Diabetic Ketoacidosis
GENERAL PRINCIPLES
Epidemiology
DKA, a potentially fatal complication of diabetes, occurs in up to 5% of patients with T1DM annually and can occur in insulin-deficient patients with T2DM.
It occurs less often in individuals with pancreatic diabetes due to deficient alpha and beta cell function.Pathophysiology
DKA is a catabolic condition that results from severe insulin deficiency, often in association with stress and activation of counterregulatory hormones (e.g., catecholamines, glucagon).
Risk Factors
Precipitating factors for DKA include inadvertent or deliberate interruption of insulin therapy, sepsis, trauma, myocardial infarction (MI), and pregnancy. DKA may be the first presentation of T1DM and, rarely, T2DM. DKA with euglycemia or lower-than-expected glucoses can occur with use of the sodiumglucose cotransporter-2 (SGLT2) inhibitor drugs, atypical antipsychotic agents, and some chemotherapy agents.
Prevention
DKA can be prevented in many cases, and its occurrence often suggests a breakdown in patient education and communication. Therefore, diabetes education should be reinforced at every opportunity, with special emphasis on (1) self-management skills during sick days; (2) the body's need for more, rather than less, insulin during illness; (3) testing of blood or urine for ketones; and (4) procedures for obtaining timely and preventive medical advice.
DIAGNOSIS
History
• Patients may describe a variety of symptoms including polyuria, polydipsia, weight loss, nausea, vomiting, and vaguely localized abdominal pain generally in the setting of persistent hyperglycemia. A
high index of suspicion is warranted because clinical presentation may be nonspecific.
• Tachycardia; prolonged capillary refill; rapid, deep, and labored breathing (Kussmaul respiration); and fruity breath odor are common physical findings.
