The Poisoned Patient
GENERAL PRINCIPLES
• Patients who present to the hospital with an overdose or toxic exposure can be challenging for the clinician. This section will review the general approach to the poisoned or potentially poisoned patient.
Specific toxins will be discussed in the sections that follow.• When managing the poisoned patient, prioritize basic supportive care measures, including airway protection and support of respiration and circulation.
Definition
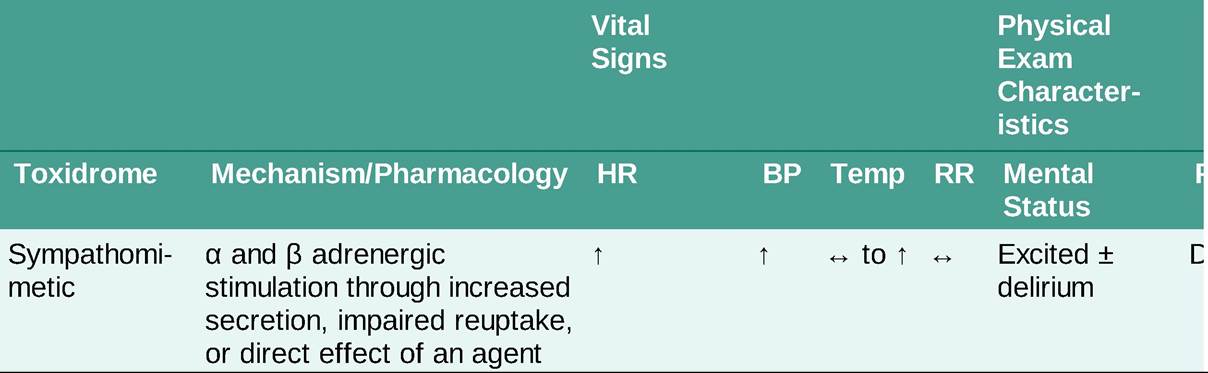
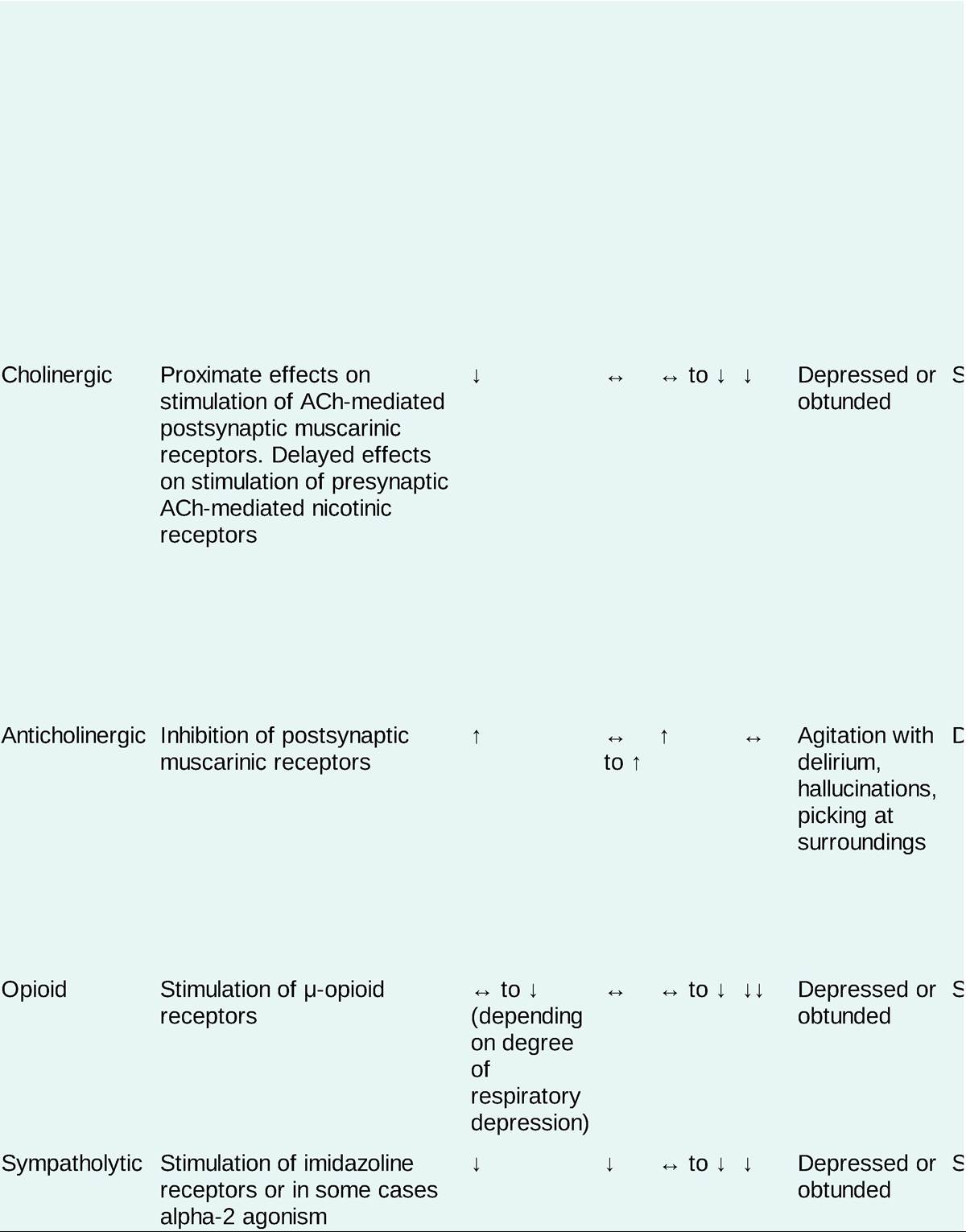
• A toxidrome, or toxic syndrome, is a constellation of clinical examination findings that assists in the diagnosis and treatment of the patient who presents following an exposure to an unknown agent.
