Hemoptysis
GENERAL PRINCIPLES
Hemoptysis is the coughing up of blood or blood-stained mucus. It is a sign of underlying pulmonary pathology. It can be life threatening and requires rapid identification, workup, and treatment.
Definition
• True hemoptysis is expectoration of blood from the lower respiratory tract below the glottis.
• Massive or life-threatening hemoptysis:
î Is usually defined by volume per unit time.
î It is most commonly defined as >600 mL of blood expectorated per 24 hours. 119, 120
î Vblumes of >100 mL in 24 hours associated with gas exchange abnormality, airway obstruction, or
hemodynamic instability are also considered life threatening.
Classification
Clinically, hemoptysis is usually classified as being massive/life threatening or not (see above). It may also be classified by the anatomic location of the bleeding.
• Airway
• Parenchyma
• Vascular
• Combination
There are various other classifications in the literature based on appearance, frequency, rate, volume, and potential for clinical consequences of the hemoptysis that may suggest an underlying etiology or predict outcome and thus help guide in diagnosis and management. However, considerable overlap exists in the clinical presentation both within and between etiologies.
Etiology
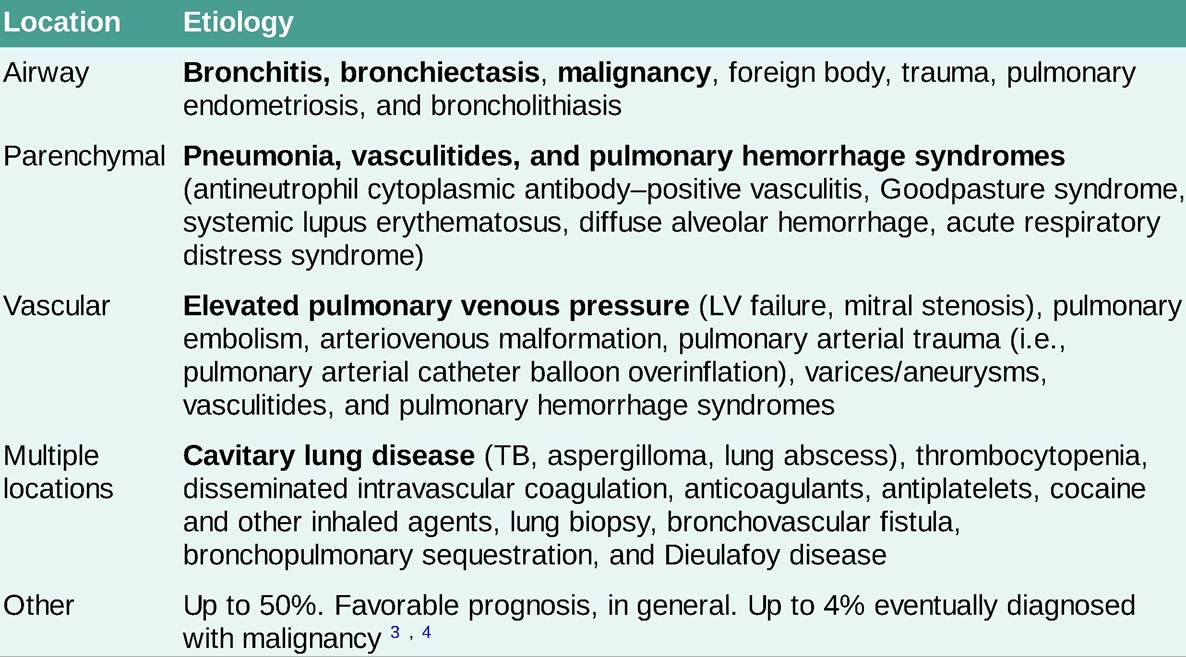
See Table 10-9.
TABLE 10-9
ETIOLOGY OF HEMOPTYSIS
Epidemiology
The incidence of each cause of hemoptysis varies considerably. Table 10-10 lists some of the most common causes of hemoptysis. 121, 122
| EPIDEMIOLOGY OF HEMOPTYSIS | |
| Etiology | Incidence (%) |
| Bronchitis | 2-37 |
| Bronchiectasis | 1-37 |
| TB and cavitary lung disease | 2-69 |
| Malignancy | 2-24 |
| Pneumonia | 1-16 |
| Pulmonary embolus | 3 |
| Pulmonary edema | 4 |
| Idiopathic | 2-50 |
Pathophysiology
The source of hemoptysis depends on the etiology and location of the underlying pathologic process.
• The pulmonary arterial circulation supplies 99% of all blood flow to the lung parenchyma under low pressure. Disruption can result in minor hemoptysis or more life-threatening hemoptysis due to processes such as vasculitis, diffuse alveolar hemorrhage, pulmonary embolism, acute respiratory distress syndrome, arteriovenous malformation (AVM) rupture, pulmonary artery catheter trauma, severe mitral stenosis, LV failure, or Rasmussen aneurysm (pulmonary artery aneurysm associated with TB).
• The bronchial arterial circulation arises from the aorta and intercostal arteries. It supplies high- pressure blood flow to the lungs but accounts for only 1% of pulmonary blood flow. Disruption by a foreign body, tumor invasion, fungal invasion, or denuded airway mucosa can result in massive, lifethreatening hemoptysis. Bleeding from the bronchial circulation may account for up to 88% of all cases of massive hemoptysis.
DIAGNOSIS
Identifying and correcting the underlying pathologic process is the basis of diagnosis and management of hemoptysis (Figure 10-5).
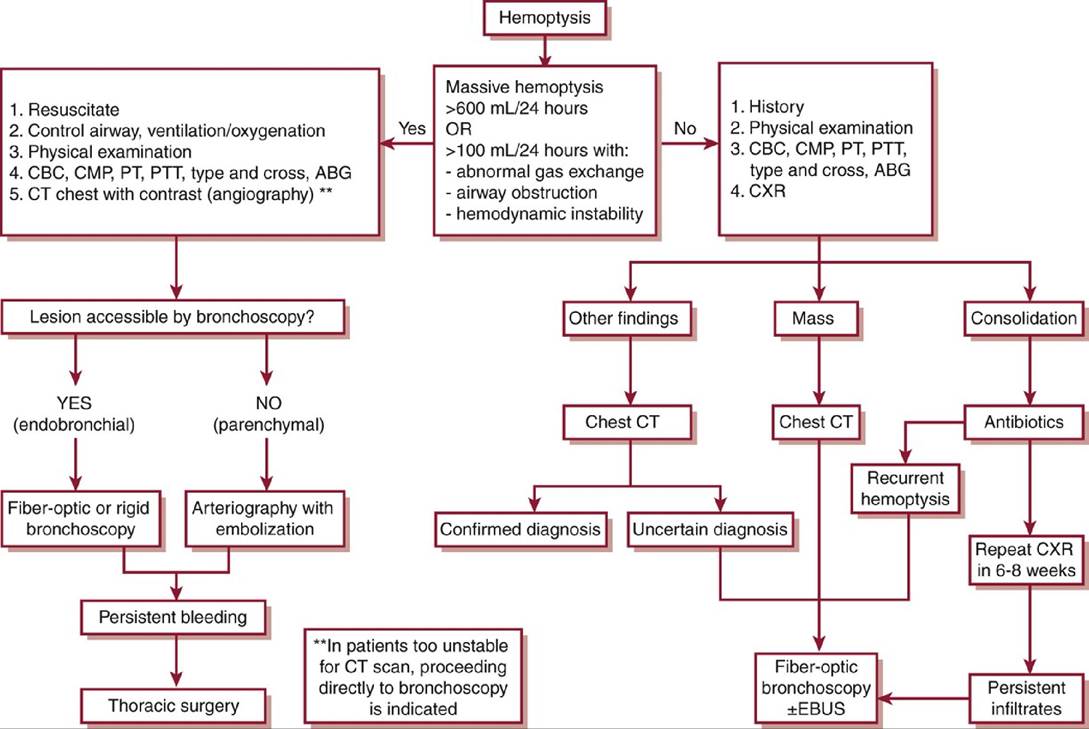
Figure 10-5 Algorithm for evaluation of hemoptysis.ABG, arterial blood gas; CBC, complete blood count; CMP, complete metabolic panel; EBUS, endobronchial ultrasound; PT, prothrombin time; PTT, partial thromboplastin.(Adapted from Earwood JS, Thompson TD. Hemoptysis: evaluation and management. Am Fam Physician. 2015;91:243-249.)
