Hyperosmolar Hyperglycemic State
GENERAL PRINCIPLES
HHS is one of the most serious life-threatening complications of T2DM.
Epidemiology
• HHS occurs primarily in patients with T2DM. In 30%-40% of cases, it is the initial presentation of a patient's diabetes.
• HHS is significantly less common than DKA, with an incidence of lt;1 case per 1000 person-years.21
Pathophysiology
• Ketoacidosis is absent because the ambient insulin level may effectively prevent lipolysis and subsequent ketogenesis while being inadequate to facilitate peripheral glucose uptake and to prevent hepatic residual gluconeogenesis and glucose output.
• Precipitating factors for HHS include dehydration, stress, infection, stroke, noncompliance with medications, dietary indiscretion, and alcohol and cocaine abuse. Impaired glucose excretion is a contributory factor in patients with renal insufficiency or prerenal azotemia.
DIAGNOSIS
Clinical Presentation
In contrast to DKA, the onset of HHS is usually insidious. Several days of deteriorating glycemic control are followed by increasing lethargy. Clinical evidence of severe dehydration is the rule. Some alterations in consciousness and focal neurologic deficits may be found at presentation or may develop during therapy. Therefore, repeated neurologic assessment is recommended.
Differential Diagnosis
The differential diagnosis of HHS includes any cause of altered level of consciousness, including hypoglycemia, hyponatremia, severe dehydration, uremia, hyperammonemia, drug overdose, and sepsis. Seizures and acute stroke-like syndromes are common presentations.
Diagnostic Testing