• Prominent gastrointestinal (GI) symptoms and abdominal tenderness on examination should raise suspicion for intra-abdominal pathology.
• Dehydration is invariable and respiratory distress, shock, and coma can occur.
Diagnostic Testing
• Metabolic panel revealing anion gap metabolic acidosis.
• Positive serum #946;-hydroxybutyrate or ketones (a semiquantitative measurement of acetone, acetoacetate, and #946;-hydroxybutyrate) and positive urine ketones.
• Plasma glucose #8805;250 mg/dL (13.9 mmol/L). Euglycemic DKA (plasma glucose lt;200 mg/dL [11.1 mmol/L]) has been described in pregnancy, alcohol ingestion, fasting or starvation, during hospitalization, and in patients with both T1DM and T2DM treated with SGLT2 inhibitors.18
• Hyponatremia, hyperkalemia, azotemia, and hyperosmolality are other possible findings.
• A focused search for a precipitating infection is recommended if clinically indicated.
• An ECG should be obtained to evaluate electrolyte abnormalities and for unsuspected myocardial ischemia.
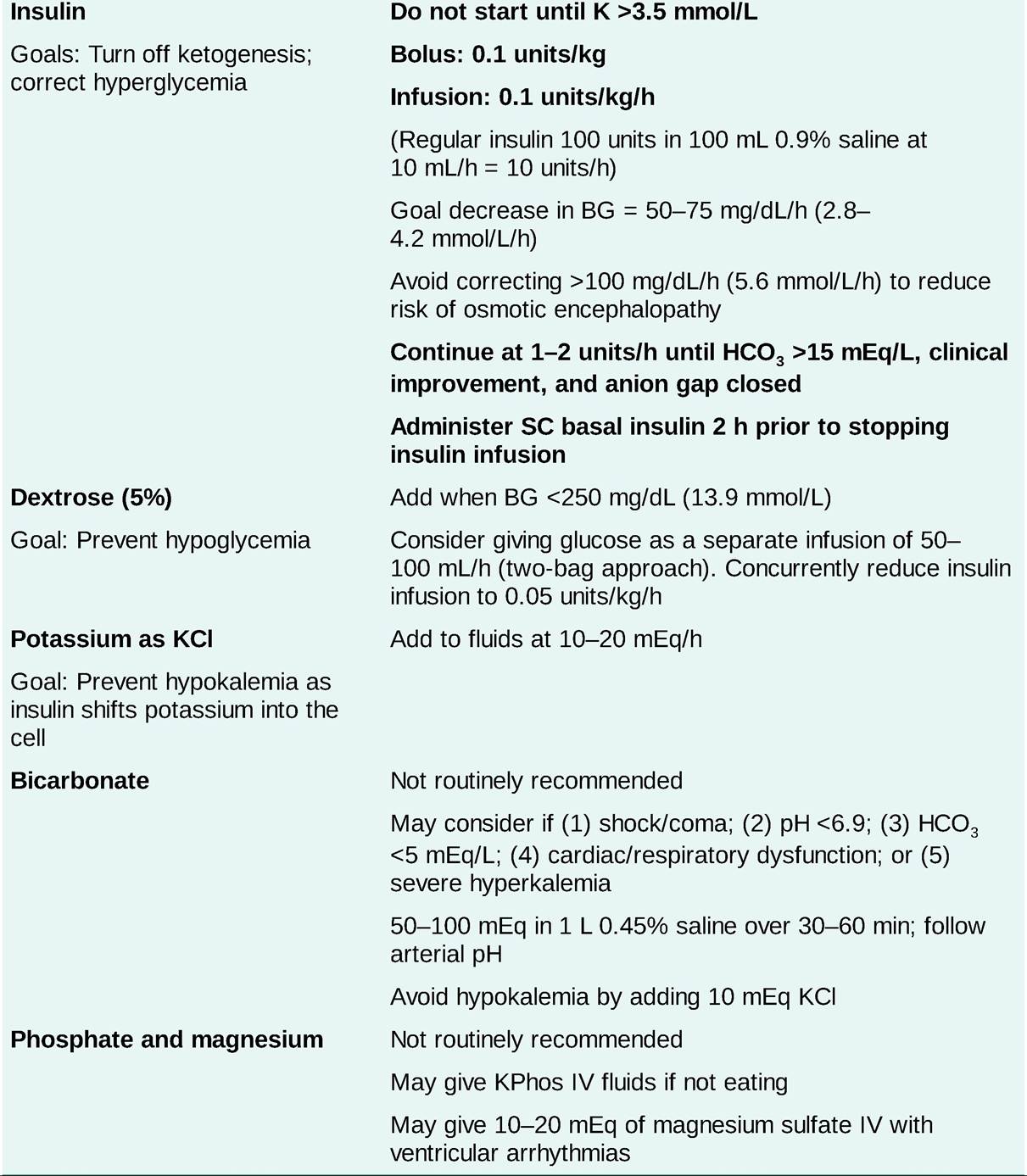
TREATMENT
Management of DKA should preferably be conducted in an ICU (Table 23-2). If treatment is conducted in a non-ICU setting, close monitoring is mandatory until ketoacidosis resolves and the patient's condition is stabilized. Mild to moderate DKA may be managed with subcutaneous insulin protocols in non-ICU settings.19 The therapeutic priorities are fluid replacement, adequate insulin administration, and potassium repletion. Administration of bicarbonate, phosphate, or magnesium, or other therapies are not routinely advised but may be appropriate in selected patients.
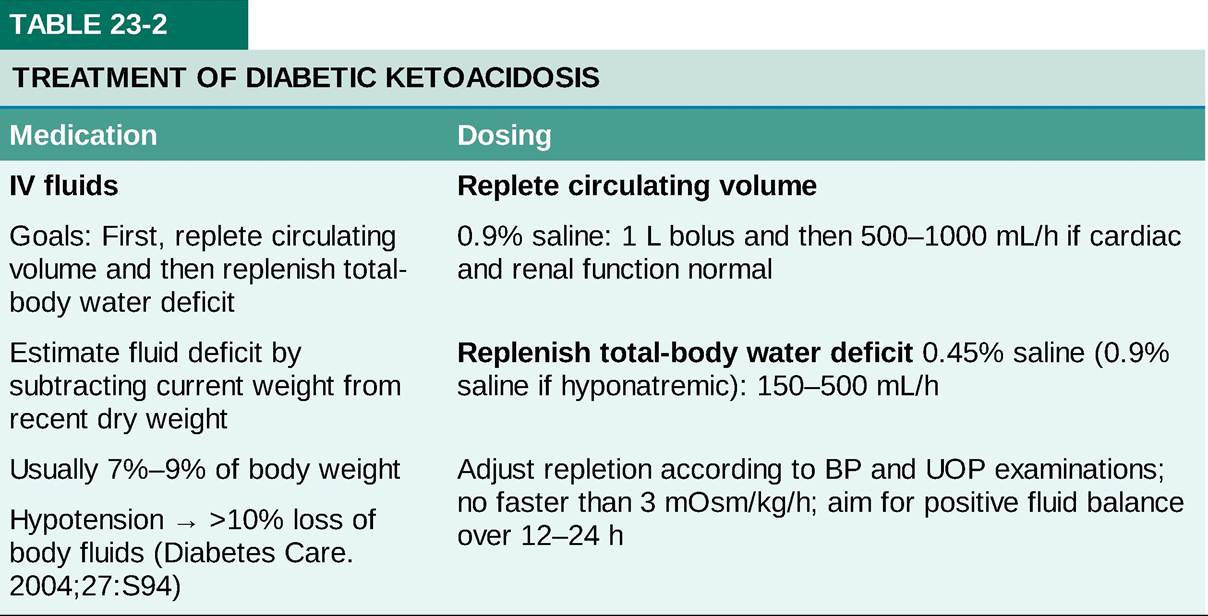
BG, blood glucose; BP, blood pressure; HCO3, bicarbonate; K, potassium; KCl, potassium chloride; KPhos, potassium phosphate; UOP, urine output.