Clinical Presentation
Hemoptysis may present in isolation or accompany other manifestations of an underlying disorder (Table 10-9). The appearance, timing, and volume of hemoptysis can provide important clues to narrowing the differential diagnosis.
• Appearance: Gross blood, blood-tinged sputum, blood-streaking, foamy pink sputum
• Timing: First episode, recurrent episodes, chronic small volumes, acute large volumes
• Vblume: Minor, submassive, massive
HISTORY
• The most important facts to gather include volume of hemoptysis, patient age, smoking history, prior lung disease, previous malignancy, risk factors for coagulopathy, and prior episodes of hemoptysis.
• Review of systems should focus on symptoms suggesting cardiopulmonary disease, active infection, underlying malignancy, and systemic inflammatory disorders.
PHYSICAL EXAMINATION
• Obtaining vital signs including oxygen saturation is the first step in patient examination.
• Thereafter, one should pay attention to the patient's general state of health, lung examination noting focal or diffusely abnormal findings such as bronchial breath sounds, crackles, stridor, and/or expiratory wheezes.
A thorough examination should always be performed, observing any manifestations suggesting underlying cardiopulmonary, infectious, immunologic, or malignant disease.
Differential Diagnosis
One must distinguish between true hemoptysis and pseudohemoptysis, which comes from the upper airway (above the glottis), or aspirated GI tract bleeding that is later expectorated.
Diagnostic Testing
• A thorough history and physical examination is important to provide clues and guidance in additional testing.
• Additional testing is aimed at determining and localizing the bleeding source and identifying the underlying etiology.
LABORATORIES AND ELECTROCARDIOGRAPHY
• Basic lab work including CBC, comprehensive metabolic panel, and coagulation studies are indicated.
• Type and cross-matching of blood are indicated, especially in cases of massive hemoptysis.
• An ABG analysis may be indicated in cases of shortness of breath or respiratory compromise.
• Sputum studies may be helpful in cases of infection and can be analyzed with routine Gram stain and culture, fungal culture, and acid-fast bacilli smear/culture as indicated.
• Serologic studies and urinalysis with microscopy may be clinically indicated based on the suspicion for rheumatologic disease or vasculitis. These may include ANA screen, antineutrophil cytoplasmic antibody (ANCA) screen, including reflex testing to myeloperoxidase and proteinase 3, antiglomerular basement membrane antibodies, complement levels, cryoglobulins, double-stranded DNA antibodies, and others.
• Brain natriuretic peptide or N-terminal pro b-type natriuretic peptide levels may be helpful when cardiac failure is suspected.
• ECG can help assess for underlying cardiac disease.
IMAGING
• Posteroanterior and lateral CXR are performed in all cases of hemoptysis.
î Unfortunately, these may be normal or nonlocalizing in up to 50% of all cases. 123, 124
î Furthermore, CXR may be normal in up to 10% of hemoptysis cases caused by bronchogenic carcinoma. 123
• Chest CT: CT should be performed if the diagnosis remains in doubt after initial clinical and CXR evaluation (see Figure 10-5). CT chest can be performed with or without contrast; however, CT angiography is increasingly useful in localizing the source of hemoptysis.
î Advantages:
■ Can visualize parenchyma, vasculature, and airways to varying extent.
■ Especially useful for hemoptysis resulting from bronchiectasis, cavitary lung disease, masses, and vascular malformations. 125
■ Can detect up to 96% of CXR-occult malignancies. 126
■ CT visualizes tumors with efficacy comparable with bronchoscopy. 127
■ CT angiography may be better than bronchoscopy in determining the etiology and source of hemoptysis. 128
■ CT angiography is useful for planning embolization procedures. 129
î Disadvantages:
■ CT is less efficacious than bronchoscopy in recognizing subtle bronchial and mucosal lesions. 125
■ It is nonspecific in cases of parenchymal/alveolar hemorrhage.
■ Delay in treatment places unstable patients at high risk.
• Echocardiography may be performed if structural or valvular cardiac disease is suspected.
DIAGNOSTIC PROCEDURES
• Fiber-optic (flexible) bronchoscopy: Generally localize s/lateralizes bleeding source in over two- thirds of cases, depending on the setting. 130
î Indications:
■ If the source is unclear after initial evaluation and imaging
■ Persistent or recurrent hemoptysis
■ To rule out infection
■ If the clinical presentation suggests an airway abnormality
■ To obtain biopsy specimens, if imaging suggests malignancy or is nonlocalizing in the presence of at least two risk factors for bronchogenic carcinoma:
? Male sex
? Age >40 years
? >40 pack-year smoking
? Duration of hemoptysis >1 week
? Vblume expectorated >30 mL 6, 131, 132
■ To identify potential anatomic area for arterial embolization
■ To provide endobronchial treatments
■ To rule out alveolar hemorrhage
î The timing of bronchoscopy is controversial, although yields increase when performed during or within 48 hours of bleeding.
131• Bronchial and pulmonary arteriography is performed in the setting of persistent, recurrent, or massive hemoptysis.
î Advantages:
■ Can be both diagnostic and therapeutic via simultaneous embolization of the visualized culprit vessel.
■ Useful in hemoptysis of varying degrees in the setting of different etiologies including bronchiectasis, malignancy, aspergilloma, and others. 133
■ Can be preceded by CT angiography for procedure planning. 129
î Disadvantages:
■ Variable and inexact localization of the bleeding source depending on clinical setting. 130
■ Anatomic variability.
■ Bleeding in cases where it is insufficient for contrast extravasation.
TREATMENT
The approach to hemoptysis is primarily aimed at distinguishing massive/life-threatening hemoptysis from nonmassive hemoptysis. The three main goals are:
.. to stabilize the patient's airway and hemodynamics,
:. to diagnose the cause and localize the site of hemoptysis, and
ł. to decide on need for and type of therapy in each case.
• Nonmassive hemoptysis is usually treated conservatively. Treatment may include the following:
î Reversal of coagulopathy
î Antitussives
î Bronchoscopy if recurrent
î Steroids and/or immunosuppression for rheumatologic conditions
î Antibiotics for infection (fungal, TB, mycobacteria)
î Diuretics and/or inotropes for heart disease (LV failure, mitral stenosis)
• Massive hemoptysis: management requires urgent action, intensive care monitoring, and an early multidisciplinary approach including an interventional pulmonologist, a thoracic surgeon, and an interventional radiologist (see Figure 10-5).
î Initial stabilization:
■ Airway management may require intubation, with a large (>8 mm) endotracheal tube. 134
? Single-lumen main stem intubation for selective ventilation of unaffected lung.
? Double-lumen endotracheal intubation for selective ventilation of unaffected lung.
Should be performed and managed only under appropriately skilled supervision.■ Lateral decubitus positioning (affected lung down) to minimize aspiration into unaffected lung.
■ Inhaled tranexamic acid may reduce volume of expectorated blood, reduce hospital length of stay, lead to more frequent resolution of hemoptysis, reduce recurrence rates, and reduce the need for invasive procedures, without increased adverse effects noted. More investigation is needed on this intervention. 135
î Bronchoscopy with directed airway therapy: Rigid bronchoscopy is favored if available because it provides optimal airway access and ventilatory control and easier suctioning and allows for manipulation of instruments.
■ Direct tamponade with the distal end of the bronchoscope.
■ Balloon tamponade: Left in place for 1-2 days. Monitor for ischemic mucosal injury or postobstructive pneumonitis. 136 Fogarty balloons, bronchial blockers, and pulmonary artery catheter balloons have all been described for tamponading bleeding.
■ Endobronchial electrocautery. 137
■ Argon plasma coagulation. 137, 138
■ Endobronchial stent placement. 139
■ Topical hemostatic agents: Cold saline, epinephrine, vasopressin, thrombin, and oxidized regenerated cellulose have been used to control bleeding. 140 - 142
• Arteriography and embolization should be performed early in massive or recurrent hemoptysis. î Successful embolization in >85% of cases can be achieved with careful localization. 133, 143
î Embolization is particularly useful in cystic fibrosis (CF) patients. 144, 145
î Treatment failure is usually because of inadequate or incomplete source vessel identification. Postembolization arteriography may identify additional systemic culprit vessels, most commonly from the intercostal and phrenic arteries. 146
î Rebleeding is common in embolized patients, occurring in up to 20% of cases over 1 year. Rebleeding appears to be more common in patients with sarcoidosis, malignancy, and aspergilloma. 143, 147, 148
o Risks include bronchial or partial pulmonary infarction and, rarely, ischemic myelopathy because of inadvertent embolization of a spinal artery.
