Iron Deficiency Anemia
GENERAL PRINCIPLES
• Iron deficiency is the most common cause of anemia in the ambulatory setting and is usually a chronic microcytic anemia with a low reticulocyte count.
• The most common causes of iron deficiency anemia are blood loss (e.g., menses, GI blood loss), decreased absorption (e.g., achlorhydria, celiac disease, bariatric surgery, Helicobacter pylori infection), and increased iron requirement (e.g., pregnancy).
• It is important to determine the cause of iron deficiency, and in the absence of menstrual bleeding, evaluation of the GI tract should be performed to identify a potential cause including the possibility of an occult malignancy.
DIAGNOSIS
Clinical Presentation
• Patients often present with cold intolerance along with fatigue or malaise that is typically worsened with activity. Pallor is also a common physical finding.
• Pica (consumption of substances of no nutritional value such as ice, starch, or clay) occurs in about 25% of patients with chronic iron deficiency anemia and rarely occurs in other clinical settings.
• Restless leg syndrome is a common but a nonspecific finding in patients with iron deficiency anemia.
Diagnostic Testing
• Peripheral blood smear may show hypochromia (increased central pallor of RBCs), microcytosis, and pencil-shaped cells (elliptocytes). The reticulocyte count is low in iron deficiency anemia.
• Ferritin is the primary storage form for iron in the liver and is a specific marker of an absolute iron deficiency. The reference range is 30-400 ng/mL.
î A ferritin level of lt;10 ng/mL in women or lt;20 ng/mL in men almost always reflects low iron stores. î Ferritin is an acute-phase reactant, so normal levels may be seen in inflammatory states despite low iron stores. A serum ferritin level of gt;200 ng/mL generally excludes an iron deficiency; however, in renal dialysis patients, a functional iron deficiency may be seen with a ferritin up to 500 ng/mL.
• Iron, total iron-binding capacity (TIBC), and transferrin saturation are often used in combination with ferritin to diagnose iron deficiency anemia. Serum iron level alone is an unreliable indicator given its significant fluctuation after a meal.
DIAGNOSTIC PROCEDURES
• A BM biopsy that shows absent staining for iron is the definitive test to diagnose iron deficiency anemia and is helpful when the serum tests do not clearly demonstrate the diagnosis.
• An iron challenge can be performed in the absence of response to oral iron replacement to differentiate poor absorption from other causes (e.g., nonadherence or occult blood loss). After an 8hour fast, a baseline iron is measured immediately followed by oral intake of liquid ferrous sulfate 5 mg/kg given with orange juice or vitamin C-containing beverage. Serum iron is measured again after 90 minutes. Normal iron absorption will result in an increase of serum iron of at least 50 pg/dL and a lower level is indicative of poor absorption.
TREATMENT
• Oral iron therapy. Given in stable patients with mild symptoms. Several different preparations are available (Table 21-1).
î Iron is best absorbed on an empty stomach, and 3-10 mg of elemental iron can be absorbed daily.
TABLE 21-1
ORAL IRON PREPARATIONS
| Preparation | Common Dosing Regimen | Elemental Iron (mg per dose) |
| Ferrous sulfate | 325 mg qd-tid | 65 |
| Ferrous gluconate | 300 mg tid | 36 |
| Ferrous fumarate | 100 mg tid | 33 |
| Iron polysaccharide complex | 150 mg bid | 150 |
| Carbonyl iron | 50 mg bid-tid | 50 |
î Oral iron ingestion may induce a number of GI side effects and as a result, nonadherence is a common problem. These side effects can be decreased by initially administering the drug with meals or every other day, which may be as effective as more frequent dosing.1 Concomitant treatment with a stool softener can also alleviate constipation.
î Ferrous sulfate is the most commonly prescribed formulation. If there are unacceptable side effects, consider using a lower dose or an alternative formulation such as ferrous gluconate or ferrous fumarate, which contains lower amounts of elemental iron.
î In general, patients responding to oral iron therapy should see an increase in reticulocyte count within 1 week of therapy; an increase in Hgb of 2 g/dL every 3 weeks is expected. Treatment should be continued until the total iron deficit is replete.
• Parenteral iron therapy (Table 21-2). There are several formulations of IV iron, and indications for parenteral iron over oral iron include the following:
î Poor absorption (e.g., inflammatory bowel disease, malabsorption).