• Monitoring of therapy
î BG levels should be monitored hourly, serum electrolyte levels every 2-4 hours, and arterial blood
gas values as often as necessary for a severely acidotic or hypoxic patient.
î Serum sodium tends to rise as hyperglycemia is corrected; failure to observe this trend suggests that the patient is being overhydrated with free water.
î Dextrose should be initiated when the blood glucose is lt;250 mg/dL (13.9 mmol/L) or is predicted to fall to lt;200 mg/dL (11.1 mmol/L) in 1 hour. Use of a separate dextrose-containing fluid bag allows fluid resuscitation and glucose infusion to be titrated separately (two-bag approach) and has been shown to result in shorter duration of treatment.20
î Serial measurements of #946;-hydroxybutyrate in addition to electrolytes may provide additional information about recovery. Restoration of renal buffering capacity by normalization of the serum bicarbonate level is the most reliable index of metabolic recovery. Note that hyperchloremia may cause closure of the anion gap before the serum bicarbonate level has normalized, making anion gap closure a less reliable indicator of recovery of DKA than serum bicarbonate.
î Telemetry is recommended given the propensity for electrolyte abnormalities.
• IV antimicrobial therapy should be started promptly for documented or suspected bacterial, fungal, and other treatable infections. Empiric broad-spectrum antibiotics can be started in septic patients pending results of blood cultures. Note that DKA is not typically accompanied by fever, so infection must be considered in a febrile patient.
Complications
Complications of DKA include life-threatening conditions that must be recognized and treated promptly.
• Lactic acidosis may result from prolonged dehydration, shock, infection, and tissue hypoxia in DKA patients. Lactic acidosis should be suspected in patients with refractory metabolic acidosis and a persistent anion gap despite optimal therapy for DKA. Management includes adequate volume replacement, control of sepsis, and judicious use of bicarbonate.
• Arterial thrombosis manifesting as stroke, MI, or an ischemic limb occurs with increased frequency in DKA.
However, anticoagulation only indicated as specific therapy for a thrombotic event.• Cerebral edema is observed more frequently in children than adults.
î Symptoms of increased intracranial pressure (e.g., headache, altered mental status, papilledema) or a sudden deterioration in mental status after initial improvement in a patient with DKA should raise suspicion for cerebral edema.
î Overhydration with free water and excessively rapid correction of hyperglycemia are known risk factors. Watch for a decrease in serum sodium level or failure to rise during therapy.
î Neuroimaging with a CT scan can establish the diagnosis. Prompt recognition and treatment with IV mannitol is essential and may prevent neurologic sequelae in patients who survive cerebral edema.
• Rebound ketoacidosis can occur because of premature cessation of IV insulin infusion or inadequate doses of subcutaneous (SC) insulin after the insulin infusion has been discontinued. All patients with T1DM and patients with T2DM who develop DKA (indicating severe insulin deficiency) require both basal and premeal insulin in adequate doses to avoid recurrence of metabolic decompensation. Basal insulin should be administered 2 hours prior to discontinuation of IV insulin.