Medications
Systemic procoagulants: These are used only in unstable massive hemoptysis as a temporizing measure. Alternatively, they may be required when conventional bronchoscopic, interventional, or surgical therapies are contraindicated and/or unavailable. Examples are administration of factor VII, vasopressin, and aminocaproic acid.
Surgical Management
Emergent surgery has high morbidity and mortality compared with elective surgery following patient stabilization. 119
• Lobectomy or pneumonectomy offers definitive cure.
î Indications: Persistent focal/unilateral massive hemoptysis despite other therapy. It is particularly useful for stable patients with hemoptysis due to cavitary lung disease, localized bronchogenic carcinoma, AVM, or traumatic injuries. 149
î Contraindications: Poor pulmonary reserve, advanced malignancy, active TB, diffuse lung disease, or diffuse alveolar hemorrhage.
Referral/Consultation
• Pulmonary (interventional for massive hemoptysis, if available)
• Thoracic surgery
• Interventional radiology
Outcome/Prognosis
Mortality depends on etiology and volume of hemoptysis. 119, 150, 151
• Mortality may be as high as 80% in cases of massive hemoptysis because of malignancy.
• Mortality tends to be regulator gene (CFTR), which results in multisystem exocrine organ dysfunction.
Epidemiology
• In the US, >30,000 people are affected by CF, and about 1000 new cases are diagnosed every year. 152, 153
• CF is the most common life-shortening genetic disease in Caucasians; however, the diagnosis should be considered in patients of diverse ethnic backgrounds as well.
• The prognosis of CF has continuously improved, and today >50% of patients with CF in the US are aged ≥18 years.
Etiology
• CF is caused by mutations in the CFTR gene, a cyclic adenosine monophosphate-regulated chloride channel, which normally maintains hydration of exocrine organ secretions.
• Abnormal CFTR function causes decreased chloride secretion and increased sodium absorption on the surface of epithelial cells, which can result in thickened secretions in the airways, sinuses, pancreatic ducts, biliary tree, intestines, and reproductive tract.
• CFTR mutations are categorized into five classes: (1) defective synthesis, (2) defective processing and maturation, (3) defective regulation, (4) defective conductance, and (5) reduced function/synthe sis.
• The most common mutation is F508del, a class II mutation resulting from the deletion of DNA coding for phenylalanine (F) amino acid at position 508. The majority of the resultant misfolded protein is destroyed intracellularly and does not reach the cell surface. More than 85% of patients in the US with CF have at least one copy of this mutation. 153
• To date, >2000 other potentially causative mutations in the CFTR gene have been identified. 153
Pathophysiology
• The primary pulmonary manifestations of CF are related to the malfunction of chloride transport across the airway epithelium, resulting in diminished airway surface liquid and impaired mucociliary clearance.
• Poor mucociliary clearance, infection, inflammation, and chronic airway obstruction often result in bronchiectasis, chronic infection, respiratory failure, and premature death.
• Similarly, thickened secretions in the pancreatic and biliary ducts lead to maldigestion, malabsorption, and, occasionally, liver disease and diabetes. 154
DIAGNOSIS
• Today, children with CF are typically diagnosed via newborn screening or during childhood, but there is increasing recognition of milder variants that may not present until later in life.
• In 2018, 62% of new diagnoses were the result of newborn screening. 153 Newborn screening is now routinely performed throughout the US.
• A diagnosis of CF is made when there are: 155
î Compatible clinical features of CF or
î A positive family history of CF or
î A positive newborn screening test and
î Elevated (>60 mmol/L) sweat chloride or î Intermediate (30-59 mmol/L) sweat chloride and
■ Presence of two disease-causing mutations in CFTR or
■ Abnormal CFTR functional assay
• A diagnosis of CF-related metabolic syndrome is made when there is a positive newborn screening test, and an intermediate sweat chloride level without two causative mutations, or a negative (2000 putative CF mutations.
î Two recessive mutations on separate alleles must be present to cause CF.
î Commercially available CF screens identify >90% of the abnormal genes in a Caucasian Northern European population, although they test for only a minority of the known CF genes. Full gene sequencing is commercially available, but interpretation may be complex. Information about specific
mutations and reported clinical phenotype may be found at http://www.cftr2.org/.
Laboratoriesand testing
• CXRs often demonstrate hyperinflation with upper lobe-predominant cystic lung disease, bronchiectasis, and mucus plugging.
• High-resolution CT scans may be helpful in evaluating patients with early or mild disease by detecting early airway changes.
• PFTs often demonstrate expiratory airflow obstruction with increased residual volume (air trapping) and total lung capacity (hyperinflation). Impairment of alveolar gas exchange may be present later in the course of disease.
• Sputum cultures typically identify multiple organisms including Staphylococcus aureus, nontypeable Haemophilus influenzae, Pseudomonas aeruginosa, Stenotrophomonas maltophilia, and Burkholderia cepacia complex. Isolation of mucoid variants of P. aeruginosa from the respiratory tract occurs frequently. Use of special culture media for fastidious organisms is recommended.
• Nontuberculous mycobacteria (NTM) are also frequently isolated from the airways of persons with CF and may be pathogenic.
TREATMENT
• CF therapy aims to improve quality of life, decrease the number of exacerbations and hospitalizations, reduce the rate of decline in lung function, and decrease mortality.
• A comprehensive program provided at an accredited CF care center is recommended.
• Treatment burden can be a significant barrier to proper adherence. The median number of minutes to complete daily therapies is over 90 min/d.
Chronic Therapies
pulmonary therapy
• Primarily focused on clearing pulmonary secretions and controlling infection.
• Inhaled bronchodilators: β-Adrenergic agonists (such as albuterol, salmeterol, or formoterol). Recommended in all CF patients. Used to treat the reversible component of airflow obstruction and facilitate mucus clearance.
• Recombinant human DNase (dornase alpha, Pulmozyme): Digests extracellular DNA, decreasing the viscoelasticity of the sputum. Improves pulmonary function and decreases the incidence of respiratory tract infections that require parenteral antibiotics. 159
• Hypertonic saline (4 mL of inhaled 7% saline): Improves clearance of secretions, results in fewer exacerbations, and improves lung function. 160 Albuterol should be administered prior to reduce bronchospasm.
• Mechanical airway clearance devices (oral oscillating device, high-frequency chest oscillation vests): Used in combination with medical therapy to promote airway clearance. Other alternatives include postural drainage with chest percussion and vibration. Exercise is also an excellent form of airway clearance.
• Immunizations: Pneumovax and Prevnar 13 are recommended for all patients with CF, as is yearly influenza vaccination.
ANTIBIOTICS
• P. aeruginosa is the most prevalent organism in CF patients and is associated with significant morbidity and mortality. Over time, the percentage of patients colonized with P. aeruginosa (and multidrug-resistant Pseudomonas) increases.
• In patients chronically infected with P. aeruginosa, the inhaled aerosolized antibiotics tobramycin (300 mg nebulized twice daily) and aztreonam lysinate (75 mg nebulized 3? daily) can be used by alternating 28 days on with 28 days off. These improve pulmonary function, decrease the density of P. aeruginosa, and decrease the risk of hospitalization. Continuous alternating inhaled antibiotic therapy has become the standard of care for many patients with chronic Pseudomonas infection and pulmonary impairment.
ANTI-INFLAMMATORY THERAPY
• Azithromycin (500 mg oral 3?∕wk) used chronically shows mild improvement in lung function and reduces days in the hospital for treatment of respiratory exacerbations. Patients should be screened for NTM before initiation of macrolide antibiotics because chronic monotherapy can lead to macrolide- resistant NTM.
• Glucocorticoids used in short courses may be helpful to some patients with asthma-like symptoms, but long-term therapy should be avoided to minimize the side effects.
RESTORATION OF CFTR FUNCTION
• Recently, effective modulator therapy has dramatically changed the treatment of CF and changed the disease course for many patients.