Clinical findings include (1) hyperglycemia, often gt;600 mg/dL (33.3 mmol/L); (2) plasma osmolality gt;320 mOsm/L; (3) absence of ketonemia; and (4) pH gt; 7.3 and serum bicarbonate level of gt;20 mEq/L (gt;15 mmol/L in UK guidelines). Prerenal azotemia and lactic acidosis can develop.
Although some patients will have detectable urine ketones, most patients do not have a metabolic acidosis. Lactic acidosis may develop from an underlying ischemia, infection, or other cause.TREATMENT
• See Table 23-3 for detailed treatment recommendations.
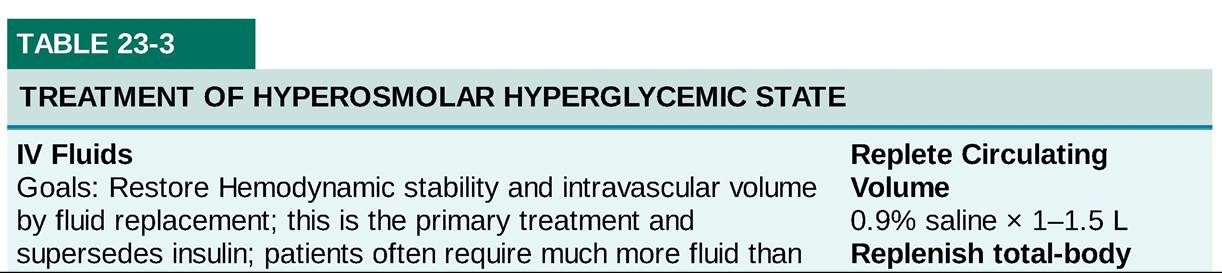
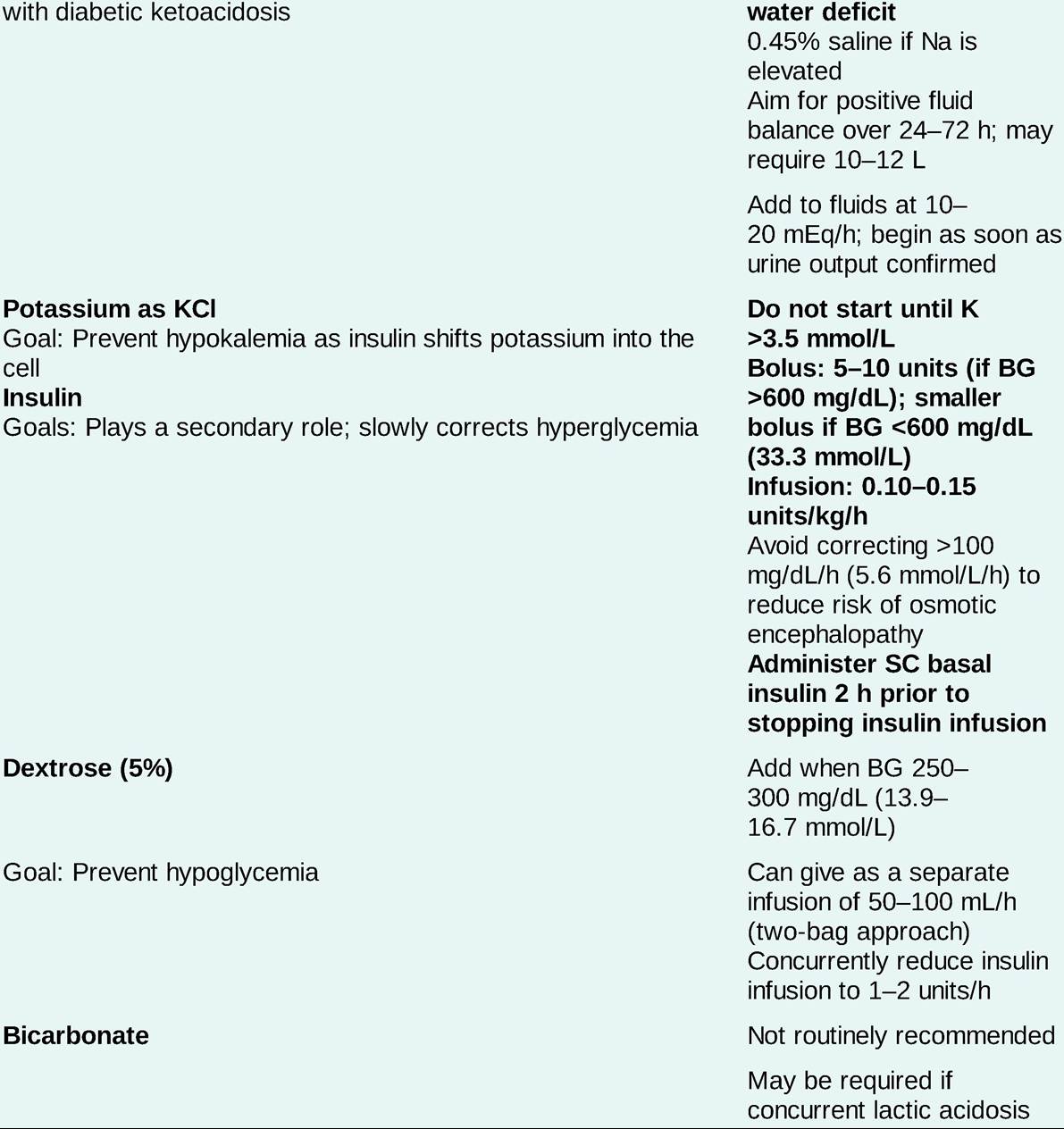
BG, blood glucose; K, potassium; KCl, potassium chloride.
• Underlying illness: Detection and treatment of any underlying predisposing illness are critical in the treatment of HHS. Antibiotics should be administered early, after appropriate cultures, in patients in whom infection is known or suspected as a precipitant to HHS. A high index of suspicion should be maintained for underlying pancreatitis, GI bleeding, renal failure, and thromboembolic events, especially acute MI.
Complications
Complications of HHS include thromboembolic events (cerebral and MI, mesenteric thrombosis, pulmonary embolism, and disseminated intravascular coagulation), cerebral edema, acute respiratory distress syndrome, and rhabdomyolysis.
Monitoring/Follow-Up
• Monitoring of therapy: Use of a flowchart is helpful for tracking clinical data and laboratory results.
• Initially, BG levels should be monitored every 30-60 minutes and serum electrolyte levels every 2-4 hours; frequency of monitoring can be decreased during recovery.
• Neurologic status must be reassessed frequently; persistent lethargy or altered mentation indicates inadequate therapy. On the other hand, relapse after initial improvement in mental status suggests too rapid correction of serum osmolarity.