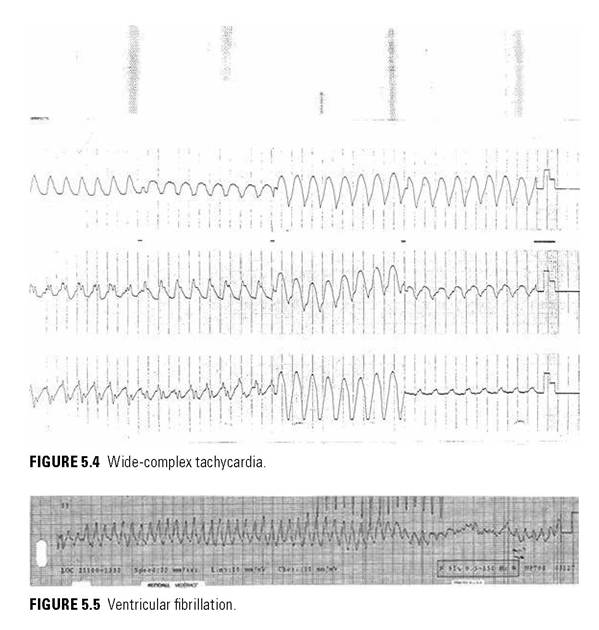
Ventricular Tachycardia
Ventricular tachycardia (VT) is a very fast, wide-complex ventricular rhythm (usually >150 bpm) and is usually dissociated from any underlying atrial rate (Fig. 5.4). In pregnant and nonpregnant patients with structurally normal hearts, VT is rare. During pregnancy, the occurrence of VT is often due to severe electrolyte or acid-base disorders or by maternal abuse of stimulant drugs. As with other arrhythmias, once VT is identified, the patient must be assessed for hemodynamic instability. For the unstable patient with a palpable pulse, VT is treated emergently with synchronized cardioversion at 100 J. If no pulse is palpable, treat like ventricular fibrillation (see next section) and defibrillate with 200J. For hemodynamically stable VT, conservative management is indicated. Procainamide (class C) and Lidocaine (class B) appear safe during pregnancy and should be used in sustained, stable VT (36). The role of Amiodarone during pregnancy is limited by its teratogenic profile (class D), and its use should be limited to pharmacologic and shock resistant VT (32).
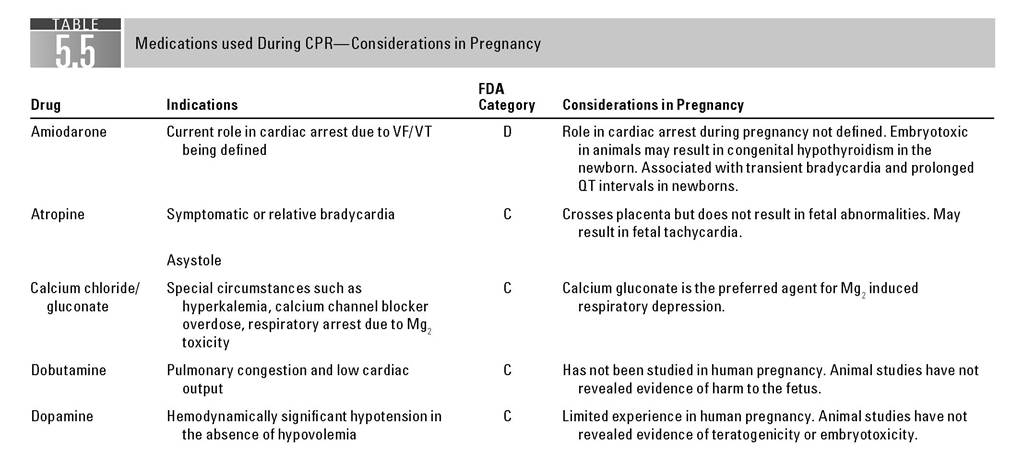
Cardiac Arrest: Ventricular Fibrillation, Pulseless Electrical Activity, and Asystole
Ventricular fibrillation (VF) is caused by disorganized electrical activity originating in the ventricles. Because organized electrical activity is absent, the ventricles are not contracting effectively and the patient is without perfusion. This rhythm will appear as a fast, sinusoidal wave pattern with no normal, discernable QRS complex (Fig. 5.5). When this rhythm is encountered, the patient is by default unstable and chest compressions must be started immediately until defibrillation is available. Defibrillate at 200J followed by chest compressions for at least 2 more minutes regardless of return of spontaneous circulation (ROSC). The 2005 American Heart Association ACLS guidelines stress the importance of minimal interruptions in chest compressions as each pause drastically reduces the coronary perfusion pressures (9). Early administration of vasopressors, either epinephrine or vasopressin, is standard but should not interfere with CPR and shocks. Little information exists about ACLS pharmacologic therapy in pregnancy. In theory, these adrenergic agents may reduce the uteroplacental blood supply. However, standard ACLS doses and protocols should be used in all pregnant resuscitations (1,15,37).
