Spondyloarthritis
GENERAL PRINCIPLES
• The Spondyloarthritides (SpAs) are an interrelated group of disorders characterized by one or more of the following features: spondylitis, sacroiliitis, enthesopathy (inflammation at sites of tendon insertion), and asymmetric oligoarthritis.
The majority of the patients present before the age of 45. SpAs have an association with HLA-B27. These diseases are classified by their location (peripheral or axial) and by the subtype.î Ankylosing spondylitis (AS)
î Psoriatic arthritis (PsA)
î Reactive arthritis (ReA)
î Inflammatory bowel disease (IBD) or enteropathic arthritis
° Undifferentiated spondyloarthritis (USpA)
• In clinical practice, SpAs overlap significantly. USpA refers to patients with features of SpA without AS, psoriasis, IBD, or a prodromal infection that could account for ReA. Of the subtypes, AS and PsA are the most prevalent.
DIAGNOSIS
Clinical Presentation
• Shared clinical manifestations include inflammatory back pain, peripheral arthritis, enthesitis, and dactylitis. Extra-articular features of this group of disorders may include inflammatory eye disease, urethritis, and mucocutaneous lesions.
• Inflammatory back pain characteristics include onset at lt;45 years of age, morning stiffness longer than 60 minutes, frequent nocturnal pain, and improvement with exercise. Patients may also describe alternating buttock pain.
• Peripheral inflammatory arthritis is usually asymmetric, commonly involves the lower extremities, and usually affects less than five joints (oligoarthritis).
• Enthesitis refers to the inflammation at the site of tendon or ligament insertion. Common sites include Achilles tendon, plantar fascia, elbow epicondyles, iliac crests, and tibial tuberosities.
• Dactylitis, also known as “sausage digit,” is the result of tenosynovitis of the flexor tendons of the digits and synovitis of the joint spaces.
It can affect fingers and toes.• Uveitis is the most common extra-articular manifestation. It can occur in any of the SpAs but is most commonly associated with AS. Uveitis tends to be anterior and unilateral.
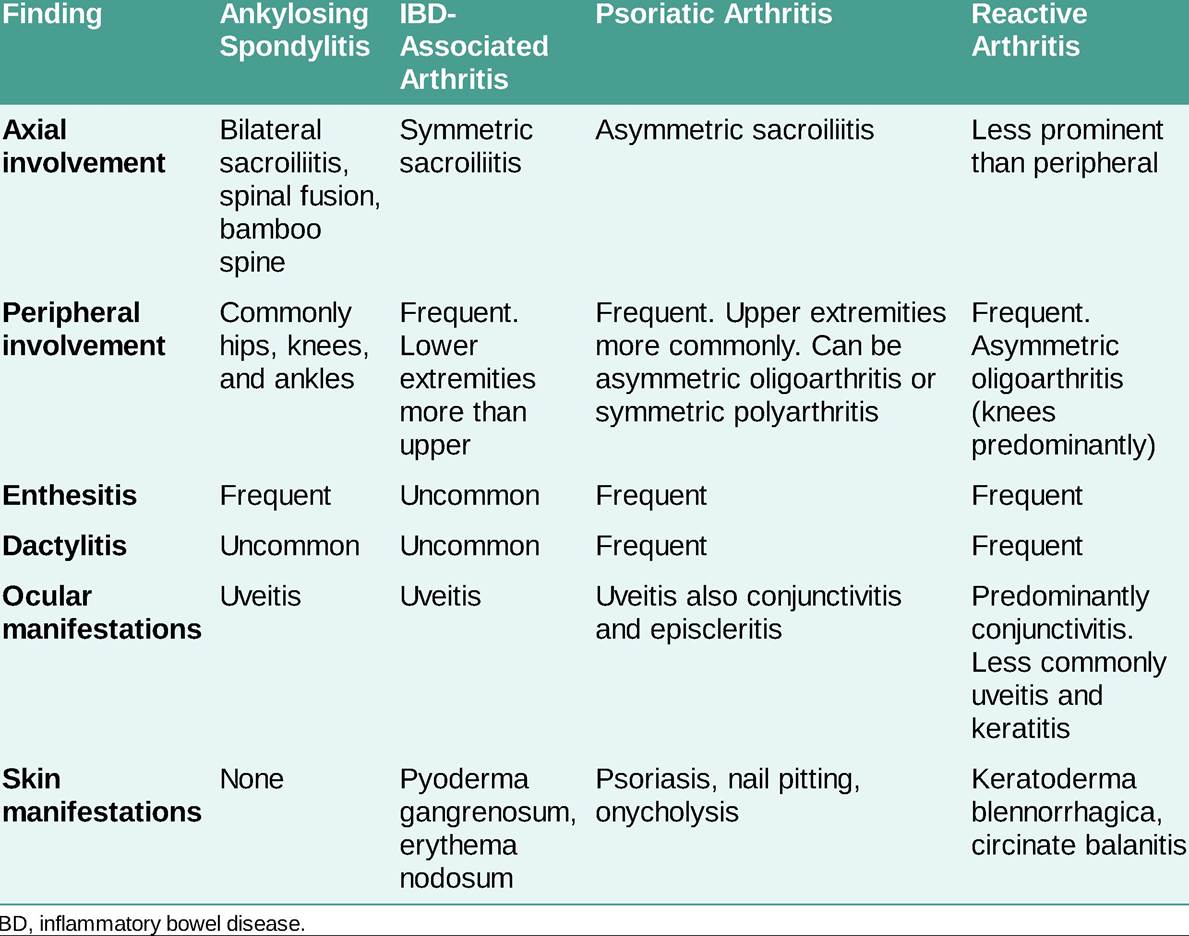
• Uncommon manifestations include oral ulcers, aortitis, aortic regurgitation, pericarditis, conduction defects, immunoglobulin A nephropathy, and amyloidosis (Table 25-4).

PHYSICAL EXAMINATION
A thorough exam should be performed to evaluate for axial and peripheral involvement as well as extra- articular manifestations.