• CFTR modulators treat the underlying cause of the disease by correcting protein misfolding, transporting CFTR to the cell surface, and restoring chloride conductance.
• CFTR correctors increase the amount of mature CFTR on the cell surface while potentiators increase the channel-gating activity of CFTR protein.
• The combination of correctors and a potentiator is more effective than either approach alone.
• See Table 10-11 for details regarding the currently Food and Drug Administration-approved CFTR modulators. One should note that the indications for CFTR modulators are constantly changing especially with respect to age cutoffs.
TABLE 10-11
CURRENTLY FDA-APPROVED CFTR MODULATORS
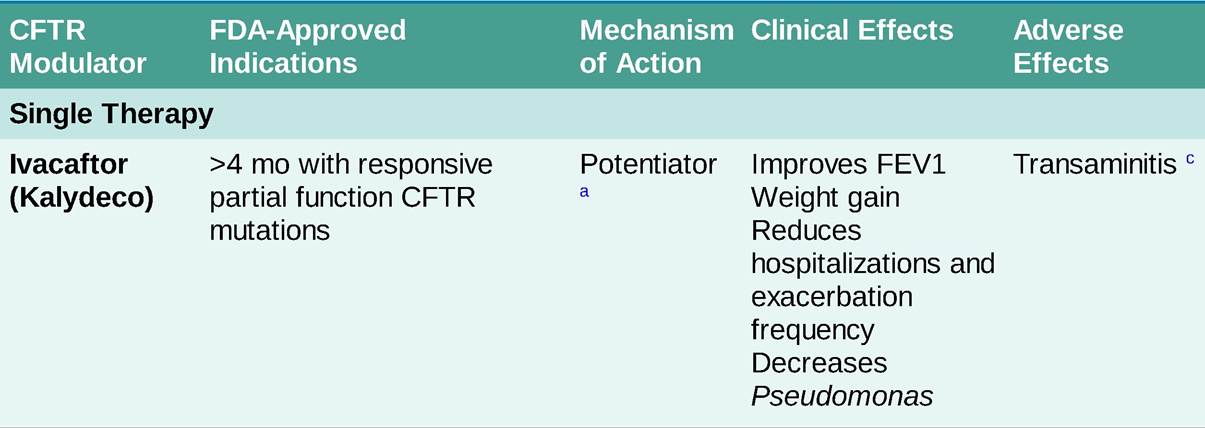
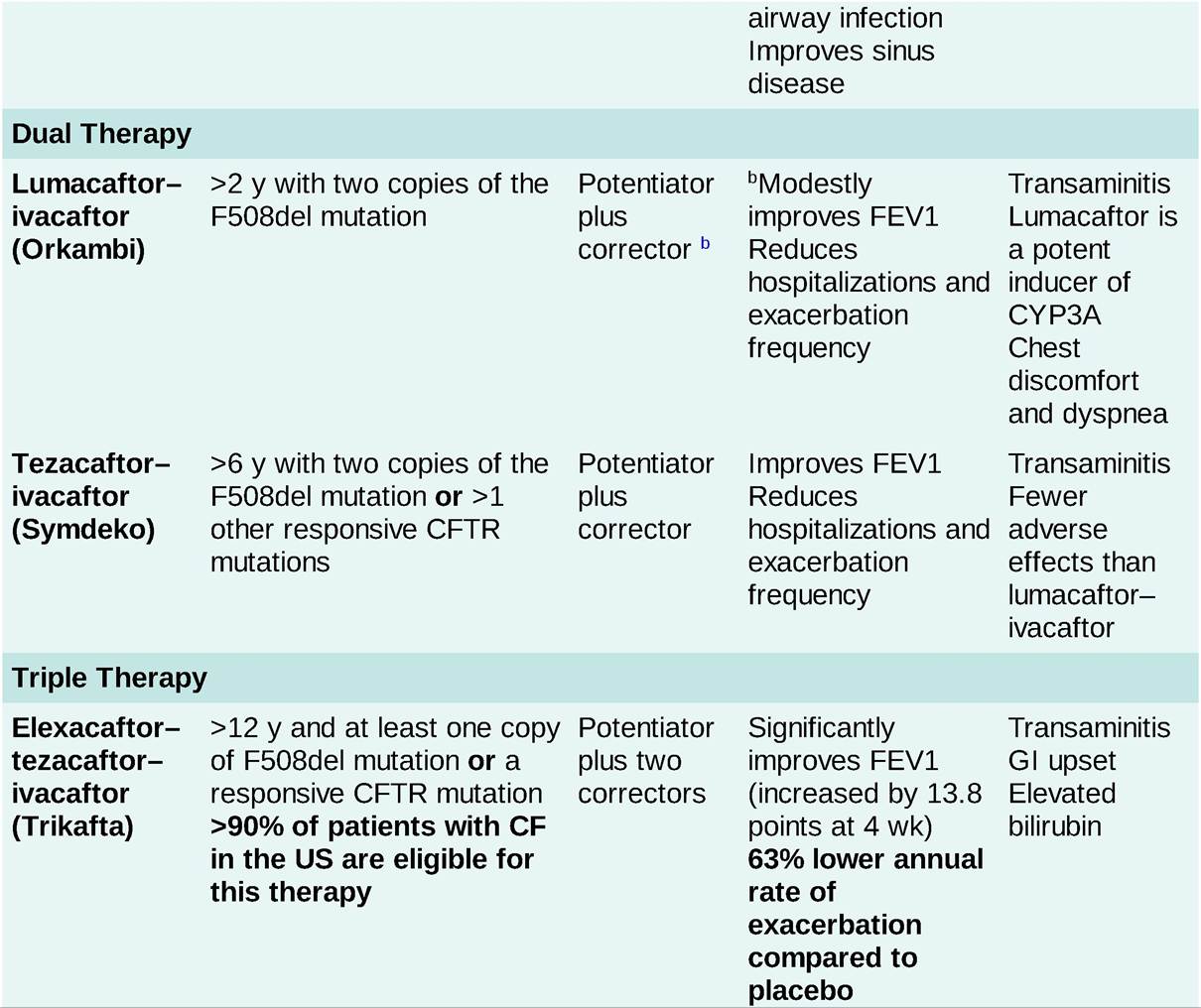
General approach to initiation of therapy: If a patient has a genotype that is eligible for more than one therapy, generally recommended to start maximal therapy available for that age group (triple therapy>double therapy> single therapy). Advance therapy when patient meets age criteria for each combination drug. Dose adjustment in Child-Pugh Class B cirrhosis, avoid in Child-Pugh class C disease. Reduce dose when coadministered with CYP3A inhibitors. See package insert. CF, cystic fibrosis; CFTR, CF transmembrane conductance regulator gene; FDA, Food and Drug Administration; FEV1, forced expiratory volume in the first second.
aPotentiator: Increases CFTR channel open time at the cell surface.
bCorrector: Increases cell surface protein expression by improving the processing and trafficking of CFTR.
cLFTs are recommended prior to initiation of CFTR modulator therapy, every 3 months for the first year, and annually thereafter.
PULMONARY REHABILITATION
• Pulmonary rehabilitation may improve functional status and promote clearance of airway secretions.
oxygen Therapyand noninvasive ventilation
• Oxygen therapy may be indicated based on standard recommendations for the treatment of COPD. Rest and exercise oxygen assessments should be performed as indicated.
• Oxygen may be indicated for patients with a resting PaO2 ≤ 55 mm Hg or SpO2 ≤ 88% at rest or PaO2 ≤ 59 mm Hg or SpO2 ≤ 89% with certain comorbidities (right heart failure, cor pulmonale, or erythrocytosis).
• Nocturnal noninvasive ventilation may be indicated for patients with a daytime resting PCO2 > 50 mm Hg or a nocturnal oxygen saturation saline washes.
• Patients whose symptoms cannot be controlled with medical management may benefit from functional endoscopic sinus surgery and nasal polypectomy.
Mental health
• Depression and anxiety are common among patients and caregivers of CF patients and both patients and caregivers should be screened on a regular basis.
• Psychological symptoms are associated with worse adherence, heath-related quality of life, decreased lung function, and lower BMI.
