Type 2 Diabetes
GENERAL PRINCIPLES
• T2DM results from defective insulin secretion followed by loss of #946;-cell mass in response to increased demand as a result of insulin resistance.24
• T2DM is usually diagnosed in adults, with both incidence and prevalence increasing with age.
However, type 2 diabetes prevalence has increased substantially since 2001 in youth aged 10-19, comprising about 20% of cases of diabetes in that age group in 2017.25• T2DM is associated with obesity, family history of diabetes, history of GDM or prediabetes, hypertension, physical inactivity, race/ethnicity, and other social determinants of health (socioeconomic status, food insecurity). African Americans, Latinos, Asian Indians, Native Americans, Pacific Islanders, and some groups of Asians have a greater risk of developing T2DM than Caucasians.
• T2DM may be asymptomatic and, therefore, can remain undiagnosed for months to years.
• The loss of pancreatic #946; cells is progressive. Insulin secretion is usually sufficient to prevent ketosis, but DKA or HHS can develop during severe stress. T2DM in patients who present with or later develop ketosis or DKA, but who do not require insulin between episodes, is termed ketosis-prone T2DM.
• The mechanisms underlying the #946;-cell loss and defective insulin secretory dysfunction in T2DM are not clear, but cell death, transdifferentiation, and de-differentiation in response to oxidative stress and endoplasmic reticulum stress in the setting of environmental exposure and genetic predisposition have been proposed. Glycemic state may also affect the beta cell over prolonged periods of time.26
TREATMENT
• The achievement of glycemic control requires individualized therapy and a comprehensive approach that incorporates lifestyle and pharmacologic interventions. Guidelines have been published by several professional organizations regarding the choice and sequence of antidiabetic therapy.27
