Type 1 Diabetes
GENERAL PRINCIPLES
A comprehensive approach is necessary for successful management of T1DM. A team approach that includes the expertise of physicians, diabetes educators, dietitians, and other members of the diabetes care team offers the best chance of success.
DIAGNOSIS
T1DM can present at any age, and because of the variable time course and severity of hyperglycemia, the diagnosis can be challenging in adults.
• The rate of destruction of #946; cells is rapid in infants and children and slower in adults. Therefore, ketoacidosis as an initial presentation is more common in young patients.
• T1DM is characterized by severe insulin deficiency. Exogenous insulin is required to control BGs, prevent DKA, and preserve life. Ketosis develops in 8-16 hours and ketoacidosis in 12-24 hours without insulin.
• Early in the course of T1DM, some insulin secretory capacity remains, and the insulin requirement may be lower than expected (0.3-0.4 units/kg). Tight control of BG level from the onset has been shown to preserve the residual #946;-cell function and prevent or delay later complications.
• Latent autoimmune diabetes in adults (LADA) is characterized by mild to moderate hyperglycemia at presentation that often responds to noninsulin therapies initially. Adults with LADA will have one or more #946; cell-specific autoantibodies and tend to require insulin therapy sooner than patients with classic T2DM (months to years).
• T1DM should be suspected when there is a family history of T1DM, thyroid disease, celiac disease or other autoimmune disease. Presentation with ketoacidosis suggests T1DM, but confirmatory tests may be useful to guide therapy.
• Autoantibodies include islet cell autoantibodies, antibodies to insulin, antibodies to glutamic acid decarboxylase (anti-GAD), antibodies to zinc transporter 8 (ZnT8), and antibodies to tyrosine phosphatases IA-2 and IA-2#946;.
Measuring one or more of these autoantibodies along with a C-peptide can help to confirm the diagnosis of T1DM; however, 20% of insulin-deficient adults are antibody negative.TREATMENT
Treatment of T1DM requires lifelong insulin replacement and careful coordination of insulin doses with food intake and activity.22
• A regimen of multiple daily insulin injections that include basal, premeal, and correction doses is preferred to obtain optimal control in both hospitalized patients and outpatients. This regimen implies that capillary glucose monitoring will occur four times daily, 10-30 minutes before meals and at bedtime or that a patient is using a CGM device.
î The insulin requirement for optimal glycemic control is approximately 0.5-0.8 units/kg/d for the average nonobese patient. A conservative total daily dose (TDD) of 0.4 units/kg/d is given initially to a newly diagnosed patient; the dose is then adjusted, using SMBG values. Higher doses may be required in obese or insulin-resistant patients, in adolescents, and in the latter part of pregnancy.
î Basal insulin (administered as NPH twice daily, detemir once or twice daily, glargine once or twice daily, or insulin degludec once daily) should provide 40%-50% of the TDD of insulin and should be adjusted by 5%-10% daily until the fasting glucose is consistently lt;130 mg/dL (7.2 mmol/L). In general, basal insulin is given regardless of nothing by mouth (NPO) or dietary status and should not be held without a direct order.
î Premeal insulin doses of insulin are given to cover caloric intake at meals or with snacks. Bolus doses are adjusted according to the BG, the anticipated carbohydrate intake, and the anticipated activity level. The total premeal complement should roughly equal the total basal dose, with one- third given before or after each meal. Rapid-acting insulins (lispro, aspart, glulisine, or inhaled technosphere insulin) are preferred, but regular human insulin can be used. There are now ultrarapid forms of lispro and aspart with a faster onset of action and earlier peak action.23
î The third component of a comprehensive insulin regimen is “correction factor” insulin, which is similar to sliding scale. This category of insulin therapy is adjusted according to the premeal fingerstick glucose testing (or CGM reading) and the patient's estimated insulin sensitivity.
In general, patients with lower BMI should use a less aggressive scale than patients with higher BMI or more insulin-resistant patients. Correction factor and premeal doses should use the same insulin and be given together in the same syringe. At times, a correction dose of rapid-acting insulin may be needed to treat hyperglycemia in the absence of food intake.• Insulin preparations: After SC injection, there is individual variability in the duration and peak activity of insulin preparations and day-to-day variability in the same subject (Table 23-4).
