Systemic Lupus Erythematosus
GENERAL PRINCIPLES
Definition
SLE is a multisystem disease of unknown etiology that primarily affects women of childbearing age. The female-to-male ratio is 9:1. It is most common in African Americans and typically occurs in the second and third decades of life.
Pathophysiology
Pathophysiology is multifactorial and incompletely understood, with interplay of genetic predisposition and environmental factors.
DIAGNOSIS
Clinical Presentation
• Disease manifestations are protean, ranging in severity from fatigue, malaise, weight loss, and fever to potentially life-threatening cytopenias, nephritis, cerebritis, vasculitis, pneumonitis, myositis, and myocarditis.
• Photosensitivity is considered a hallmark. Patients often get the “butterfly” rash in the malar area with nasolabial sparing; rash can be seen in all sun-exposed areas. Other symptoms like joint pain, fatigue, and mucosal ulcers can also be triggered by sun exposure.
• Skin involvement is classified as acute, subacute, or chronic. Subacute lupus can present with annular or psoriasiform lesions. Discoid lupus can occur alone or with systemic disease and can cause longterm scaring and pigmentation changes.
• Renal involvement is common and can sometimes be the only or presenting manifestation. It can present with proteinuria gt;500 mg/d, hematuria, pyuria, or elevated creatinine. There are several types of renal disease associated with SLE which can affect the glomerular, tubular, and vascular compartments of the kidney.
• Classification criteria are used primarily for research purposes, but are helpful to review when suspicion arises. Most recent 2019 EULAR/ACR criteria were updated from 2012 SLICC to improve sensitivity and specificity as well as to improve early detection. If ANA (antinuclear antibody) is not present, the patient does not classify as having SLE.
Patients are classified as having SLE with a score of 10 or more points. 2019 EULAR/ACR criteria have a sensitivity of 96.1% and a specificity of93.4%.11
Diagnostic Testing
• Workup should include routine laboratory testing more specific tests as well like antibody and complements levels.
• General tests should include complete blood count (CBC) to look for anemia, leukopenia, or thrombocytopenia; basic metabolic panel for renal dysfunction; urinalysis for hematuria, proteinuria, pyuria, or cellular casts, and urine protein-creatinine ratio. Specific tests include ANA by indirect immunofluorescence, ESR, CRP, and C3 and C4 complement levels.
• It should be noted that up to 15% of the general healthy population have a positive ANA at 1:80.12 Patients with SLE typically have ANA at significant titers (gt;1:320). If ANA is positive, more specific antibodies should be ordered, which include:
î Anti-double-stranded DNA is highly specific for SLE and seen in approximately 70%.
î Anti-Smith is highly specific for SLE as well, but less sensitive and seen in 30%.13,14
î Ro/SSA, La/SSB: these are more commonly associated with Sjogren syndrome but can be seen in with SLE.
o U1 ribonucleoprotein (RNP): always present in patients with mixed connective tissue disease (MCTD) but can be present in 25% of patients with SLE.14
î Antiphospholipid antibodies: lupus anticoagulant, anticardiolipin antibodies, and anti-beta2- glycoprotein can also be present in patients with SLE.
TREATMENT
Medications
• Treatment varies according to disease severity. Patients with only mucocutaneous, musculoskeletal, leukopenia, mild thrombocytopenia, and serositis are considered to have mild disease. Moderate disease is considered in patients who have symptoms that are unresponsive to standard treatment, especially if low C3/C4 and high dsDNA. Severe disease includes lupus nephritis, CNS involvement, pneumonitis, vasculitis, and severe cytopenias.
• NSAIDs usually help SLE-associated arthritis, arthralgias, fever, and mild serositis but not fatigue, malaise, or major organ system involvement. The response to selective COX-2 inhibitors is similar. Hepatic and renal toxicities of NSAIDs appear to be increased in SLE.