• Considerations for selecting noninsulin therapy (Table 23-5) in patients with T2DM include the following:
î Pharmacologic therapy should be initiated early in conjunction with diet and exercise.
TABLE 23-5
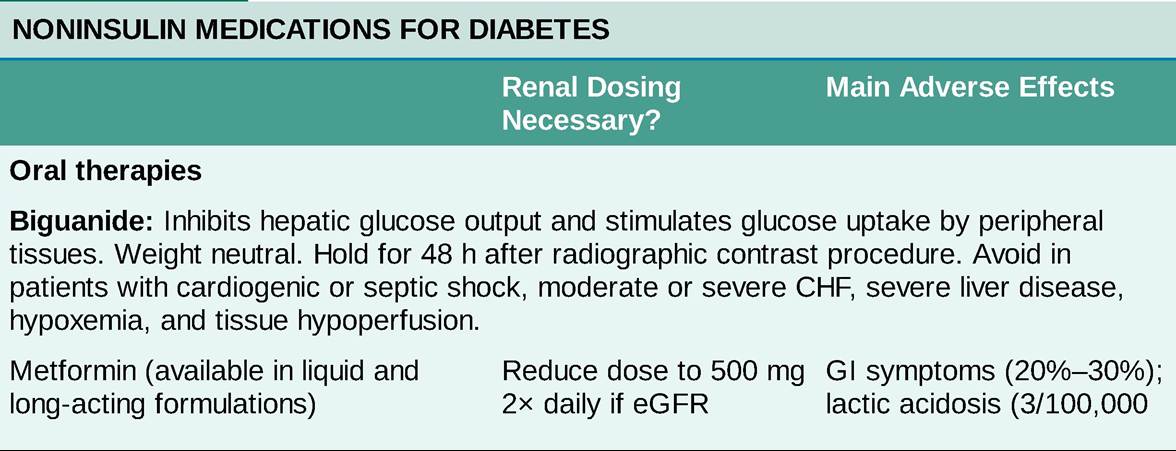
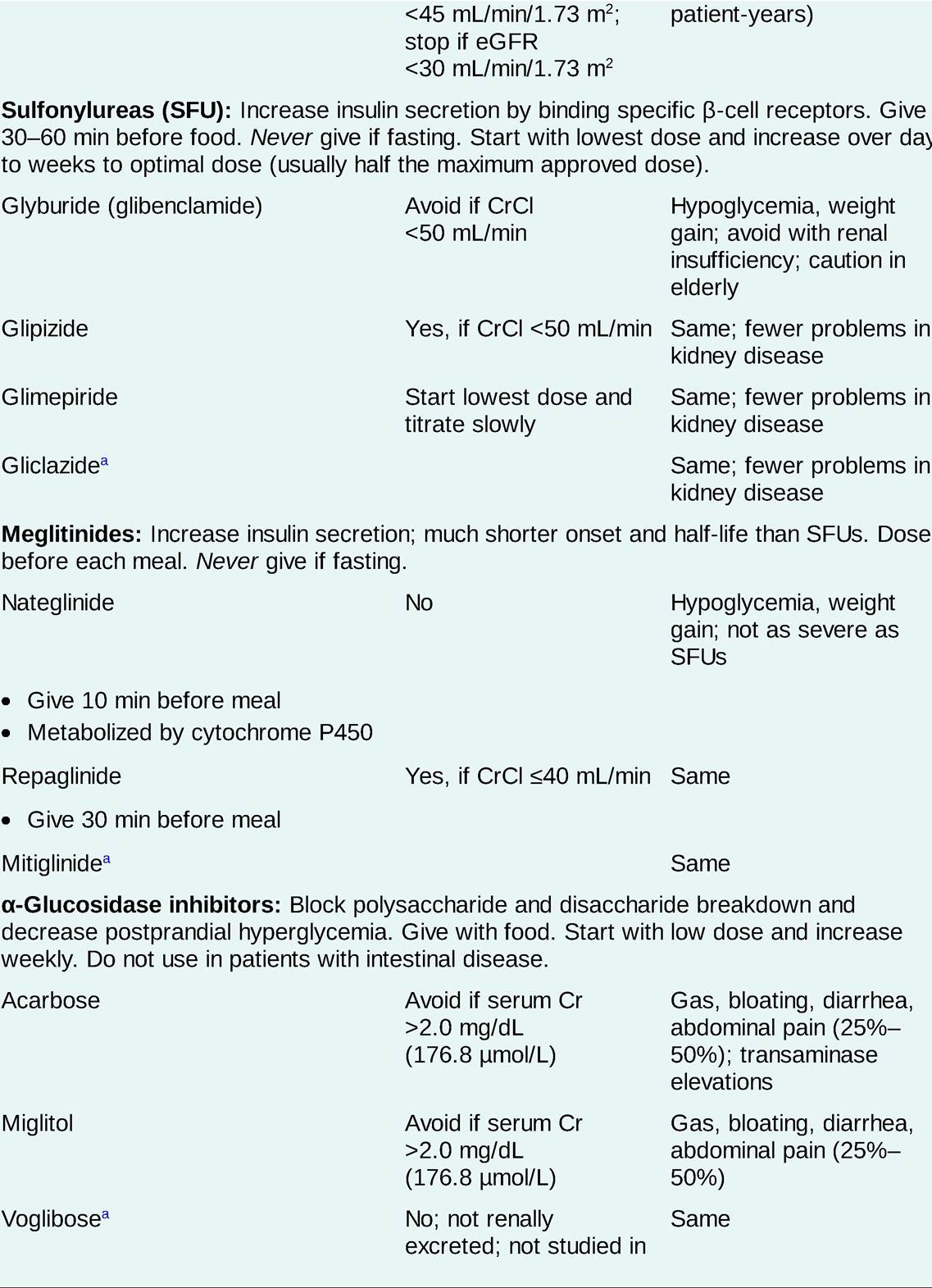
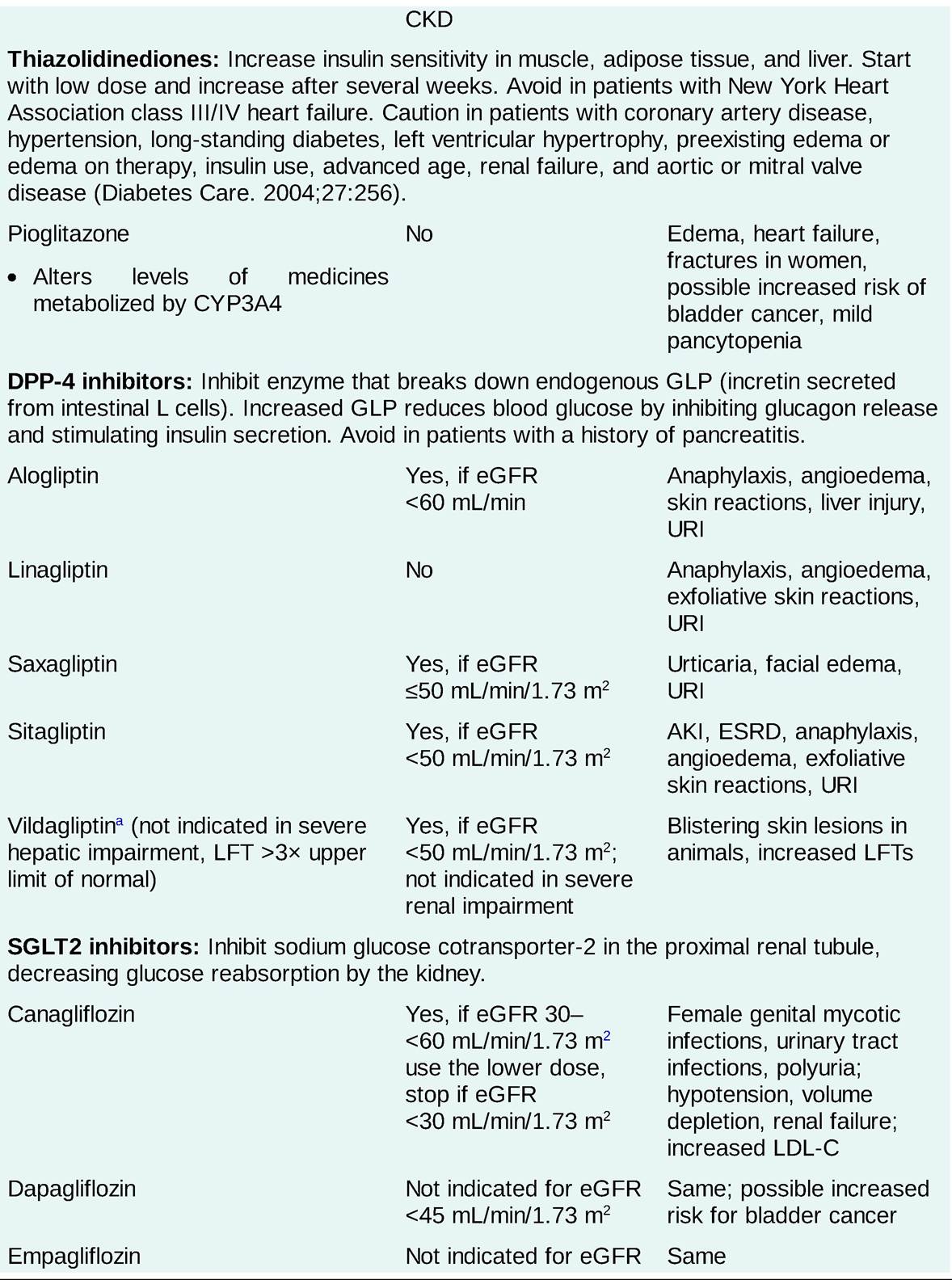
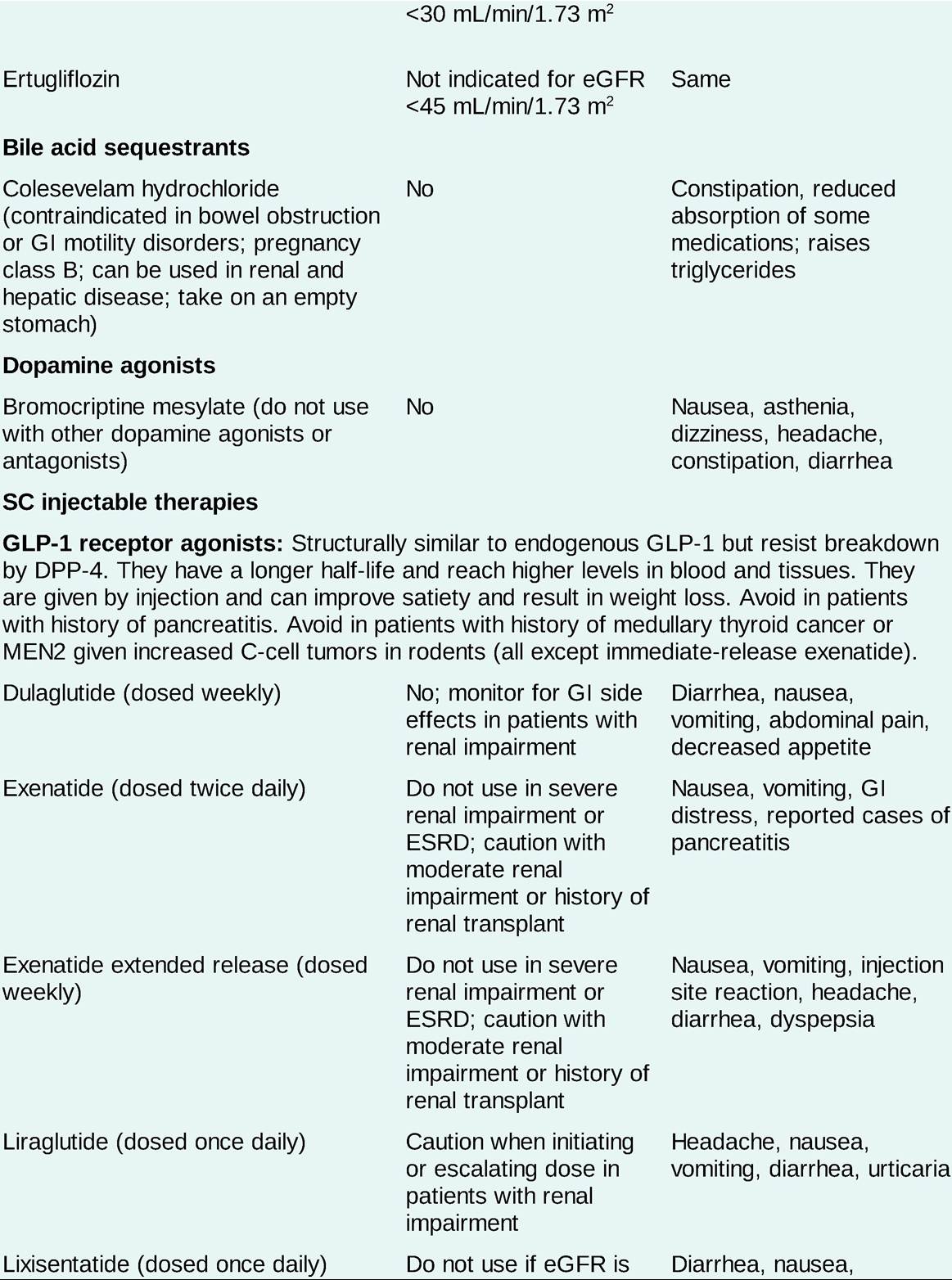
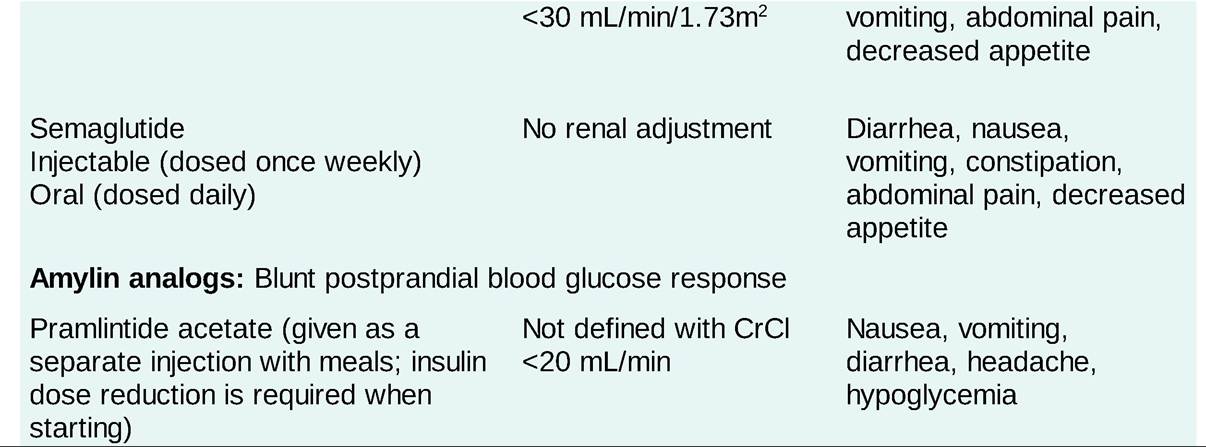
AKI, acute kidney injury; CKD, chronic kidney disease; CHF, congestive heart failure; Cr, creatinine; CrCl, creatinine clearance; DPP-4, dipeptidyl peptidase 4; eGFR, estimated glomerular filtration rate; ESRD, end-stage renal disease; GI, gastrointestinal; GLP, glucagon-like peptide; LDL-C, low-density lipoprotein cholesterol; LFT, liver function test; MEN2, multiple endocrine neoplasia type 2; URI, upper respiratory infection.