• The toxidromes are generally defined by vital signs, pupillary diameter, skin and mucous membrane findings, and mental status. In certain cases, bowel and bladder function may also be relevant. See Table 28-1.
TABLE 28-1
TOXIDROMES
DIAGNOSIS
Diagnostic Testing
Diagnostic testing is typically guided by historical features of the exposure and physical exam findings. Very few diagnostic tests are helpful without history or physical exam findings to suggest an exposure.
LABORATORIES
• Finger stick blood glucose (FSBG): This test should be considered one of the vital signs in the patient with altered mental status.
• Chemistry: A basic metabolic profile should be ordered on any patient with a toxic exposure. The most important components of the basic metabolic panel (BMP) are the bicarbonate, anion gap, and creatinine.
î Bicarbonate: The presence of acidosis is an important indicator of the presence and severity of poisoning by many important xenobiotics (e.g., toxic alcohols, salicylates, iron, and metformin).
° Anion gap: An elevated anion gap acidosis in a poisoned patient should prompt testing for ketones, lactate, salicylates, and in certain select circumstances toxic alcohols.
î Creatinine: Many important xenobiotics are renally excreted; impaired renal function may require treatments such as hemodialysis for toxin removal.
• Blood gas: In most cases of intoxication, pH rather than oxygenation is relevant. Therefore, it is reasonable to send venous blood gases (VBGs) rather than arterial blood gases (ABGs) in most cases. However, if adequate oxygenation is a concern (e.g., cyanide, carbon monoxide poisoning, methemoglobinemia), then an ABG should be sent.
î Co-oximetry (i.e., testing for dyshemoglobins such as methemoglobin or carboxyhemoglobin) can be performed on arterial or venous samples.
• Serum acetaminophen (V-acetyl-p#945;r#945;-aminophenol [APAP]): APAP is widely available and potentially life-threatening in overdose. Screening for acetaminophen should be performed in any patient presenting with an intentional overdose.
• Serum salicylate: The authors recommend universal screening for salicylates in patients with intentional overdoses (although other physical exam/chemistry findings may be also present).
• Serum ethanol: Routine or universal testing or ethanol is not helpful. Ethanol intoxication remains primarily a clinical diagnosis. Ethanol testing is necessary as part of the workup for toxic alcohol poisoning.
• Urine drug screen (UDS): This test is rarely helpful in the acute medical management of the poisoned or potentially poisoned patient. Clinical treatment should be guided by signs/symptoms of poisoning (toxidrome). The UDS is a test of exposure, not a test of intoxication. Appropriate UDS with confirmatory reflex testing may be useful for forensic purposes (e.g., drug-facilitated sexual assault, elder abuse). The UDS tends to vary between hospitals but often tests for the following substances:
î Amphetamines: The assay for amphetamines commonly cross-reacts with over-the-counter cold medications.
Many designer amphetamines will not be detected.î Opiates: Detects only substances naturally derived from or metabolized to components of the opium poppy (morphine, codeine). Testing for specific synthetic opioids is typically performed as a separate test and may not be readily available.
° Methadone: Susceptible to false positives, particularly with psychotropic medications such as quetiapine and certain antidepressants.
î Cocaine: Almost all drug screening assays for cocaine are directed at the cocaine metabolite benzoylecgonine (BEG), as cocaine is rapidly metabolized by cholinesterases in vivo. This metabolite itself is also short-lived and a positive cocaine screen typically indicates exposure within the last 3-4 days. 1 The BEG immunoassay is not typically susceptible to false-positive results.