• Axial skeleton evaluation should include spinal forward flexion using modified Schober's test (normal is gt;5 cm), lateral flexion (distance from the middle fingertip to the floor), cervical motion measuring the occiput to wall distance (normal distance is zero), and chest expansion by measuring circumference of the chest in inspiration and expiration (normal gt;2.5 cm).
• Peripheral joints should be evaluated for swelling, erythema, warmth, tenderness at the site of tendon insertion, joint effusions, and dactylitis.
• The skin should be thoroughly evaluated for evidence of rashes, with special attention to the scalp, gluteal fold, and umbilical areas since these are commonly affected areas by psoriasis and are often overlooked.
Diagnostic Testing
• Inflammatory markers such as ESR and CRP lack sensitivity and specificity and are not diagnostic.
• HLA-B27 test is nonspecific since it is present in up to 8% of the general healthy population. It is estimated that only 5% of the general population with HLA-B27 will develop SpA. The prevalence of HLA-B27 varies across the SpAs, ranging from 30% to 90%.10 Therefore, its positive predictive value is low in the absence of high clinical suspicion.
• If ReA is suspected, infectious workup should be considered.
The triggering infection may have been asymptomatic. Testing for stool pathogens is low yield if the diarrheal illness has resolved. However, in patients with ongoing diarrhea, stool cultures to test for Salmonella, Shigella, Campylobacter, and Yersinia are recommended. In patients with neither gastrointestinal nor genitourinary symptoms or in patients with suspected Chlamydia trachomatis infection, urine testing for chlamydia using nucleic acid amplification techniques may be helpful if the clinical syndrome is consistent with ReA.IMAGING
• X-rays usually detect late changes including sacroiliac erosions or sclerosis or calcification of the spinal ligaments with bridging syndesmophytes (bamboo spine). Peripheral joint x-rays should also be obtained to evaluate for erosions, entheseal calcifications, and osteitis.
• MRI is preferred for early detection of inflammation like sacroiliitis. Typically ordered if there is a high clinical suspicion for SpA and x-rays are negative or equivocal. Supportive findings of sacroiliitis include bone marrow edema (although low specificity), erosions, synovitis, and ankylosis.
• CT is also sensitive for detection of sacroiliitis but involves more radiation.
TREATMENT
Behavioral
• Physical therapy emphasizing extension exercises and posture is recommended to minimize possible late postural defects and respiratory compromise.