Please refer to country-specific prescribing information before using any of the antidiabetes therapies.
aNot available in the United States.
î Metformin is the recommended first-line therapy if tolerated.
î Based upon results of the cardiovascular outcome trials, GLP-1 receptor agonists should be considered first-line in individuals with cardiovascular disease or stroke. SGLT2 inhibitors should be considered first-line in individuals with heart failure or diabetic kidney disease.
î The glucose-lowering effects of metformin, insulin secretagogues, DPP-4 inhibitors GLP-1 receptor analogs, and SGLT2 inhibitors are observed within days to weeks, whereas the maximum effect of thiazolidinediones may not be observed for several weeks to months.
î Combination therapy with two or more oral or injectable agents may be needed at the time of diagnosis to achieve A1C and glucose targets in patients presenting with significant hyperglycemia (A1C gt;9%; 75 mmol/mol) and will likely be needed as #946;-cell function deteriorates over time.
î Insulin therapy should be considered for patients presenting in DKA or with very high glucose levels (A1C gt;10%; 86 mmol/mol).
Insulin therapy can sometimes be stopped after glucose toxicity is corrected but may need to be continued in patients with persistent insulin deficiency.î Because pancreatic #946;-cell function is required for the glucose-lowering effects of all noninsulin therapies, many patients will require insulin replacement therapy at some point. Insulin therapy can be initiated with basal insulin in addition to other therapies.
î The toxicity profile of some oral and injectable antidiabetic agents may preclude their use in patients with preexisting illnesses.
î Doses of noninsulin therapies may need to be reduced for declining kidney function (Table 23-5).
