SYSTEMIC LUPUS ERYTHEMATOSUS
Systemic lupus erythematosus (SLE) is a multi-systemic autoimmune disorder, characterized by presence of antinuclear antibodies (ANA) and inflammatory damage to virtually any organ, especially skin, synovium, blood cells, kidney and CNS.
Epidemiology: SLE is one of the commonest rheumato- logical disorders, predominantly affecting females (gt; 4:1) with peak age of onset in adolescence, frequently corresponding to menarche.
Etiopathogenesis involves hallmark development of autoantibodies against many cell antigens, e.g. DNA, other nuclear antigens and blood cells, leading to immunecomplex mediated injury in target organs.
While exact cause for autoimmune phenomena is obscure, important hypotheses suggest—(a) genetic basis with high incidence of disease in certain HLA types, e.g. B8, DR2 and 3, (b) defective apoptosis of self-reactive T-cells in fetal life, (c) non-specific response to a specific antigen, e.g. virus or drugs, and (d) role of female sex hormones in altered immune response.
Pathology in target organs is characterized by presence of fibrinoid deposits in vascular walls and certain hematoxylin stained bodies (LE cells) in parenchymal tissues. LE cell is a modified polymorph, ready for phagocytosis after reacting to antinuclear antibody against own deoxyribonucleoprotein (DNP).
Clinical presentation: SLE is rare below 5 years of age, usually diagnosed in adolescent females. Natural course is highly unpredictable, ranging from chronic smoldering disease to acute life-threatening illness. Most cases begin with:
a. Constitutional symptoms, e.g. prolonged fever, weight loss and fatigue.
b. Butterfly skin rash over malar prominences and nasal bridge (Fig. 24.2), which may be photosensitive and varies in appearance from a simple erythematous flush to thickened epidermis with scaly patches. Other
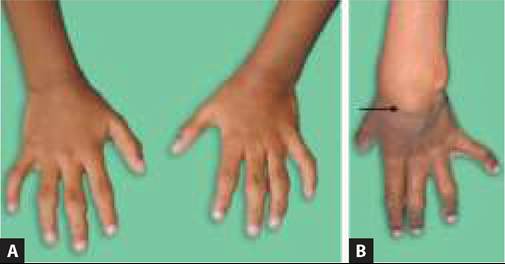
Fig.
24.2: Systemic lupus erythematosus: Butterfly rash.skin lesions, e.g. discoid lesions, vasculitis purpura or livedo reticularis (generalized lace-like discoloration) are common but not diagnostic.
c. Arthralgia or arthritis, specially involving small joints and disproportionately more painful than local signs. Residual deformities are uncommon during childhood.
d. Renal involvement of variable severity (Lupus nephritis) in 30-40%, presenting with hematuria, proteinuria, hypertension and renal failure. Lupus nephritis is pathologically classified into six types (I-VI) and renal biopsy is essential for therapeutic decision making.
Other important systemic manifestations of SLE may appear during the course of disease and include:
• GIT involvement as abdominal pain, diarrhea, melena, etc. due to peritoneal serositis and/or vasculitis,
• Pulmonary involvement as pleuritis or hemorrhage,
• Neurological involvement as seizures, psychosis or strokes,
• Cardiac involvement as pericarditis, conduction defects, coronary vasculitis, CCF, and
• Hematological involvement with Coombs-positive hemolytic anemia, thrombocytopenia, etc.
Diagnosis rests on the essential presence of Entry criteria, i.e. ANA Positivity gt;1:80 on Hep2 cells or equivalent test, and a total score of 10 (including 1 clinical criteria) on additive criteria, as per EULAR/ACR classification Criteria 2019 (Table 24.7). Additive criteria may be present at the same or different times during course of illness and must have no alternative explanation.