• Glucocorticoidtherapy
î Indications for systemic glucocorticoids at high doses include life-threatening manifestations of SLE, such as glomerulonephritis, CNS involvement, thrombocytopenia, and hemolytic anemia. Steroids can also be used as initial therapy for skin rashes, serositis, and joint symptoms for immediate relief of flares.
î Dosage: Patients with severe or potentially life-threatening complications of SLE should be treated with high-dose prednisone (1-2 mg/kg PO daily) which can be given in divided doses. After disease is controlled, prednisone should be tapered slowly, with the dosage being reduced by 10% every 710 days. More rapid reduction may result in relapse. IV pulse therapy in the form of methylprednisolone, 500-1000 mg IV daily for 3-5 days, has been used in SLE in such lifethreatening situations as rapidly progressive renal failure, active CNS disease, and severe thrombocytopenia. Patients who do not show improvement with this regimen are probably unresponsive to steroids, and other therapeutic alternatives must be considered. A course of oral prednisone should follow completion of pulse therapy.
• Hydroxychloroquine 5 mg/kg is recommended for all patients with SLE. It is effective in the treatment of rash, photosensitivity, arthralgias, arthritis, alopecia, and malaise associated with SLE and in the treatment of discoid and subacute cutaneous lupus erythematosus. The drug is not effective for treating major organ manifestations, but long-term usage reduces disease progression number of flares and long-term damage from the disease. Hydroxychloroquine also reduces incidence of thrombosis in lupus patients with antiphospholipid antibody syndrome.
• Immunosuppressive therapy
î Indications for immunosuppressive therapy in SLE include life-threatening manifestations of SLE such as glomerulonephritis, CNS involvement, thrombocytopenia, hemolytic anemia, and the inability to reduce corticosteroid dosage or severe corticosteroid side effects.
î Choice of an immunosuppressive therapy is individualized to the clinical situation. Cyclophosphamide is reserved for life-threatening manifestations of SLE. Azathioprine and mycophenolate mofetil are also used as steroid-sparing agents for serious lupus manifestations. There is increasing evidence that mycophenolate mofetil may be as effective as cyclophosphamide in certain classes of lupus nephritis due to fewer side effects and is particularly preferred in the younger population where fertility maintenance is a concern.15
î Methotrexate is often used for musculoskeletal and skin manifestations. Rituximab has been shown in uncontrolled observational studies to be effective in cases of severe SLE not responding to conventional treatment; however, placebo-controlled studies have been disappointing. Belimumab was approved by the FDA in 2012 for the treatment of adult autoantibody-positive lupus patients who are receiving standard,16 and in 2020, the FDA approved it for lupus nephritis. The addition of belimumab to standard therapy increased the response rate and prevented worsening of renal disease. Voclosporin is a calcineurin inhibitor which does not require monitoring of drug levels. It was approved by the FDA in 2021 for lupus nephritis in combination with standard-of-care therapy. Studies showed marked reduction of proteinuria and higher rates of complete renal response.17 For dosing, side effects, and contraindications of individual medications, please refer to Table 25-5.