• Patients should be instructed to sleep supine on a firm bed without a pillow and to practice postural and deep-breathing exercises regularly.
• Cigarette smoking should be strongly discouraged.
Medications
• NSAIDs, such as indomethacin and selective COX-2 inhibitors, are used to provide symptomatic relief in all SpAs.
• Conventional DMARDs like methotrexate and sulfasalazine provide benefit for peripheral involvement in SpAs.
• Other conventional DMARDs and biologics have been specifically approved for different SpAs.
î AS approved treatments include anti-TNF (inflximab, adalimumab, golimumab, certolizumab pegol), and anti-IL-17 (secukinumab, ixekizumab).
î PsA approved treatments include apremilast, anti-TNF, anti-IL-17, anti-IL-12/23 (ustekinumab, guselkumab), anti CTLA-4 (abatacept), and JAK inhibitors (tofacitinib).
° IBD-associated arthritis approved treatments include anti-TNF (except etanercept since it is ineffective for the treatment of IBD, and it is associated with a higher risk of uveitis in SpA patients). NSAIDs should be used with caution because they may trigger IBD flares. Anti-IL-17 should be avoided as they increase the rate of IBD flares and other adverse events. Use of non-TNF inhibitor biologics for IBD-related arthritis should be a shared decision between the patient, rheumatologist, and gastroenterologist.
î ReA: in patients who fail NSAIDs and conventional DMARDs, anti-TNFs have shown some benefit although they are not FDA-approved for this indication. Treatment for chlamydia infection, if detected, is appropriate. Prolonged empiric antibiotic therapy has not been shown to be beneficial.
î Local injection of glucocorticoids is a useful adjunctive measure.
Surgical Management
Many patients develop osteoporosis in the fused spondylitic spine and are at risk of spinal fracture. Surgical procedures to correct some spine and hip deformities may result in significant rehabilitation in carefully selected patients.
More on the topic Spondyloarthritis:
- Boon Andrew. The Ethics and Conduct of Lawyers in England and Wales. Hart Publishing,1999. — 808 p., 1999
- Griffiths-Baker Janine. Serving Two Masters: Conflicts of Interest in the Modern Law Firm. Hart Publishing,2002. — 227 p., 2002
- Grisso T.. Evaluating Competencies: Forensic Assessments and Instruments. 2nd edition. — Springer,2002. — 564 p., 2002
- Luban David. Legal Ethics and Human Dignity. Cambridge University Press,2007. — 350 p., 2007
- Ayupova Z.K.. Theory of state and law: textbook. - Almaty: Kazakh University,2015. - 192 pages., 2015
- Allen Danielle, Benkler Yochai et al. (eds.). A Political Economy of Justice. The University of Chicago Press,2022. — 416 p., 2022
- Barnes Rudolph C.. Military Legitimacy: Might and Right in the New Millennium.Frank Cass,1996. — 198 p., 1996
- Bedner Adriaan (ed.).. Real Legal Certainty and its Relevance: Essays in Honor of Jan Michiel Otto. Leiden University Press,2018. — 261 p., 2018
- Fridson M., Alvarez F.. Financial Statement Analysis. John Wiley & Sons, Inc.,2002. — 413 p, 2002
- Banking, Finance, and Accounting: Concepts, Methodologies, Tools, and Applications. IGI Global,2014. — 1593 p., 2014
- Hare C., Neo D. (eds.). Trade Finance: Technology, Innovation and Documentary Credit. Oxford University Press,2021. — 417 p., 2021
- Fligstein Neil. The Banks Did It: An Anatomy of the Financial Crisis. Harvard University Press,2021. — 334 p., 2021
- Cline W.. The Right Balance for Banks. Peterson Institute for International Economics,2017. — 281 p., 2017
- Alsharari Nizar Mohammad (ed.). Banking and Accounting Issues. ITexLi,2022. — 175 p., 2022
- AAP. Guidelines for Air and Ground Transport of Neonatal and Pediatric Patients. 4th edition. — American Academy of Pediatrics,2015. — 488 p., 2015
- Ancha S., Auberle C., Cash D., Harsh M., Hickman J., Kounga C.. The Washington Manual of Medical Therapeutics, 37th edition, LWW, 2022. —1250p., 1250