Acetaminophen
GENERAL PRINCIPLES
Epidemiology
• APAP is available worldwide as an over-the-counter analgesic and antipyretic. It is a common component of cold and flu remedies and is often sold in combination preparation together with nonsteroidal anti-inflammatory drugs (NSAIDs), opioids, or sedatives.
• APAP is available in multiple formulations, including tablets, extended-release tablets, capsules, liquids, suppositories. An intravenous formulation is also available.
• In the US, APAP is the most common pharmacologic agent involved in toxicologic fatalities and the most common cause of acute liver failure.
Pathophysiology
• APAP is a centrally active cyclooxygenase (COX) inhibitor with analgesic and antipyretic effects.
• In therapeutic doses, APAP is primarily metabolized via phase II conjugation enzymes in the liver, which generates nontoxic conjugate products. Small amounts of APAP are metabolized by phase I enzymes (primarily cytochrome P450 2E1), producing a toxic oxidizing metabolite, A-acetyl-p- benzoquinone imine (NAPQI). NAPQI is then detoxified by glutathione.
• In cases of APAP toxicity, the phase II conjugation enzymes are saturated, and a higher proportion of APAP is metabolized via oxidation to NAPQI. Conjugation of NAPQI by glutathione occurs until cellular glutathione is depleted, after which the toxic NAPQI and other free radicals accumulate and cause damage to the hepatocytes.
• Toxicity may occur after a large APAP overdose or after the repeated use of supratherapeutic amounts of APAP.
• Conditions that reduce glutathione stores (such as fasting, malnutrition, and chronic heavy alcohol use) or induce CYP 2E1 (chronic heavy alcohol use, phenytoin and other anticonvulsants, isoniazid) predispose patients to APAP toxicity.
DIAGNOSIS
Clinical Presentation
• 0-24 hours—Asymptomatic (stage 1)
î Early symptoms are nonspecific and primarily related to irritation of the GI tract by ingested tablets (nausea, vomiting, and anorexia).
î This initial phase has few symptoms and patients generally appear clinically well. If a patient exhibits significant vital sign abnormalities or symptoms in the first 24 hours following ingestion, consider other co-ingestants.
î In rare cases, patients who ingest supermassive quantities of APAP may present early with encephalopathy and metabolic acidosis, as APAP is a direct mitochondrial toxin at extremely high concentrations.
• 24-48 hours—Hepatotoxic (stage 2)
î Right upper quadrant abdominal pain is the most common symptom.
î Transaminase elevations and elevated prothrombin time (PT)Zinternational normalized ratio (INR) develop in this phase.
• 2-4 days—Fulminant hepatic failure (stage 3)
î Significant hepatic dysfunction, potentially including fulminant hepatic failure, develops. Jaundice, severe coagulopathy, thrombocytopenia, hypoglycemia, hepatic encephalopathy, and renal injury may be present.
• 4-14 days—Recovery (stage 4): If stage 3 is survived, the hepatic dysfunction usually resolves over the following daysZweeks. If renal injury occurred, it would typically resolve slowly during this phase.
HISTORY
• Obtain a reliable time of ingestion to accurately predict the risk of hepatotoxicity after acute overdose.
• Characterize the time course of poisoning—was there a single acute overdose, or was there repeated supratherapeutic use, chronic overdose, or a staggered overdose (occurring over the course of several hours)?
• Obtain as much information as possible about the amount of APAP that has been ingested, the formulation ingested (for example, combination preparations, extended-release form), and the period over which the overdose occurred.
• Obtain information about co-ingestants (alcohol, other medications, other drugs) and comorbid conditions (especially heavy alcohol use and hepatic disease).
PHYSICAL EXAMINATION
• As in all poisoned patients, assess airway, breathing, circulation, and mental status. These will generally be normal in isolated APAP poisoning, except in patients who present to medical care late (already in stage 3) or in the rare patients who ingest supermassive quantities of APAP.
• Right upper quadrant tenderness, jaundice, or evidence of hepatic encephalopathy (mental status changes, asterixis) may be present in those presenting late to medical care (in stage 2 or 3 of poisoning).
Diagnostic Criteria
• In general, an APAP dose of 150 mg/kg or higher is potentially toxic and may require therapeutic intervention. Unfortunately, the total dose ingested is frequently inaccurate or unknown.
• Use the modified acetaminophen (Rumack-Matthew) nomogram (Figures 28-2) to predict the risk for hepatotoxicity in acute APAP poisoning. 4 This nomogram is not applicable in cases of chronic poisoning, poisoning due to repeated supratherapeutic use, poisoning due to ingestions that are staggered over several hours, or poisoning by the extended-release APAP formulation.
î Obtain a serum APAP concentration at 4 hours or later after ingestion. APAP concentrations obtained before 4 hours postingestion have no prognostic value.