TABLE 25-5
SYNTHETIC DMARDS
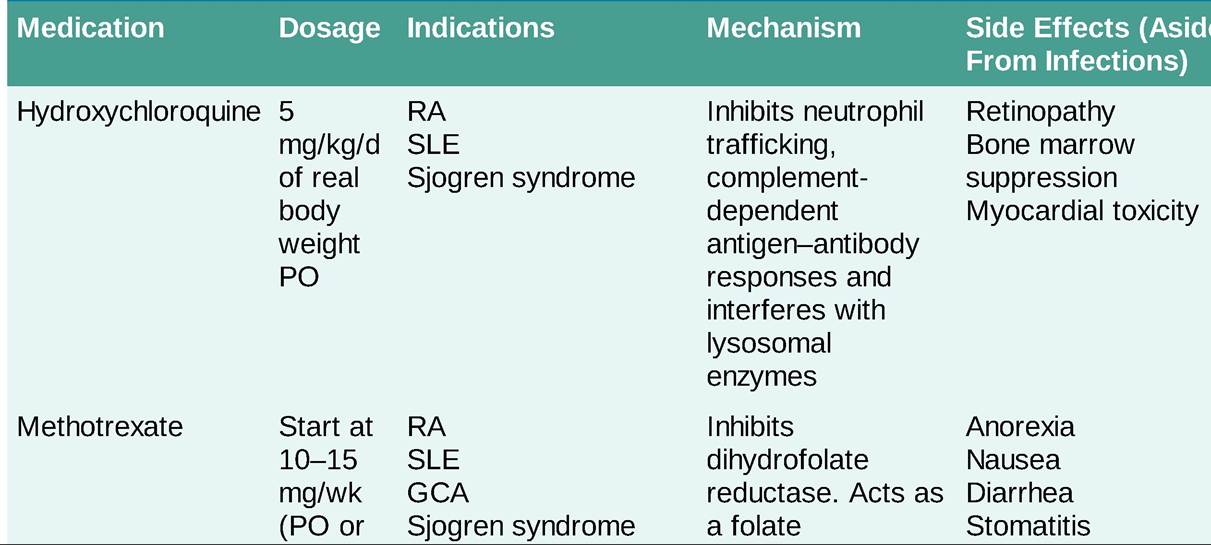
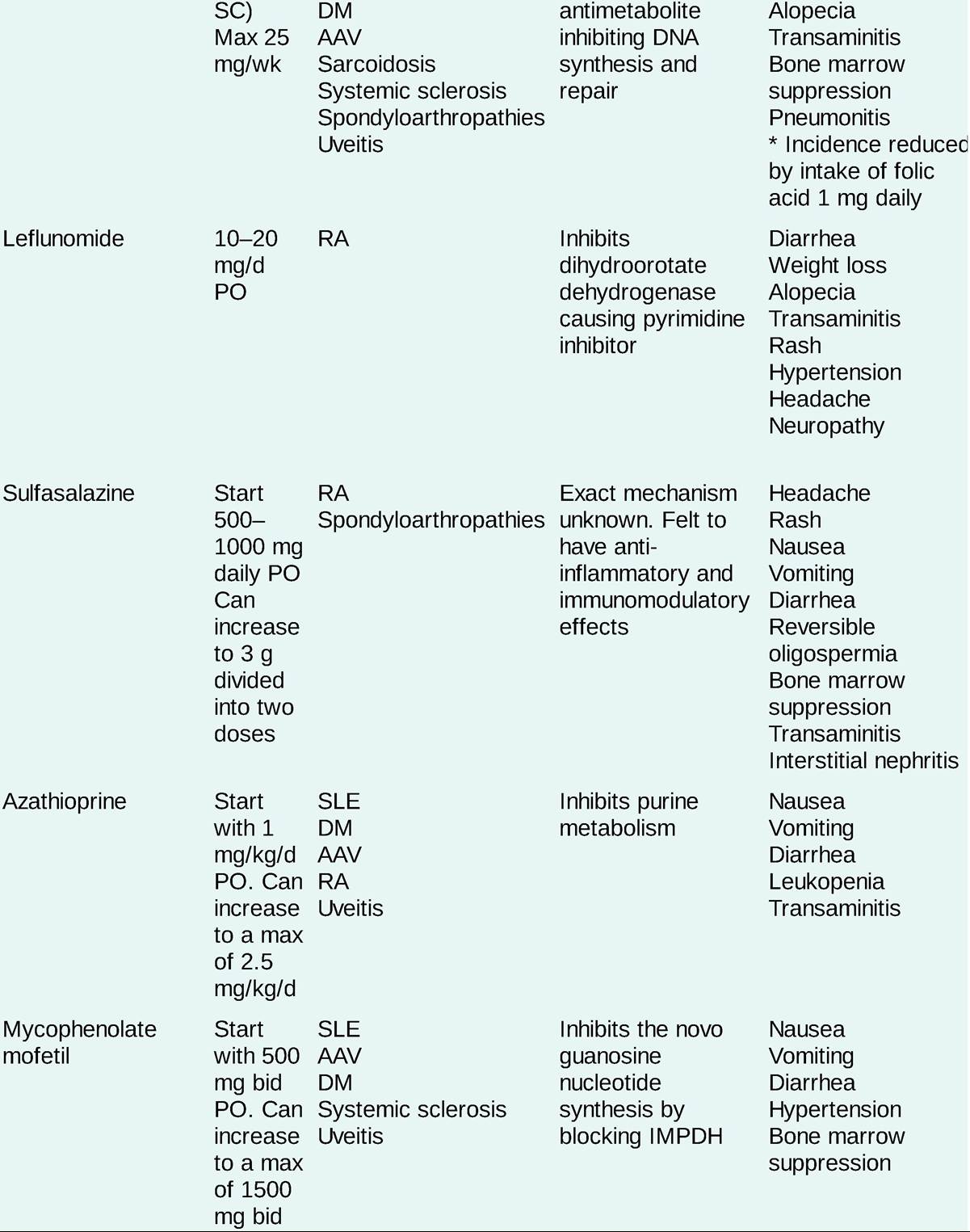
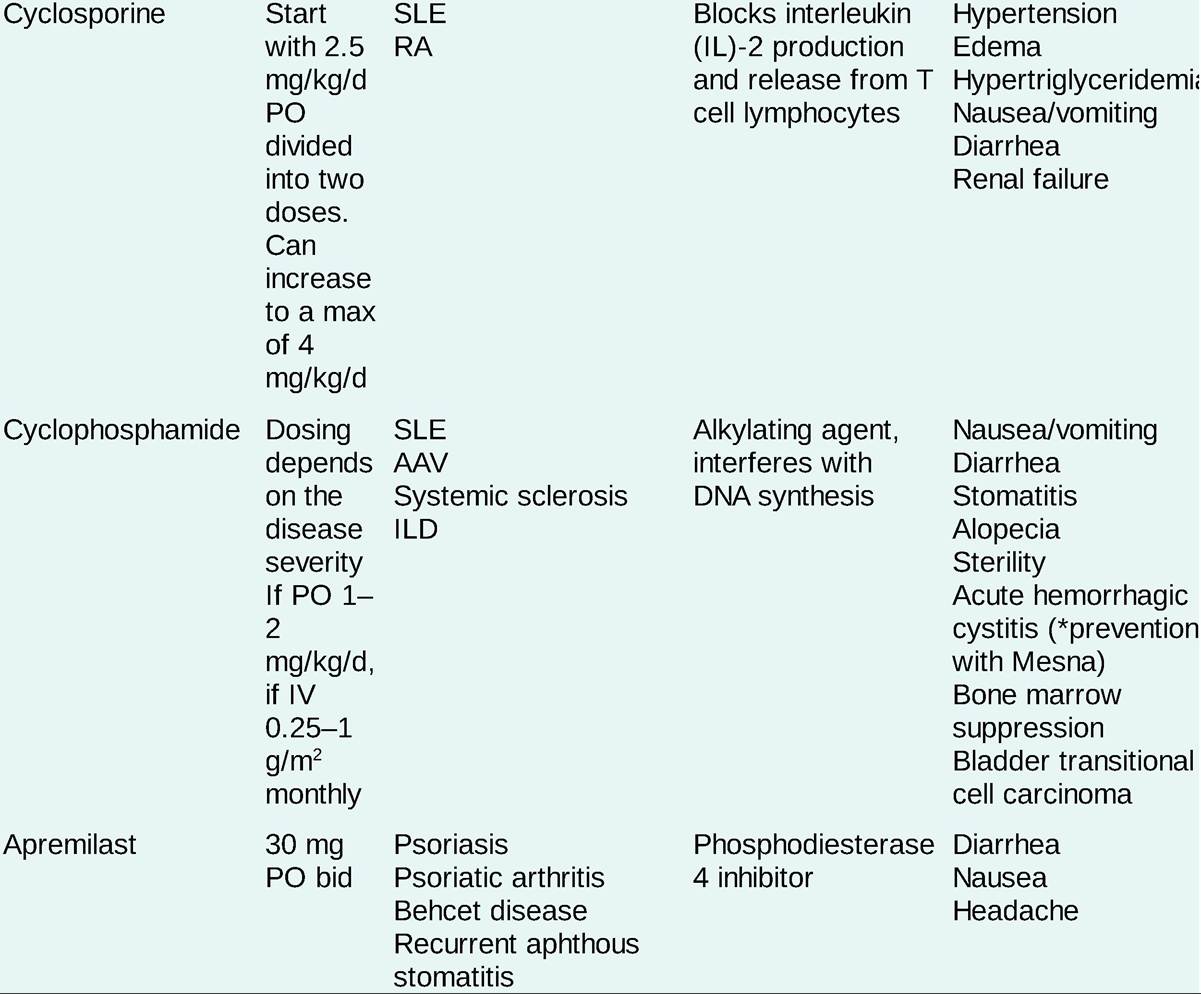
AAV, ANCA-associated vasculitis; DM, dermatomyositis; GCA, giant cell arteritis; ILD, interstitial lung disease; IMPDH, inosine monophosphate dehydrogenase; RA, rheumatoid arthritis; SLE, systemic lupus erythematosus; TPMT, thiopurine S- methyltransferase.
Nonpharmacologic Therapies
• General supportive measures include adequate sleep and fatigue avoidance.
• All patients, not just those with photosensitive rashes, are advised on use of sunscreens with sun protection factor (SPF) of 30 or greater, protective clothing, and sun avoidance. Isolated skin lesions may respond to topical steroids.
[1] Consider prophylaxis against Pneumocystis pneumonia in patients treated with cyclophosphamide. Also consider adding prophylaxis for the prevention of bladder and gonadal toxicity from this agent. Appropriate immunizations should be considered prior to initiation of immunosuppressive therapy, especially against influenza and pneumococcus. Immunization with live vaccines is contraindicated in immunosuppressed patients.