Important laboratory investigations include:
• Screening ANA test, to detect non-specific antinuclear antibodies, which are present in almost all cases of SLE
TABLE 24.7: EULAR/ACR* criteria for diagnosis of SLE
Entry criteria (Essential) ANA positive gt;1:80 on Hep2 cells or equivalent positive test Additive criteria (+Total score of #8805;10 and #8805;1 clinical criteria)
*European League Against Rheumatism/American College of Rheumatology
• Do not count a criteria in presence of alternative explanation
• Presence of criteria at least on one occasion is sufficient
• Criteria need not be present simultaneously
• Within each domain, only highest weighted criterion must be counted
but also in other rheumatic and infective conditions (Ch 24.1). A false-positive VDRL test or RF may also suggest SLE in suspected case.
• Anti-ds DNA test to detect lupus-specific anti-DNA antibodies, which also reflect degree of disease activity. Anti-Sm antibodies are also lupus-specific.
• Low serum complement levels (CH50, C3, C4), which gradually normalize with remission, are useful to monitor response to therapy.
• Tests for other tissue-specific antibodies, e.g. Coombs test, anti-thyroid antibodies, etc. in selected cases.
• Organ-specific Investigations, e.g. renal biopsy or radioimaging with USG/CT/MRI in selected cases.
Management depends on the extent and severity of disease, guided by clinical features and serological markers (Anti-ds DNA antibodies, complement levels):
• Mild and localized disease, without renal or lifethreatening organ involvement is generally treated with NSAIDs and hydroxychloroquine (PO 3-5 mg/kg/day). Retinal toxicity is a major concern on hydroxychloroquine therapy and needs regular ophthalmic monitoring.
• Moderate multisystemic disease, but without lifethreatening involvement of kidneys or other vital organs, is treated with corticosteroids, i.e. Prednisolone (PO 1-2 mg/kg/day) in divided doses till normalization of complement levels, followed by single dose alternate-day therapy for next 2-3 years. Severe cases may be treated with IV pulse methylprednisolone (30 mg/kg OD for 3 days) initially, followed by oral steroid therapy. Steroid-sparing agents, e.g. hydroxychloroquine, mycophenolate or azathioprine may be used with steroids for long-term treatment.
• Severe multisystemic disease and presence of Class III or IV lupus nephritis requires aggressive therapy with drugs, e.g. cyclophosphamide and biologic agents, e.g. Rituximab.
Role of other modalities, e.g. cyclosporine, hormone therapy, stem-cell transplant and anti-cytokines is in experimental stage.
Additional therapy is indicated in selected cases,
e. g. anticoagulant therapy in thrombotic episodes, antihypertensives in renal disease, anticonvulsants in CNS disease, etc.
Avoidance of direct sun exposure and use of sunscreens in advised to all cases, apart from other supportive measures.
Prognosis: 5-year survival rate is ~85% with current therapeutic regimes, though some patients may ultimately succumb to renal disease, cerebrovascular events or therapy-related opportunistic infections.
Neonatal lupus: Newborns born to mothers suffering from SLE may develop neonatal lupus due to transplacental transfer of antibodies (specially anti-RO/ SSA and anti-LA/SSB antigens), presenting with-
(a) congenital heart block, (b) cutaneous lesions, (c) hematological manifestations, e.g. hemolytic anemia or thrombocytopenia, and (d) rarely, other systemic manifestations. All newborns with antibody transfer do not necessarily manifest clinically and most manifestations resolve soon after birth. However, congenital heart block is permanent and requires cardiac pacing.
Drug-induced lupus: Many drugs have been implicated in presentation of lupus-like features or aggravation of SLE, including anticonvulsants, e.g. Phenytoin, Carbamazepine, Valproate etc. Antitubercular drugs, e.g. INH and Rifampicin and others, e.g. penicillamine, Amiodarone, and Procainamide, etc.
24.3.2
More on the topic SYSTEMIC LUPUS ERYTHEMATOSUS:
- Agrawal M.. Textbook of Pediatrics. 3rd ed. — CBS Publishers,2025. — 973 p., 2025
- Sexually Transmitted Diseases