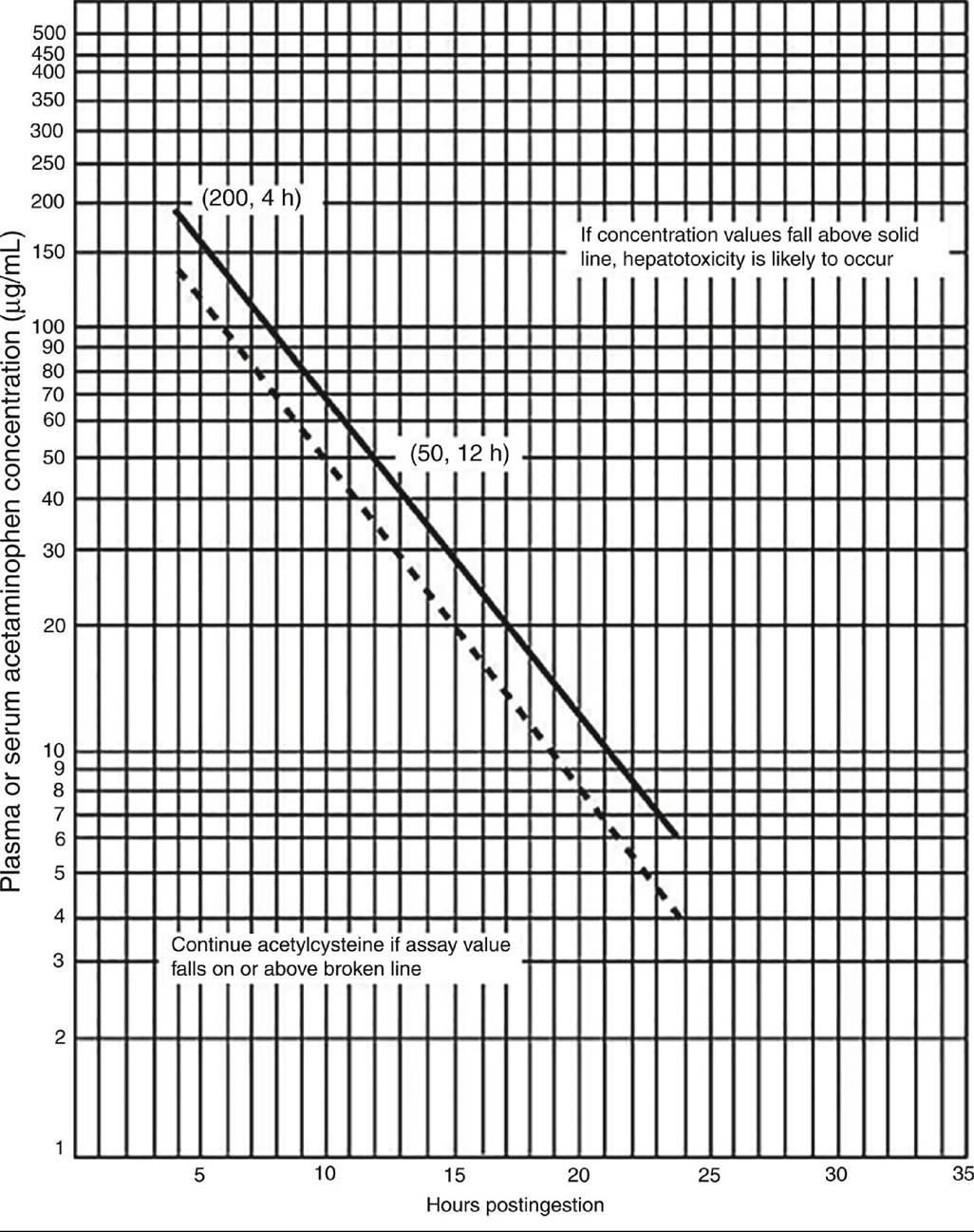
Figure 28-2 Acetaminophen (Rumack-Matthew) nomogram(Reproduced with permission from Rumack BH, Matthew
H. Acetaminophen poisoning and toxicity. Pediatrics. 1975;55(6):871-876. Copyright © 1975 by the American Academy of Pediatrics.)
î If the patient plots below the treatment line with an accurate time of ingestion, no further testing or treatment is necessary.
• It is challenging to predict hepatotoxicity in patients with staggered, subacute, or chronic APAP ingestions, or ingestions that cannot be accurately timed. These patients should generally be treated with NAC.
• During treatment of APAP overdose, it is important to assess the risk of liver failure that may require evaluation for hepatic transplantation. The King's College Hospital (KCH) criteria provide prognostic markers that help to predict the probability of developing severe liver damage (Table 28-2). 5
TABLE 28-2
KING’S COLLEGE CRITERIA
pH lt; 7.3 a or
Lactate gt; 3.5 mmol/L at 4 h a or
Lactate gt; 3.0 mmol/L at 12 h a or
INR gt; 6.5, creatinine gt; 3.4 mg/dL, and severe hepatic encephalopathy (grade III or IV)
Other prognostic factors
Phosphate gt; 3.72 mg/dL on days 2-4
aAfter fluid resuscitation.