Lifestyle considerations
• When patients with CF have close contact with another individual with CF, there is a risk of aquiring relevant bacterial infections (cross-infection). Nonetheless, robust peer support groups and virtual events exist and are encouraged.
• People with CF should avoid irritating inhaled fumes, dusts, or chemicals, including second-hand smoke.
• A high-calorie diet with vitamin supplementation is typically recommended.
• CF patients should maintain as much activity as possible.
• Although fertility may be decreased in women with CF secondary to thickened cervical mucus, many women with CF have tolerated pregnancy as well. Ideally, pregnancies should be planned to optimize patient status and coordinate care with obstetrics. CF genetic screening should be offered to partners of patients with CF.
Treatment of Acute Exacerbations
• Common CF exacerbation symptoms include increased cough, change in sputum, increased shortness of breath, fevers, weight loss, or reduction in lung function on spirometry.
• When in a healthcare setting, all personnel should implement contact precautions. Of note, patients with previous isolation of B. cepacia complex should be cared for in a separate area than those without this species.
• Antibiotics are the main treatment for exacerbations.
î Typically, clinicians select antibiotics to which the pathogens are susceptible. However in chronic CF airway infection, it may not be possible to select antibiotics in which all identified pathogens are susceptible.
î P. aeruginosa is the most frequent pulmonary pathogen. The standard approach has been to use two antipseudomonal drugs to enhance activity. A combination of an antipseudomonal β-lactam and an aminoglycoside is typically recommended during acute exacerbations. 161 Of note, prior studies have demonstrated that there is no correlation between in vitro susceptibility testing and clinical response to a particular antibiotic.
î The duration of antibiotic therapy is dictated by the clinical response. At least 14 days of antibiotics are typically needed to treat an exacerbation.
î Patients with CF have atypical pharmacokinetics and often require higher drug doses at more frequent intervals during an acute exacerbation.
î Home IV antibiotic therapy is common, but hospitalization may allow better access to comprehensive therapy and diagnostic testing. Oral antibiotics are recommended only for mild exacerbations. The Cystic Fibrosis Foundation (CFF) recommends against the delivery of home antibiotics unless resources and support are equivalent to hospital setting.
• There is insufficient evidence to recommend routine use of steroids in treatment of acute exacerbations.
• Airway clearance should be intensified during an exacerbation.
• Chronic therapies such as bronchodilators, Pulmozyme (dornase), hypertonic saline, pancreatic enzymes, and CFTR modulators should be continued during a hospitalization.
• Other complications that may require hospitalization include:
î Hemoptysis: Basic treatment involves correction of coagulation factors, withholding chest physiotherapy, stopping inhaled antibiotics, and initiation of IV antibiotics. Refractory cases may require bronchial artery embolization.
î Pneumothorax: Unless small pneumothoraces are treated with chest tube placement. Surgical pleurodesis should be considered in cases of recurrent pneumothorax. In general, airway clearance measures that utilize positive pressure should be withheld in cases of a large pneumothorax, as should noninvasive ventilation.
Lung Transplantation
• CF is the third most common indication for lung transplantation worldwide.
• The CF Foundation guidelines recommend lung transplant referral for any patient with CF with:
î an FEV1 from lung cancer compared to screening with CXR. 164
DIAGNOSIS
• Diagnosis of the SPN is made radiographically, usually via CXR or CT scan.
• Most frequently, the nodule is noted incidentally on a study performed for other reasons (e.g., chronic cough, chest pain, shortness of breath).
Clinical Presentation
• The majority of SPNs are diagnosed incidentally by radiographic tests done for other reasons, so there may not be overt symptoms.
• There are instances when a nodule may precipitate cough, chest pain, hemoptysis, or sputum production depending on the etiology and location of the SPN.
HISTORY
• Ask typical screening questions for malignancy including weight loss and night sweats.
• Hemoptysis may indicate malignancy but may also prompt investigations for ANCA-associated
vasculitis, TB, and hereditary hemorrhagic telangiectasia (HHT).
• Ask about arthritis and arthralgias for possible undiagnosed CTD or sarcoidosis.
• Take an exposure history including recent travel history related to endemic mycoses (histoplasmosis, coccidioidomycosis, etc.) as well as possible TB exposures.
• A history of previous malignancies increases the risk of metastatic disease of the lung.
• Patients who are immunosuppressed from HIV, organ transplant, or chronic steroids have increased risk of infectious causes.
• Smoking is linked to 85% of lung cancers. A patient's risk of lung cancer decreases significantly 5 years after smoking cessation, but never truly returns to baseline.
• An occupational history is important including possible exposure to asbestosis (associated with not only mesothelioma but also non-small-cell lung cancer), silica, beryllium, radon, and ionizing radiation, among others.
PHYSICAL EXAMINATION
• Although there are no specific physical examination findings related to SPNs, evidence for underlying etiologies might be discovered with a thorough examination.
• Note that signs of weight loss or cachexia are suggestive of malignancy.
• Do a thorough lymph node examination. A cervical lymph node might provide an easy diagnostic target to determine the etiology of an SPN.
• Perform a breast examination in women and testicular examination in young men.
• A careful skin examination may reveal telangiectasias, erythema nodosum, rheumatoid nodules, or other findings that might suggest a cause.
Risk Stratification
• The first step in managing an SPN is to stratify the patient in terms of malignancy risk: low-, intermediate-, or high-risk categories (Table 10-12). Risk stratification can be accomplished either qualitatively via clinical judgment or quantitatively using validated risk assessment tools. These approaches appear to be complementary. 165
| ASSESSMENT OF | THE PROBABILITY OF MALIGNANCY | ||||
| Assessment Criteria | Low (65%) | ||||
| Clinical factors alone (determined by clinical judgment and/or use of validated model) | Young, less smoking, no prior cancer, smaller nodule size, regular margins, and/or non-upper lobe location | Mixture of low and high- probability features | Older, heavy smoking, prior cancer, larger size, irregular spiculated margins, and/or upper-lobe location | ||
| FDG-PET scan results | Low-moderate clinical probability and low FGD-PET activity | Weak or moderate FDG-PET scan activity | Intensely hypermetabolic nodule | ||
| Nonsurgical biopsy results (bronchoscopy or TTNA) | Specific benign diagnosis Nondiagnostic Suspicious for malignancy | ||||
| CT scan surveillance | Resolution or near-complete Nonapplicable Clear evidence of resolution, progressive or growth persistent decrease in size, or no growth over ≥2 y (solid nodule) or ≥3-5 y (subsolid nodule) | ||||
FDG, 18-fluorodeoxyglucose; PET, positron emission tomography; TTNA, transthoracic needle aspiration.
Reprinted from Gould MK, Donington J, Lynch WR, et al. Evaluation of individuals with pulmonary nodules: when is it lung cancer? Diagnosis and management of lung cancer, 3rd ed—American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143(5):e93s-e120s. Copyright © 2013 The American College of Chest Physicians. With permission.
• Once the risk of malignancy has been established, further management can proceed, as outlined in Figure 10-6.