SPECIAL CONSIDERATIONS
• Patients with lupus have accelerated coronary and peripheral vascular disease, especially with high disease activity and chronic steroid use, and cardiovascular risk factors should be managed aggressively.
• Transplantation and chronic hemodialysis have been used successfully in SLE patients with renal failure. Clinical and serologic evidence of disease activity often remits when renal failure ensues.
• Pregnancy in SLE: An increased incidence of second-trimester spontaneous miscarriages and stillbirths has been reported in women with antibodies to cardiolipin or lupus anticoagulant. SLE patients may experience flares during pregnancy if the lupus is active at the time of conception. Differentiation between active SLE and preeclampsia is often difficult. Women in whom SLE is well controlled are less likely to have a flare of disease during pregnancy.
• Neonatal lupus may occur in offspring of anti-SSA- or anti-SSB-positive mothers, with skin rash and heart block being the most common manifestations. Drug-induced lupus typically has a sudden onset and is associated with serositis and musculoskeletal manifestations. Renal and CNS manifestations are rare. Serology includes positive ANA and antihistone antibodies, negative anti-SM, and anti-doublestranded DNA antibodies along with normal complement levels. The disease usually resolves with drug discontinuation. Offending drugs include procainamide, hydralazine, minocycline, diltiazem, isoniazid, chlorpromazine, quinidine, methyldopa, and anti-TNF biologics.
More on the topic Systemic Lupus Erythematosus:
- SYSTEMIC LUPUS ERYTHEMATOSUS
- Lupus Nephritis
- Systemic Sclerosis
- SYSTEMIC RISK EXPOSURES AND LOSSES
- SYSTEMIC RISK AND PORTFOLIO DIVERSIFICATION
- COUNTERPARTY SYSTEMIC RISK
- Systemic Antimicrobials
- Systemic Relevance of Financial Institutions
- SYSTEMIC CONNECTIVE TISSUE DISORDERS
- Systemic and Pulmonary Mycoses