TABLE 23-4
APPROXIMATE KINETICS OF INSULIN PREPARATIONS
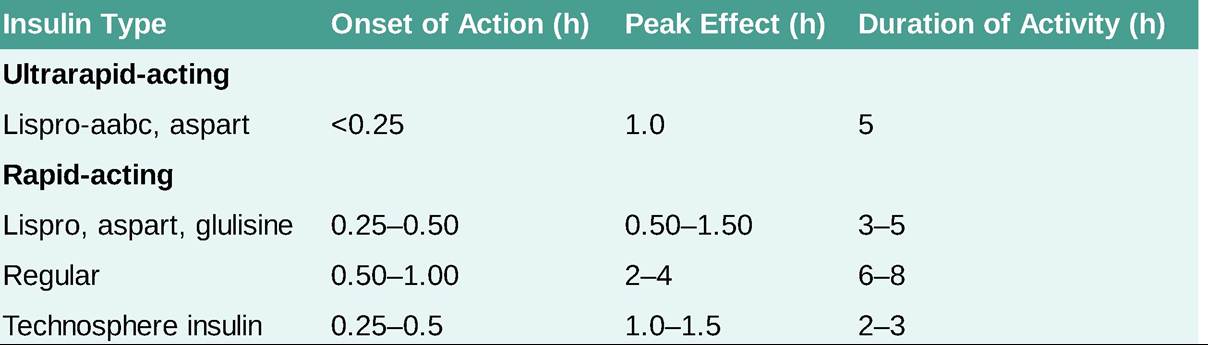
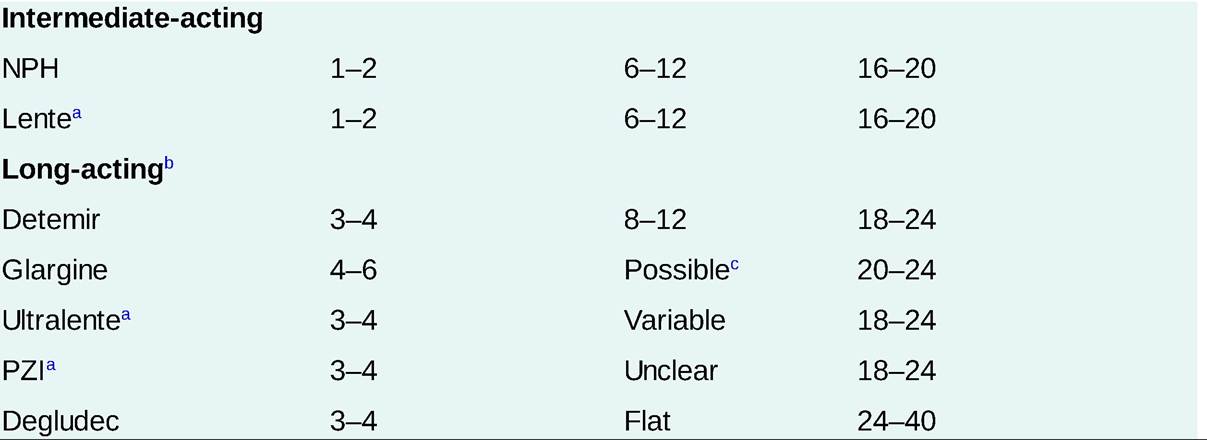
NPH, neutral protamine Hagedorn; PZI, protamine zinc insulin.
aNot available in the United States; possibly generic manufacturers.
bSome patients with type 1 diabetes have improved control when the long-acting basal insulin is given twice a day rather than once daily.
cInsulin dosage and individual variability in absorption and clearance rates affect pharmacokinetic data. Duration of insulin activity is prolonged in renal failure. After a lag time of approximately 5 hours, insulin glargine generally has a mostly flat peakless effect over a 22- to 24-hour period; however, broad peaks can occur. Insulin degludec has the longest duration of action, allowing administration at any time of the day.
• SC insulin administration: The abdomen, thighs, buttocks, and upper arms are the preferred sites for SC insulin injection. Absorption is fastest from the abdomen, followed by the arm, buttocks, and thigh, probably as a result of differences in blood flow. Injection sites should be rotated within the regions, rather than randomly across separate regions, to minimize erratic absorption. Exercise or massage over the injection site may accelerate insulin absorption.
• Regular human insulin is available in an inhaled form as technosphere insulin. This comes in 4-, 8-, and 12-unit cartridges for bolus dose insulin administration. Onset occurs at 0.2-0.25 hour with peak effect within the first hour and a duration of action of 3 hours. It is contraindicated in patients with asthma or chronic obstructive pulmonary disease because of risk of bronchospasm. Pulmonary function tests are required prior to starting and at regular intervals during therapy.
• Continuous SC insulin infusion with an insulin pump is widely used for insulin delivery in patients with T1DM, and increasingly in T2DM. Use of an insulin pump integrated with CGM adds additional features. Sensor augmented pump (SAP) therapy allows automated suspension of insulin delivery on reaching a preset low threshold, or above the threshold if glucose is declining and predicted to reach a hypoglycemic value within a specified period. Hybrid closed loop (HCL) systems allow the basal rate to automatically adjust according to CGM data while the patient continues to input bolus dosing information.
î A typical regimen provides 50% of total daily insulin as basal insulin and the remainder as multiple preprandial bolus doses of insulin. A rapid-acting insulin (aspart, lispro, or glulisine) is used to fill the pump and is infused continuously to provide basal insulin.
° Insulin pumps have advanced features that allow patients to fine-tune their basal and bolus doses but require diabetes education to use the pump to its full potential. Patients must check their blood sugars regularly because DKA can occur rapidly if the insulin infusion is disrupted (i.e., faulty infusion set).
î SAP and HCL systems are currently available. Fully closed loop systems, whereby the patient will not manually enter information, are being developed.