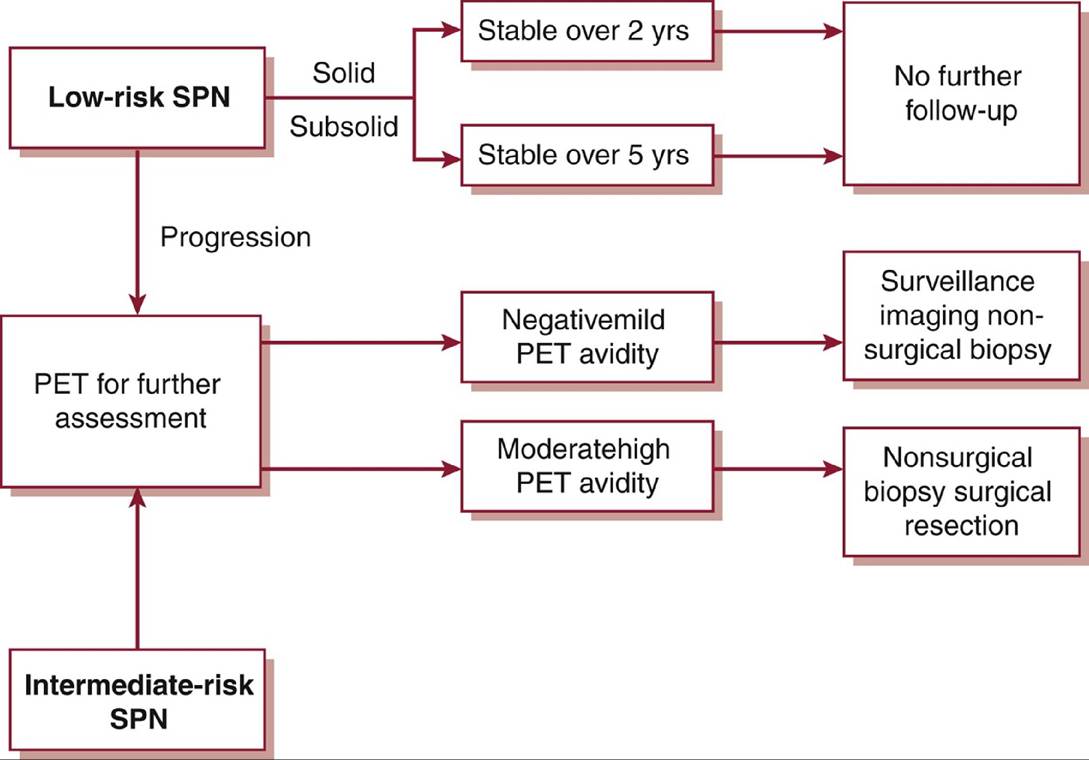
Figure 10-6 Diagnostic and therapeutic management of low- and intermediate-risk pulmonary nodules.PET, positron emission tomography; SPN, solitary pulmonary nodule; yrs, years.
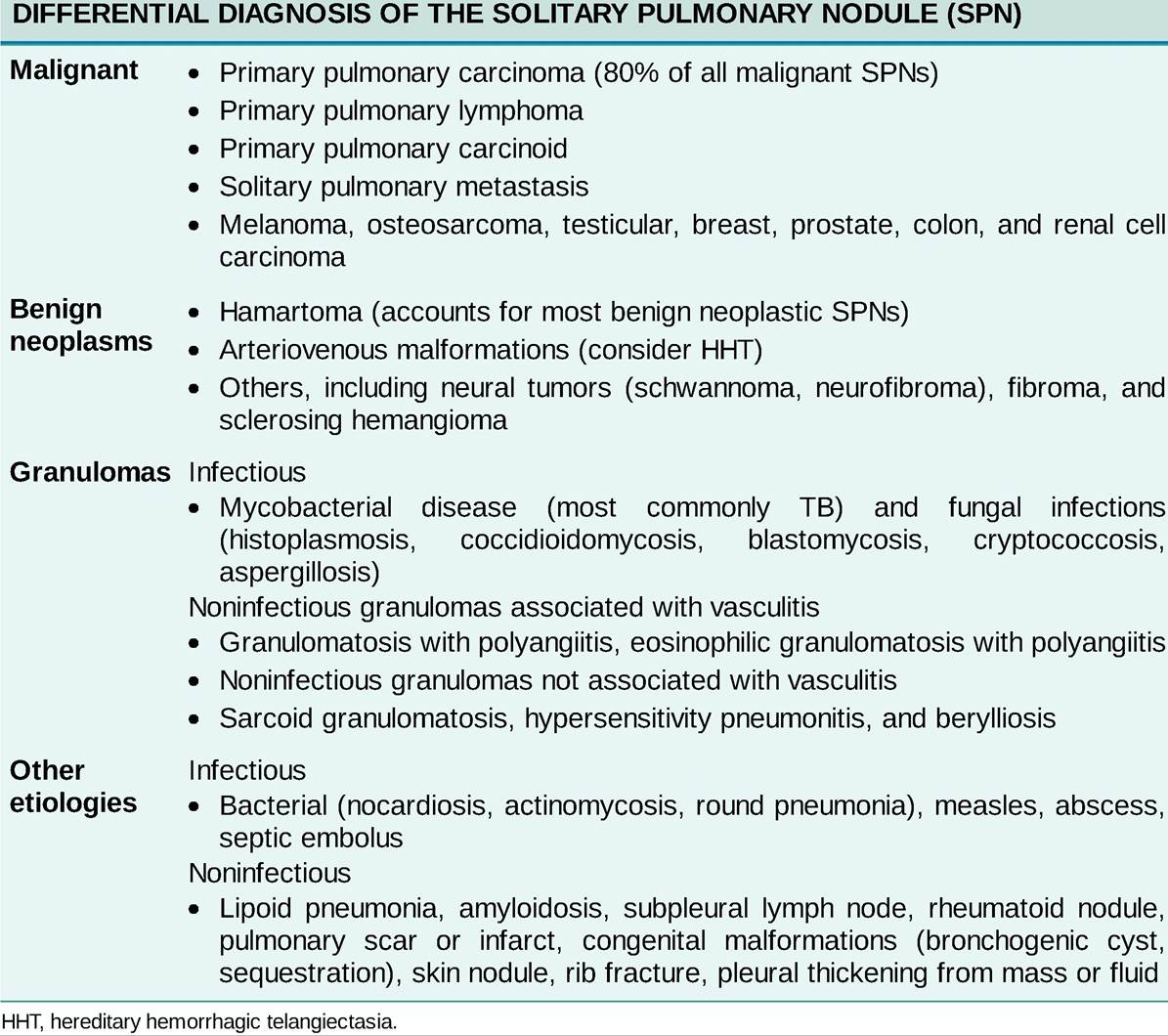
Differential Diagnosis
Pulmonary nodules are divided primarily into malignant or benign etiologies, with benign processes further divided into infectious or noninfectious causes (Table 10-13).
TABLE 10-13
Diagnostic Testing
LABORATORIES
• Routine laboratory testing is seldom helpful unless the history and physical examination strongly suggest an etiology.
• If CTDs or vasculitides are suspected, perform appropriate testing.
• Hyponatremia may suggest syndrome of inappropriate antidiuretic hormone associated with primary lung cancer, as well as other pulmonary processes.
• Hypercalcemia might suggest lung cancer as well as sarcoidosis.
• Anemia may indicate chronic pulmonary hemorrhage (e.g., HHT) or a chronic inflammatory disease.
• Microbiologic studies, particularly sputum culture, may aid in the diagnosis of an infectious SPN.
• Sputum cytology has limited use because yield is low for peripherally located, small lesions.
IMAGING
The mainstay of diagnostic evaluation of an SPN is via radiographic studies, primarily CXR, chest CT, and positron emission tomography (PET) scan.
• CXR:
î A previous CXR is an important tool in the initial evaluation of an SPN.
î If an SPN has been present and unchanged on CXR for >2 years, then further evaluation may not be warranted. Subsolid lesions should be followed for longer periods because the volume-doubling time is extended in certain types of non-small-cell lung cancers.
î If an SPN appears on a new radiograph in sensitivity of 80%-100% and specificity of 79%-100% for detecting malignancy.
î False negatives can occur in bronchoalveolar carcinoma, carcinoid, and mucinous neoplasms, whereas false positives are common in nonmalignant “inflammatory” conditions (infectious and autoimmune processes).
î A higher incidence of both false-positive and false-negative results occurs in nodules effusion occur annually in the US.
• It is estimated that malignant pleural effusion affects about 150,000 people a year in the US. Congestive heart failure and parapneumonic effusion are the predominant etiologies of pleural effusion in the US. 174
• Incidence of pneumothorax varies widely by gender, country, and race.
Etiology
• Pleural effusions have a variety of causes and are listed below (Table 10-14).
î Empyema is generally caused by extension of an infection of the lung or surrounding tissue.
■ Common microbial pathogens are S. aureus, Streptococcus species, H. influenza, and oral anaerobes.
■ Empyemas are frequently polymicrobial in cases where aspiration is suspected, commonly because of oral flora.
° The three major grouped causes of chylothorax are malignancy (50% of cases), 172 ’ 178 trauma (25%), and idiopathic (15%). 179 Other rare causes such as LAM 180 and trauma to thoracic duct account for 10%.
■ Seventy-five percent of chylous effusions associated with malignancy are due to lymphoma- related obstruction of pleural lymphatics preventing reabsorption of pleural fluid. 172
■ Trauma as a causative factor of chylothorax includes any cardiothoracic surgical procedure. It may take 1-2 weeks postsurgery for the chylothorax to become apparent.