Pulseless electrical activity (PEA) is a rhythm defined by the presence of organized electrical activity (not VT or VF) as displayed on a cardiac monitor in the absence of a pulse. In contrast to unstable VT and VF, a PEA rhythm will not benefit from cardioversion or defibrillation. Minimally-interrupted chest compressions and pharmacologic therapy with vasopressors (epinephrine or vasopressin) and atropine are the foundation of PEA ACLS care. PEA is frequently caused by reversible etiologies and correction of these is the best chance for a successful resuscitation. It is helpful to remember the “Five H’s and T’s” when PEA is encountered: hypovolemia, hypoxemia, hydrogen ion (acidosis), hyper/hypokalemia, hypothermia and thrombosis (coronary and pulmonary embolus), tension pneumothorax, tamponade (cardiac), tablets (drug OD) (15). Pregnant patients are particularly vulnerable to pulmonary embolus and hypovolemia secondary to hemorrhage; however, consideration of all causes is prudent.
Asystole is the cardiac arrest rhythm with the most dismal prognosis. It is characterized by little to no cardiac electrical activity (usually a “flat line” on the monitor) and no pulse. As with PEA, asystole does not benefit from cardioversion or defibrillation. The best chance for successful resuscitation is to identify and treat the reversible cause. The treatment algorithm for asystole mirrors that of PEA, with quality, minimally interrupted chest compressions and pharmacologic therapy with vasopressors and atropine (15).
Clinical experience with the pharmacologic agents used in ACLS is limited in pregnancy. The general recommendation is that standard pharmacologic therapy be used without modification (6). Vasopressors such as epinephrine and dopamine generally are avoided during pregnancy because of their adverse effects on uteroplacental blood flow but should not be withheld during arrest when clinically indicated (6,38). Similarly, despite theoretical concerns about some drugs such as lidocaine inducing fetal acidosis and ^-blocking agents inducing fetal bradycardia, no adverse fetal effects have been shown when these agents are used in maternal cardiac arrest (6,29,38,39). Table 5.5 lists the drugs commonly used during CPR and their application during pregnancy.
The initial minutes of a maternal resuscitation should focus on restoration of the maternal cardiorespiratory function. Optimum fetal care occurs in the setting of a resuscitated mother. However, if immediate resuscitative efforts do not restore spontaneous circulation, consideration should be given to the performance of a crash cesarean section. Most texts give a guideline of 3 to 5 minutes of maternal resuscitation before crash c-section is initiated (1,6,38,40). The reader is referred to the chapter in this text describing this technique. It is important to note that once the fetus is delivered, a resuscitative team should redirect attention to the mother, as case reports of ROSC have occurred following fetal delivery by crash c-section (6,41).
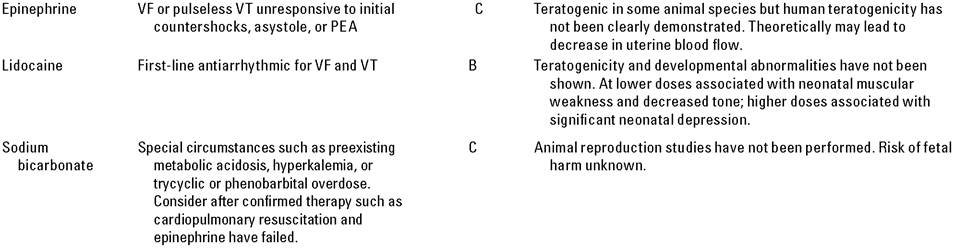
FDA, Food and Drug Administration; VF1 ventricular fibrillation; VT1 Ventriculartachycardia; PEA, pulseless electrical activity.