TABLE 21-2
IV IRON PREPARATIONS
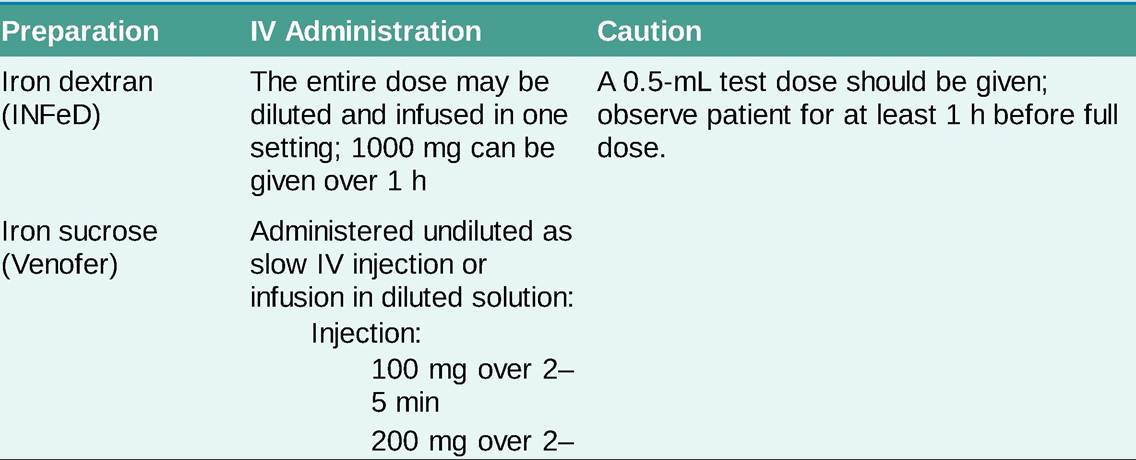
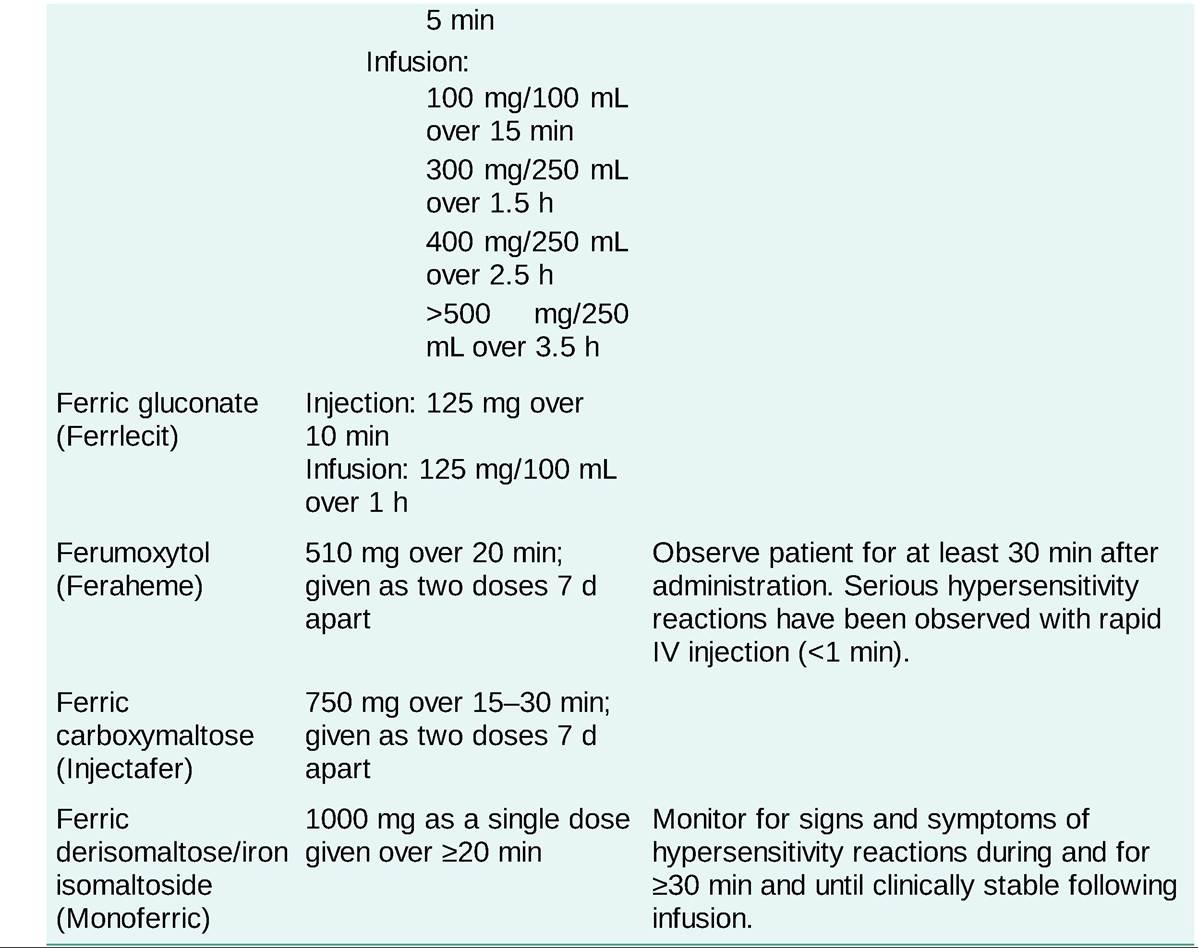
° Very high iron requirements that cannot be met with oral supplementation (e.g., ongoing bleeding). î Intolerance to oral preparations.
î Functional iron deficiency in chronic kidney disease (CKD).
Specific Considerations
• IV iron infusion should not be given in patients with an active infection (i.e., fever) owing to concern for increased adverse reactions such as sepsis.
• The total iron replacement dose may be estimated using the patient's baseline Hgb and body weight with the Ganzoni formula:


given over an hour; however, infusion can be complicated by serious side effects including anaphylaxis.
• Second-generation iron products include ferric gluconate (Ferrlecit) and iron sucrose (Venofer) and can be given at a faster infusion rate than INFeD. Anaphylaxis is rare, and a test dose is not needed; however, a single infusion is typically insufficient to replenish the entire iron deficit, so multiple doses are required.
• Third-generation iron products, including ferumoxytol (Feraheme), ferric carboxymaltose (Injectafer), and ferric derisomaltose (Monoferric), allow for administration of a high dose with a rapid infusion. A rare complication is severe hypotension, which can be related to the rapidity of the injection. Ferric carboxymaltose and ferric derisomaltose can be associated with hypophosphatemia.
• Of note, some IV irons can interfere with MRI results and mimick hemosiderosis on liver MRI. If MRI imaging is needed, it is recommended that a period of at least 1 week be given between the last IV iron sucrose and ferric gluconate infusion and MRI. Ferumoxytol is available as an MRI contrast agent and will transiently show a significant increase in iron stores in the liver, which can be seen for up to 3 months following infusion.