■ In a number of cases, chylothorax results from transdiaphragmatic leakage of chylous ascites. 172 Causes of chylous ascites include nephrotic syndrome, hypothyroidism, and cirrhosis of the liver. 172
î Hemothorax may result from trauma or an iatrogenic etiology and are rarely spontaneous. 171
î Other causes of pleural effusion include heart failure, anasarca, and pulmonary embolism.
• Secondary pneumothorax is often seen in chronic obstructive pulmonary disease, AIDS, CF, TB, P. jirovecii pneumonia, sarcoidosis, pulmonary fibrosis, asthma, Marfan disease, LAM, PLCH, trauma, or any cavitary or cystic lung disease.
TABLE 10-14
CAUSES OF PLEURAL EFFUSION
• Exudates
î Infections
■ Bacteria
■ TB
■ Fungi
■ Parasites
■ Viruses
■ Mycoplasma
î Neoplasms
■ Metastatic carcinoma
■ Lymphoma
■ Leukemia
■ Mesothelioma
■ Bronchogenic carcinoma
■ Chest wall tumors
î Intra-abdominal disease/gastrointestinal
■ Abdominal surgery
■ Pancreatitis
■ Meigs syndrome
■ Intrahepatic abscess
■ Incarcerated diaphragmatic hernia
■ Subdiaphragmatic abscess
■ Esophageal rupture
■ Endoscopic variceal sclerotherapy
■ Hepatitis
î Collagen vascular diseases/vasculitis
■ Systemic lupus erythematosus
■ Rheumatoid arthritis
■ Drug-induced lupus
■ Sjogren syndrome
■ Granulomatosis with polyangiitis
■ Eosinophilic granulomatosis with polyangiitis
■ Immunoblastic lymphadenopathy
î Drug-induced pleural disease
■ Nitrofurantoin
■ Dantrolene
■ Methysergide
■ Bromocriptine
■ Procarbazine
■ Amiodarone
î Pulmonary infarction secondary to thromboembolic disease
î Miscellaneous
■ Dressler syndrome (postcardiac injury)
■ Sarcoidosis
■ Yellow nail syndrome
■ Trapped lung
■ Radiation therapy
■ Electrical burns
■ Iatrogenic injury
■ Ovarian hyperstimulation syndrome
■ Chronic atelectasis
■ Asbestos exposure
■ Familial Mediterranean fever
■ Urinoma
î Idiopathic
î Lipid laden
■ Chylous
■ Pseudochylous
î Trauma
• Transudates
î Increased hydrostatic pressure
■ Congestive heart failure
■ Constrictive pericarditis
■ Superior vena caval obstruction
î Decreased oncotic pressure
■ Cirrhosis
■ Nephrotic syndrome
■ Hypoalbuminemia
■ Peritoneal dialysis
î Miscellaneous
■ Acute atelectasis
■ Subclavian catheter misplacement
■ Myxedema
■ Idiopathic
Pathophysiology
• Pleural effusions can be categorized as transudates or exudates.
î Transudates result primarily from passive fluid shifts that occur as a result of changes in the hydrostatic and/or oncotic pressures of the circulation. 181
î Exudates are indicative of an active pleural process such as inflammation of the pleura or underlying
lung tissue.181
î There are numerous causes of both transudates and exudates (Table 10-14). 181
• Primary spontaneous pneumothorax is thought to result from rupture of subpleural apical blebs, with no obvious preceding cause. 182
• Secondary pneumothorax results from rupture of pathologic lung architecture such as emphysematous bullae, cysts, or cavity formation. 182
Risk Factors
• Risk factors for pleural effusion reflect those of the underlying causative disease.
• Primary spontaneous pneumothoraces are more common in tall, thin males and recur 50% of the time.
• Marfan disease is associated with a primary spontaneous pneumothorax. 182
DIAGNOSIS
• Diagnosis of a pleural disease is based on history, physical examination, and radiographic imaging, which includes chest radiography, CT scan, and chest ultrasound. 183
• Differentiation into a specific pathologic entity is based on history, imaging, and laboratory analysis (chemistry, microbiology, and cytology) of the pleural fluid if present.
Clinical Presentation
• Symptom onset may be chronic, subacute, or acute depending on the rapidity with which the pleural pathology developed (amount of gas or excess pleural fluid).
• If the effusion is very large in nature, it may cause a mass effect progressing to a tension physiology with hemodynamic instability from cardiac tamponade resulting in a life-threatening hypotension.
HISTORY
• Dyspnea is the primary symptom of pleural disease, and pain may also be present.
î Pain is generally pleuritic in nature.
î Referred pain to the abdomen and ipsilateral shoulder are possible.
• Other symptoms depend on the specific etiology of the pleural disease:
î Empyema may be associated with fevers, chills, and malaise.
î Hemothorax may present with signs and symptoms of anemia such as acute or subacute dyspnea. 171 î Chylothorax contains large amounts of fat, protein, and lymphocytes, which accounts for nutritional and immunologic deficiencies observed when they are chronic in nature.
PHYSICAL EXAMINATION
• Decreased expansion on inspiration, dullness to percussion, and decreased or absent breath sounds on auscultation are all consistent with a pleural effusion.
• The examination finding that correlates best with presence of pleural effusion is asymmetric chest wall expansion.
• Asymmetric chest wall appearance, decreased breath sounds, decreased tactile fremitus, and hyperresonance to percussion may be consistent with a large pneumothorax.
• Hypotension may be the presenting sign if there is a mass effect from a large pleural effusion or tension pneumothorax.
Diagnostic Criteria
There are no clinical criteria to definitively diagnose a pleural effusion or pneumothorax and radiographic imaging is generally needed.
Differential Diagnosis
The differential diagnosis for pleural effusion or pneumothorax includes other causes of dyspnea such as pulmonary edema, pneumonia, compressive or resorptive atelectasis, thromboembolic disease, ILD, or central airway obstruction because of benign or malignant disease.
Diagnostic Testing
Radiographic imaging and laboratory testing of pleural fluid are the two most useful diagnostic modalities for diagnosing pleural disease.
LABORATORIES
• Categorization of pleural fluid as transudative or exudative assists with diagnosis and therapeutic management. 184
î Light's criteria compare levels of protein and lactate dehydrogenase in the effusion with those in the patient's serum to determine whether inflammation or fluid shift is responsible for the effusion. 185
■ If one of the three Light's criteria is met, the effusion is defined as an exudate (Table 10-15). 184, 185
o Heffner's criteria have similar sensitivity for identifying exudative pleural effusions when compared with Light's criteria and do not require concomitant serum values for comparison (Table 10-15). 186
• Other useful studies to differentiate the type of pleural effusion include pH, glucose, cell count, Gram stain, culture, and triglycerides. Hematocrit should be sent if hemothorax is suspected. 184
î Empyema can be diagnosed by a positive Gram stain or culture.
■ Empyema is also characterized by a low pH and low glucose.
î Hemothorax is defined by a pleural hematocrit/serum hematocrit of >0.5.
î Chylothorax is diagnosed by pleural triglycerides >110 mg/dL or by the presence of chylomicrons in the pleural fluid. 172
■ If chylothorax is suspected and triglycerides are 50-110 mg/dL, a lipoprotein electrophoresis can confirm the presence of chylomicrons. 172
° Malignant pleural effusion is diagnosed by a positive fluid cytology, and though highly specific, it is not sensitive. The sensitivity of diagnosis of a malignant pleural effusion increases slightly with subsequent thoracentesis up to three times and with increasing amount of pleural fluid. 187
î See Table 10-16 for other pleural fluid laboratory values associated with specific pleural effusions.
TABLE 10-15
CRITERIA FOR DEFINING AN EFFUSION
• Light's criteria
î Pleural fluid protein to serum protein ratio of >0.5
î Pleural fluid lactate dehydrogenase (LDH) to serum LDH ratio of >0.6
î Pleural fluid LDH >2/3 serum upper limit of normal
• Heffner criteria
î Pleural fluid protein >2.9 g/dL
î Pleural fluid cholesterol >45 mg/dL
î Pleural fluid LDH > 45% of upper limits of normal serum value
Adapted from Light RW. Clinical manifestations and useful tests. In: Light RW, ed. Pleural Diseases. 4th ed. Lippincott Williams and Wilkins; 2001:42-86; Heffner JE, Brown LK, Barbieri CA. Diagnostic value of tests that discriminate between exudative and transudative pleural effusions. Chest. 1997;111:970-980.