î Cannabinoids: Detection of tetrahydrocannabinol (THC) metabolites is a reliable indicator of cannabis use. Heavy cannabis users may continue to test positive for THC metabolites for several weeks after cessation. In general, synthetic cannabinoids will not cause a positive test result.
î Benzodiazepines: The detection of benzodiazepines most commonly relies on the detection of oxazepam (nordiazepam); therefore, commonly used benzodiazepines that are not metabolized to oxazepam (such as lorazepam, clonazepam, alprazolam) are not consistently detected. Some commercial screening assays do specifically test for benzodiazepines such as clonazepam or alprazolam, but this is not universal.
î Phencyclidine (PCP): Screening assays may cross-react with dextromethorphan, ketamine, and diphenhydramine to produce a false-positive result.
ELECTROCARDIOGRAPHY
• The ECG is a critical part of the toxicologic evaluation, as certain overdoses produce characteristic ECG changes that guide diagnosis and treatment.
• In general, cardiac toxins tend to prolong the PR interval (reflecting nodal blockade), the QRS (reflecting sodium channel blockade), or the QT interval (potassium channel blockade).
î The specific prolongation of segment from the end of the ventricular depolarization to the end of repolarization (“JT” interval) is characteristic of toxic exposures that directly antagonize the IKr potassium channel. Toxins that antagonize the fast cardiac sodium channels will prolong the QRS interval; this will by definition impact the QT interval as well, as the QT interval includes the QRS interval.
î Automatic correction of the QT interval for heart rate (e.g., by Bazett's method) may overestimate the risk of ventricular dysrhythmia in poisoning. An alternate means of correction such as the QT nomogram (Figures 28-1) may more accurately represent the risk of dysrhythmia from QT prolongation in poisoning. 2
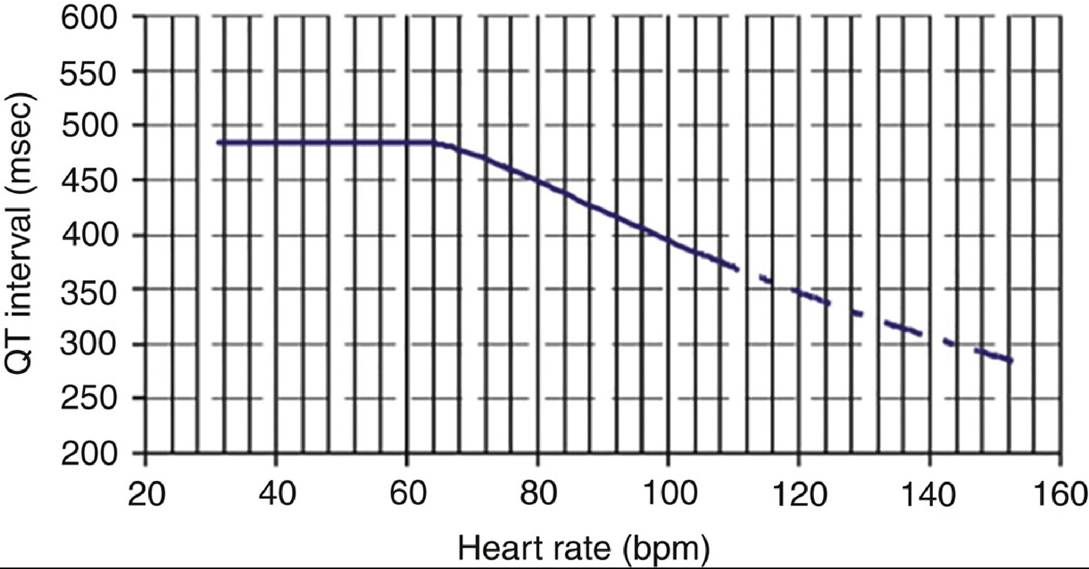
Figure 28-1 Qt interval nomogram(Adapted from Chan A, Isbister GK, Kirkpatrick CMJ, Dufful SB. Drug-induced QT prolongation and torsades de pointes: evaluation of a QT nomogram. QJM. 2007;100(10):609-615, by permission of Oxford University Press.)
IMAGING
• In general, diagnostic imaging has a limited role in toxicology.
• An abdominal radiograph may reveal radiodense material in the gastrointestinal (GI) tract of patients who have ingested certain radiopaque toxins, namely chloral hydrate, metals, certain antipsychotics, and enteric-coated or sustained-release pharmaceuticals.
• Occasionally, subtle abnormalities on the abdominal film will detect the presence of “rosettes” or elongated packets in the GI tract of body packers (patients who swallow hundreds of packets of drugs in an attempt to smuggle them). The abdominal film is of limited utility in body stuffers (patients who ingest small quantities of poorly packaged drugs to evade detection by law enforcement).