î Cardiovascular outcome trials (CVOTs) comparing anti-hyperglycemic medications versus placebo have shown that none increase the risk of CVD. Studies with DPP-4 inhibitors have shown CVD safety but no benefit.
î In a meta-analysis of CVOTs, GLP-1 receptor agonists reduced major adverse cardiovascular events, all-cause mortality, composite kidney outcomes, and heart failure.28
î In meta-analysis of CVOTs, SGLT2 inhibitors reduced the risk of hospitalization for heart failure and cardiovascular death and reduced progression of renal disease. Major adverse cardiovascular events were reduced in those with preexisting cardiovascular disease.29
• Insulin therapy in T2DM is indicated in the following:
î Patients in whom oral or injectable agents have failed to achieve or sustain glycemic control
î Metabolic decompensation: DKA, HHS
î Newly diagnosed patients with severe hyperglycemia
î Patients with chronic kidney disease that precludes use of noninsulin therapies
î Pregnancy and other situations in which oral agents are contraindicated
• The success of insulin therapy depends on both the adequacy of the insulin TDD (0.6 to gt;1.0 units/kg of body weight per day) and the appropriateness of the insulin regimen for a given patient to achieve target glucose and A1C values.
î A once-daily injection of intermediate- or long-acting insulin at bedtime or before breakfast (basal insulin) added to oral or injectable agents may achieve the target A1C goal.
î Premeal insulin may be required if basal insulin plus other agents are not adequate. Short- or rapidacting insulin administered before meals can be added to basal insulin. Alternatively, a premixed insulin can be given twice daily before breakfast and dinner. In general, the secretagogues are discontinued when premeal insulin is added, but sensitizing and other agents are continued based on individual patient needs.
î The TDD of insulin required to achieve glycemic targets varies widely in patients with T2DM and is based on BMI, the continuation of oral agents, and the presence of comorbid conditions. Large doses of insulin (gt;100 units/d) may be required for optimal glycemic control. Weight gain with insulin use is a concern.
î Insulin-induced hypoglycemia, the most dangerous side effect, may increase CV event rates and death. Avoidance of hypoglycemia while achieving an A1C as low as can be safely achieved requires close collaboration between physician, patient, and diabetes educators. The frequency of hypoglycemia increases as patients approach normal A1C levels or when kidney function declines.
• Concentration: The standard insulin concentration is 100 units/mL (U-100), with vials containing 1000 units in 10 mL. A highly concentrated form of regular insulin containing 500 units/mL (Humulin U-500) is available for patients with severe insulin resistance (usually T2DM) requiring more than 200 units per day. The vial size for U-500 insulin is 20 mL. Pens containing 3 mL are also available for U- 100 and U-500 insulins. Concentrated forms of insulin glargine, a formulation that is 300 units/mL (U- 300), insulin degludec, and insulin lispro formulated with 200 units/mL (U-200), are available in pens.
• Mixed insulin therapy: Short- and rapid-acting insulins (regular, lispro, aspart, and glulisine) can be mixed with NPH insulin in the same syringe for convenience. The rapid-acting insulin should be drawn first, cross-contamination should be avoided, and the mixed insulin should be injected immediately. Commercial premixed insulin preparations do not allow dose adjustment of individual components but are convenient for patients who are unable or unwilling to do the mixing themselves. Premixed insulins are an option for patients with T2DM who have a regular eating and activity schedule and, in general, should not be used in T1DM. Premixed insulins are not advised for use in hospitalized patients.
More on the topic Type 2 Diabetes:
- Type 2 Diabetes
- Diabetes Mellitus
- Type 1 Diabetes
- 22.7 DIABETES MELLITU
- Diabetes Mellitus
- OBESITY
- Focal Segmental Glomerulosclerosis
- Congenital Fiber-Type Size Disproportion
- Pathology of Insulin Signaling and Adipose Tissue
- Nonalcoholic Fatty Liver Disease