TABLE 10-16
HELPFUL FEATURES OF EXUDATIVE PLEURAL EFFUSIONS
• Malignancy
î Fluid cytology positive for malignant cells
• TB
î Pleural fluid is lymphocytic
î Positive acid-fast bacilli stain is very rare
î Pleural fluid is sanguineous
• Connective tissue disease
î Pleural fluid usually lymphocytic and will often have antinuclear antibody positivity
• Pancreatitis
î Increased amylase
• Infection
î Gram stain and culture often reveal specific infection
î Empyema is accompanied by very low glucose and pH and a markedly elevated lactate dehydrogenase
• Drug related
î Eosinophilic fluid
• Chylothorax
î Milky fluid, triglyceride level >110 mg/dL
• Hemothorax
î Sanguineous fluid
î Hematocrit of pleural fluid is >50% of peripheral blood
IMAGING
• Chest radiograph is generally the first imaging study obtained when a patient presents with a suspected pleural effusion or pneumothorax. 188
î On a posteroanterior chest film, blunting of the costophrenic angle or blurring of the diaphragmatic margin suggests the presence of a pleural effusion.
■ Generally, 200-500 mL of fluid is needed to generate this finding. 189
î A lateral decubitus film of the affected side can reveal an effusion of approximately 100 mL and allows for assessment of a free-flowing versus loculated effusion. 188, 189
• CT is more sensitive than routine chest radiography and can detect the presence of even a very small amount of fluid or air in the pleural space as well as the presence of Ioculations in the pleural fluid. 188
• Ultrasound is a modality that is increasingly being used to image the pleural space.
î Ultrasound can detect fluid or air and provides qualitative information regarding pleural fluid and detects small amounts of fluid as well as the presence of septations in the pleural space.
■ Ultrasound findings such as fluid echogenicity and the presence of septations indicate a complex loculated effusion potentially changing management and predicting clinical outcome.
■ Ultrasound guidance is often used to direct treatments such as drainage of fluid or chest tube insertion.
DIAGNOSTIC PROCEDURES
• Thoracentesis should be performed for diagnosis in cases of pleural effusion of unknown etiology. Subsequent thoracentesis increase the diagnostic yield depending on the etiology. 187
• Therapeutic thoracentesis can lead to symptom relief and is indicated for dyspnea.
î Thoracentesis should generally be performed after ultrasound localization of pleural fluid to decrease risk of complications such as pneumothorax.
î CXR should be performed after the procedure to rule out a complicating pneumothorax.
î Hemothorax is a rare complication.
TREATMENT
• Generally, treatment of a pleural effusion depends on the etiology.
° Transudative pleural effusions are most appropriately managed by treating the underlying cause.
■ Symptomatic treatment may involve drainage of the effusion if the presenting symptom is dyspnea or acute respiratory failure.
î Exudative pleural effusions should be evaluated for an underlying cause.
■ Treatment may involve drainage of the effusion or even pleurodesis to prevent reaccumulation of fluid.
■ Placement of an indwelling pleural catheter for malignant recurrent pleural effusions or in cases of hepatic hydrothorax refractory to medical therapy may be an option. 190
• Treatment of pneumothorax generally involves draining the air from the pleural space by insertion of a chest tube.
• Pleurodesis should be considered after the first episode of secondary spontaneous pneumothorax because rates of recurrence are high. 175
Medications
• Pleural effusions can sometimes be treated with medications depending on the cause.
• Parapneumonic effusions and empyema are treated with antibiotics in conjunction with fluid drainage. 174
• Transudative pleural effusions can sometimes be treated effectively with diuretics in disease states such as congestive heart failure, anasarca, renal failure, and liver failure.
• There is no medical treatment for pneumothorax.
Nonpharmacologic Therapies
• Pleurodesis involves instillation of a sclerosing agent into the pleural space to cause scarring and restriction of the space itself.
î This is generally performed for recurrent malignant effusion, recurrent pneumothorax once the lung has reexpanded, occasionally for chylothorax, and after the first episode of secondary spontaneous pneumothorax. 175
• When other modalities fail, total parenteral nutrition with complete bowel rest can cause chylothoraces to resolve as oral intake results in chyle formation. 172
î Medium-chain triglyceride diets have been tried, as chyle is derived from long-chain triglycerides in the diet, though this has yielded mixed results. 172
• If a pneumothorax is In cases of persistent pneumothorax secondary to a bronchopleural fistula, fiber-optic bronchoscopy with placement of endobronchial valves causing atelectasis of the distal lung may be an option if the bronchopleural fistula has been localized to one location via balloon catheter occlusion. 191
Surgical Management
• Pleural effusion:
î Chest tube insertion is often indicated for drainage of large pleural effusions.
î Other indications for chest tube insertion include empyema, chylothorax, and hemothorax. 171
î Thoracentesis can be used as a therapeutic modality.
î Malignant pleural effusion:
■ Tunneled pleural catheter is used for recurrent malignant pleural effusion and occasionally hepatic hydrothorax refractory to medical management and diuresis. 190
■ This catheter can be drained at home every other day with attachment to a vacuum-sealed device or gravity collection system.
■ About 30%-50% of patients who have indwelling tunneled pleural catheters in place for malignant pleural effusion may experience auto-pleurodesis, or the cessation of significant additional pleural fluid drainage. In these cases, the indwelling pleural catheters may be removed with a very low likelihood for reaccumulation of pleural fluid on the side where the catheter was placed. 192
î Empyema:
■ In cases where chest tube drainage does not effectively drain an empyema and there is continued evidence of infection, VATS with decortication is often indicated.
■ There is a role for intrapleural use of tissue plasminogen activator and recombinant deoxyribonuclease (DNase) in pleural infections. These result in improved fluid drainage and decreased need for surgical intervention. 193
î Hemothorax:
■ Requires surgical stabilization in 30% of penetrating injuries and 15% of blunt injuries. 194
■ Initial output of >1500 mL of blood or continued chest tube output or >200 mL of blood over 2 hours requires surgical intervention.
■ Clotted blood in the pleural space may require VATS to prevent development of empyema or fibrothorax. 195
î Chylothorax:
■ For persistent chylothorax, surgical interventions include thoracic duct ligation via VATS in conjunction with pleurectomy or pleurodesis. 195
■ Pleuroperitoneal shunting is also occasionally performed, though obviously not in cases in which the pleural disease is secondary to chylous ascites. 194
■ Early surgical intervention for chylothorax should be considered when chest tube output is >1500 mL/d or in a patient with malnourishment or an immunocompromised state. 172
î Pneumothorax:
■ Treated with chest tube insertion if they are large, symptomatic, under tension, recurrent, or bilateral.
? In extreme circumstances where a large pneumothorax is causing cardiovascular collapse, immediate needle decompression is indicated by inserting a needle in the anterior chest above the nipple line in a parasternal location.
■ For recurrent pneumothorax, VATS may be indicated with endoscopic stapling and removal of the bulla or fistula, particularly if there is a bronchopleural fistula. 191
■ Therapeutic success of bronchoscopic management of bronchopleural fistula with endobronchial valves, coils, glue, or sealant has been variable and treatment must be individualized. 191
SPECIAL CONSIDERATIONS
• The etiology of pleural effusions can often be discerned by their appearance.
î A serous effusion is more likely to be transudative, while an exudative effusion is more likely to have other appearances, frequently with a cloudy or serosanguinous appearance.
° If the fluid appears frankly bloody, a hemothorax should be suspected.
î Pus indicates an empyema.
î Milky white and opalescent pleural fluid is indicative of a chylothorax.
• In cases of massive hemothorax requiring surgical intervention, clamping the chest tube may result in tension hemothorax and cardiovascular collapse. 195
• Chylothorax is nonirritating and bacteriostatic, thus secondary infection is extremely rare. 194
Complications
• Disease recurrence.
• Cardiovascular compromise in extreme cases.
• Other complications are disease-specific.
Referral
• Interventional pulmonology may be consulted for the placement of chest tubes, tunneled pleural catheters, or endobronchial valve.
• Surgical consultation may be needed as per the “Surgical Management” section above.