Sources: Clinical Pharmacology [database online], Tampa, FL: Gold Standard, lnc.; 2009. URL: http://cp.gsm.com.lp.hscl.ufl.edu Updated February 2009. MICR0MEDEX® Healthcare Series, Copyright© 1974-2009. Thomson Reuters. All rights reserved.
EMERGING TECHNOLOGIES
Resuscitative technologies continue to creatively explore methods of resuscitation that are just now being studied in human populations, including maternal cardiac arrests. Therapeutic hypothermia has been demonstrated to improve neurologic outcomes in cardiac arrest survivors (38,42). This technique has also been employed successfully in case reports of maternal arrest (43). Similarly, fibrinolytic therapy has been considered for use in cardiac arrest for patients with pulmonary embolism (38), but the use of this treatment would complicate emergent cesarean section.
COMPLICATIONS OF CPR
Maternal complications of CPR include fractures of ribs and sternum, hemothorax, hemopericardium, and laceration or rupture of internal organs, most notably the liver, spleen, and uterus (10,12). Damaging fetal effects include central nervous system toxicity from medications, transient dysrhythmias from DC countershock, altered uterine activity, and reduced uteroplacental perfusion with possible fetal hypoxemia and acidemia (44,45).
SUMMARY
Cardiopulmonary arrest during pregnancy occurs infrequently. Most resuscitative procedures require little alteration, with the exception of displacement of the gravid uterus during the latter part of pregnancy. Resuscitative attempts should be directed primarily toward the mother, with the best chance of fetal survival being maternal survival. Perimortem cesarean section should be considered after the age of fetal viability, in an attempt both to save the infant and to improve maternal hemodynamics.
References
1. Atta E, Gardner M. Cardiopulmonary resuscitation in pregnancy. Obstet Gynecol Clin North Am. 2007;34:585-597, xiii.
2. Peters CW, Layon AJ, Edwards RK. Cardiac arrest during pregnancy. J Clin Anesth. 2005;17:229-234.
3. Mallampalli A, Powner DJ, Gardner MO. Cardiopulmonary resuscitation and somatic support of the pregnant patient. Crit Care Clin. 2004;20:747-761, x.
4. Whitty JE. Maternal cardiac arrest in pregnancy. Clin Obstet Gynecol. 2002;45: 377-392.
5. Einav S, Matot I, Berkenstadt H, Bromiker R, Weiniger CF. A survey of labour ward clinicians' knowledge of maternal cardiac arrest and resuscitation. Int J Obstet Anesth. 2008;17:238-242.
6. Part 10.8: Cardiac arrest associated with pregnancy. Circulation. 2005;112:IV- 150-153.
7. Part 1: Introduction. Circulation. 2005;112:IV-1-5.
8. Part 3: Overview of CPR. Circulation. 2005;112:IV-12-18.
9. Walls RM, Murphy MF. Manual of Emergency Airway Management. Philadelphia, PA: Lippincott Williams & Wilkins; 2008.
10. Dildy GA. Critical Care Obstetrics. Malden, MA: Blackwell; 2004.
11. Cunningham FG, Williams JW. Williams Obstetrics. New York, NY: McGraw-Hill Professional; 2005.
12. Roberts JR, Hedges JR, Chanmugam AS. Clinical Procedures in Emergency Medicine. Philadelphia, PA: W.B. Saunders; 2004.
13. Kiefer RT, Ploppa A, Dieterich HJ. Aortocaval compression syndrome. Der Anaesthe- sist. 2003;52:1073-1083, quiz 1084.
14. Bamber JH, Dresner M. Aortocaval compression in pregnancy: the effect of changing the degree and direction of lateral tilt on maternal cardiac output. Anesth Anal. 2003;97:256-258, table of contents.
15. Part 7.2: Management of cardiac arrest. Circulation. 2005;112:IV-58-66.
16. Reece EA, Hobbins JC. Clinical Obstetrics: The Fetus & Mother. Malden, MA: Blackwell; 2007.
17. Jensen A, Garnier Y, Berger R. Dynamics of fetal circulatory responses to hypoxia and asphyxia. Eur J Obstet Gynecol Reprod Biol. 1999;84:155-172.