The decision to transfer a patient to a transplant center for evaluation is complex and should take into account local practice patterns, logistics, and risk tolerance in addition to the KCH criteria. Generally speaking, patients who meet none of the KCH criteria may be safely managed at a nontransplant center.
Diagnostic Testing
• Serum APAP at four or more hours after ingestion (see earlier discussion).
• Hepatic function panel (HFP) to assess for transaminase elevations that indicate the presence of hepatocellular injury.
• Testing for evidence of hepatic failure (PT/INR, bilirubin, pH, lactate, phosphate, and renal function panel) is not generally required at presentation in patients with acute overdose who present to medical care rapidly but may be necessary later in hospitalization or in patients who present late in the course of poisoning.
NAC therapy can cause minor interference in the PT/INR assay; this does not indicate an in vivo coagulopathy and will not elevate the INR above 2.0.
TREATMENT
• GI decontamination is generally not required or useful in APAP poisoning. Some authors advocate for AC administration in patients who present within 1-2 hours of overdose and have no contraindications to AC.
• N-Acetylcysteine (NAC): NAC is the specific antidote to prevent APAP-related hepatotoxicity. NAC replenishes depleted glutathione stores, directly detoxifies NAPQI, and counteracts oxidative stress caused by NAPQI. It is most effective when administered within 8 hours after ingestion, although it will still have a hepatoprotective effect even beyond this time. 6
• When dosed appropriately (Table 28-3), IV NAC is very safe. There is a small risk of rate-related anaphylactoid reactions (flushing, headache, nausea, pruritus), which typically resolve with antiemetics, antihistamines, and in some cases slowing the infusion rate of IV NAC. A one-bag method (Table 28-3) may help reduce administration delays and dosing errors. 7
TABLE 28-3
DOSING OF N-ACETYLCYSTEINE
| Oral | IV (Authors’ One-Bag Protocol) | IV (FDA Package Insert) | |
| Loading dose | 140 mg/kg | 150 mg/kg over 1 h | 150 mg/kg over 1 h |
| Subsequent doses | 70 mg/kg q4h ?17 doses (72 h) | 12.5 mg/kg/h for 20 h or longer | 12.5 mg/kg/h for 4 h |
| 6.25 mg/kg/h for 16 h | |||
| Comments | Sulfur taste, recommend lid with straw, antiemetics PRN. Use only if IV NAC not readily available | Less errors and stoppage with this method + programmable IV pump | Original FDA approval dosing used in many hospitals |
When to stop IV NAC: 21 h + AST lt; 50% of peak, INR lt; 2.0, clinical improvement
• NAC indications: NAC treatment should be started in the following circumstances:
î Any patient after acute poisoning with a toxic APAP level according to the modified Rumack- Matthew nomogram.
î If the determination of the initial acetaminophen level and potential initiation of treatment with NAC is anticipated to be delayed longer than 8 hours postingestion (e.g., due to late presentation or lab or pharmacy delays). In this circumstance, NAC may be stopped if the APAP level is ultimately determined to be nontoxic.
î Patients who present more than 24 hours after acute ingestion and still have a detectable serum APAP level or elevated AST.
î Patients with chronic supratherapeutic APAP exposure (i.e., gt;4 g/d or gt;2 g/d in patients with significant hepatic disease or heavy alcohol use) who present with elevated transaminases or unmetabolized APAP.
î Patients with signs of fulminant hepatic failure, regardless of etiology. NAC has been shown to improve transplant-free survival of patients in fulminant hepatic failure.
î Patients poisoned by other xenobiotics that cause oxidative hepatocellular damage, such as Amanita phalloides mushrooms, carbon tetrachloride, and eugenol.
More on the topic Acetaminophen:
- Necrosis
- Adverse Drug Reactions
- Drug-Induced Liver Injury
- Acute Liver Failure
- Pain
- Acute Burn Management
- Index
- REFERENCES
- Index
- Index
- Boon Andrew. The Ethics and Conduct of Lawyers in England and Wales. Hart Publishing,1999. — 808 p., 1999
- Griffiths-Baker Janine. Serving Two Masters: Conflicts of Interest in the Modern Law Firm. Hart Publishing,2002. — 227 p., 2002
- Grisso T.. Evaluating Competencies: Forensic Assessments and Instruments. 2nd edition. — Springer,2002. — 564 p., 2002
- Luban David. Legal Ethics and Human Dignity. Cambridge University Press,2007. — 350 p., 2007
- Ayupova Z.K.. Theory of state and law: textbook. - Almaty: Kazakh University,2015. - 192 pages., 2015