TREATMENT
• Prevention of absorption: GI decontamination should not be performed routinely or indiscriminately. It is most helpful in patients who present early, have ingested large quantities of xenobiotics, and/or have ingested dangerous xenobiotics without other effective treatments.
î Induction of emesis (via ipecac or salt administration) is never indicated.
î Gastric lavage is inefficacious in most cases and is uncomfortable for the patient and technically challenging to perform. It may have a limited role in the small subset of patients who present rapidly following ingestion of dangerous xenobiotics, liquid xenobiotics, or xenobiotics not adsorbed by activated charcoal. Lavage via a standard-bore orgogastric or nasogastric tube is ineffective for solids/pill fragments. An Ewald tube is required, which may not be readily available.
î Activated charcoal (AC) nonspecifically adsorbs most chemicals and xenobiotics, preventing their absorption into the circulation.
#9632; The clinical utility of this method of decontamination is diminished if the ingestion occurred more than 1-2 hours before presentation in most ingestions. As such, most toxicologists do not routinely recommend the administration of AC.
#9632; Patients at risk for decreased mental status or seizures should not be given AC owing to concerns for aspiration; patients whose airways are protected by intubation may be given AC per tube.
#9632; AC should be dosed to produce a ratio of at least 10:1 AC to ingested drug by weight (g/g), with the caveat that 100 g of AC is typically the highest one-time dose an awake patient can tolerate.
î Whole-bowel irrigation (WBI) involves the administration of massive quantities of polyethylene glycol with electrolytes (PEG-ELS) to clear the GI tract of ingested material by bulk action.
#9632; WBI may be considered in patients who have ingested sustained-release medications, patients who have ingested metals that do not bind to AC (e.g., iron, lithium, lead), or in body packers.
#9632; The optimal dose of PEG is 1-2 L/h until the rectal effluent is clear. It is usually necessary to place a nasogastric tube to administer this volume of fluid.
î Cathartics have no role in the management of overdose. They are often present in the premixed AC solutions.
If this is the case, only one dose should be administered.î All GI decontamination interventions are contraindicated in the presence of airway compromise, persistent vomiting, and the presence of an ileus, bowel obstruction, or GI perforation.
• Enhanced elimination: In certain circumstances, techniques to promote the rapid elimination of toxins may be helpful.
î Forced diuresis with intravenous crystalloid is typically not useful. It may have a role in the treatment of lithium poisoning.
î Urinary alkalinization with intravenous sodium bicarbonate enhances the elimination of weak acids and is useful in the setting of salicylate overdose and certain other poisonings.
° Multidose activated charcoal (MDAC), as opposed to single-dose AC discussed above, may enhance the elimination of certain xenobiotics that undergo enterohepatic recirculation (most importantly quinine, theophylline, carbamazepine, phenobarbital, and dapsone).
î Hemodialysis and other extracorporeal elimination methods may be indicated in serious poisonings by specific dialyzable xenobiotics. Hemodialysis may also be used to correct acid-based disorders due to poisoning, even when it does not directly remove a significant amount of xenobiotic.
• Antidotes: Antidotal therapy is indicated only in specific circumstances and should not be administered indiscriminately.
SPECIAL CONSIDERATIONS: SEIZURES IN POISONING
• Many poisonings and withdrawal syndromes produce seizures. Toxic seizures are usually generalized and tonic-clonic; nonconvulsive status epilepticus and focal seizure are rare in toxicology.
• Generally speaking, it is not necessary to preemptively or prophylactically treat patients at risk for toxic seizures. Exceptions include chloroquine and hydroxychloroquine and the cholinesterase inhibitor pesticides and nerve agents.
• Toxic seizures should be treated with agents that directly enhance GABAergic tone.
î Benzodiazepines are the first-line agent of choice. They do not directly open the GABA-A chloride channel, but rather enhance opening in response to endogenous GABA binding.
î Barbiturates may be used in patients refractory to benzodiazepines. Unlike benzodiazepines, barbiturates open the GABA-A chloride channel even in the absence of endogenous GABA, and thus may be particularly helpful in patients with impaired GABA synthesis (e.g., hydrazine poisonings, severe alcohol use disorder [AUD]).
î Propofol also directly opens the GABA-A chloride channel. It is an excellent choice in intubated patients who are experiencing or at risk for toxic seizures.
î Parenteral pyridoxine may be helpful in select cases, especially in hydrazine poisoning (isoniazid, Gyromitra esculenta, hydrazine fuels) and in malnourished patients.
• Anticonvulsants that are not directly GABAergic should not be used to treat toxic seizures.
î Levetiracetam and other anticonvulsants used in epilepsy (e.g., valproate, carbamazepine, lacosamide, zonisamide) are likely ineffective in poisoned or withdrawing patients.
î Phenytoin may actually be harmful in certain poisonings (e.g., theophylline) and should be avoided. 3