18. Stallard TC, Burns B. Emergency delivery and perimortem C-section. Emerg Med Clin North Am. 2003;21:679-693.
19. Yildirim C, Goksu S, Kocoglu H, Gocmen A, Akdogan M, Gunay N. Perimortem cesarean delivery following severe maternal penetrating injury. Yonsei Med J. 2004;45: 561-563.
20. Part 1: Introduction. Circulation. 2005;112:1-4.
21. Part 2: Adult basic life support. Circulation. 2005;112:5-16.
22. Part 4: Adult basic life support. Circulation. 2005;112:IV-19-34.
23. Part 7.1: Adjuncts for airway control and ventilation. Circulation. 2005;112: IV-51-57.
24. Deakin CD, Low JL. Accuracy of the advanced trauma life support guidelines for predicting systolic blood pressure using carotid, femoral, and radial pulses: observational study. Br MedJ (Clinical Research Ed.). 2000;321:673-674.
25. Part 6: CPR techniques and devices. Circulation. 2005;112:IV-47-50.
26. Part 3: Defibrillation. Circulation. 2005;112:17-24.
27. Part 5: Electrical therapies: automated external defibrillators, defibrillation, cardioversion, and pacing. Circulation. 2005;112:IV-35-46.
28. Nanson J, Elcock D, Williams M, Deakin CD. Do physiological changes in pregnancy change defibrillation energy requirements? Br JAnaesth. 2001;87:237-239.
29. Page RL. Treatment of arrhythmias during pregnancy. Am Heart J. 1995;130: 871-876.
30. Anonymous. Advanced trauma life support for doctors ATLS: manuals for coordinators and faculty. Chicago, IL: American College of Surgeons; 2008.
31. Marx JA, Hockberger RS, Walls RM, Adams J, Rosen P. Rosens Emergency Medicine: Concepts and Clinical Practice. Philadelphia, PA: Mosby/Elsevier; 2006.
32. Kron J, Conti JB. Arrhythmias in the pregnant patient: current concepts in evaluation and management. JIntervent Card Electrophysiol IntJArrhythmias Pacing. 2007;19:95-107.
33. Li JM, Nguyen C, Joglar JA, Hamdan MH, Page RL. Frequency and outcome of arrhythmias complicating admission during pregnancy: experience from a high- volume and ethnically-diverse obstetric service. Clin Cardiol. 2008;31:538-541.
34. Trappe HJ. Acute therapy of maternal and fetal arrhythmias during pregnancy. J Intensive Care Med. 2006;21:305-315.
35. Elkayam U, Goodwin TM. Adenosine therapy for supraventricular tachycardia during pregnancy. Am J Cardiol. 1995;75:521-523.
36. Chow T, Galvin J, McGovern B. Antiarrhythmic drug therapy in pregnancy and lactation. Am J Cardiol. 1998;82:58I-62I.
37. Shapiro JM. Critical care of the obstetric patient. J Intensive Care Med. 2006;21: 278-286.
38. Part 4: Advanced life support. Circulation. 2005;112:25-54.
39. Part 7.3: Management of symptomatic bradycardia and tachycardia. Circulation. 2005;112:IV-67-77.
40. Bloom SL, Leveno KJ, Spong CY, et al. Decision-to-incision times and maternal and infant outcomes. Obstet Gynecol. 2006;108:6-11.
41. Finegold H, Darwich A, Romeo R, Vallejo M, Ramanathan S. Successful resuscitation after maternal cardiac arrest by immediate cesarean section in the labor room. Anesthesiology. 2002;96:1278.
42. Part 7.5: Postresuscitation support. Circulation. 2005;112:IV-84-88.
43. RittenbergerJC, Kelly E, Jang D, Greer K, Heffner A. Successful outcome utilizing hypothermia after cardiac arrest in pregnancy: a case report. Crit Care Med. 2008;36:1354-1356.
44. Littleford J. Effects on the fetus and newborn of maternal analgesia and anesthesia: a review. CanJAnaesth. 2004;51:586-609.
45. Dildy GA, Clark SL. Cardiac arrest during pregnancy. Obstet Gynecol Clin North Am. 1995;22:303-314.