Acute Burn Management
The decrease in burn morbidity and mortality seen in recent decades is believed to be related to improved acute care and management of individuals with burns. Pain control has been a major area of emphasis in the care of children with burns in the past decade (135).
Immediate pain management includes using cool saline-soaked gauze or sheets over burned areas. Medications such as acetaminophen or ibuprofen may be used for smaller burns. Children with larger burns may require opioids such as morphine for pain control and benzodiazepines for sedation. With protracted, painful treatment in severe burns, tolerance to these medications develops, and very high doses may be required (136). More recently, protocols using ketamine or dexmedetomidine for sedation, amnesia, and analgesia have been described as safe and effective (137,138). Nonpharmacologic adjuvants for pain control include distraction, music and art therapy, relaxation, massage, hypnosis, and imagery (135).Acute burns are cleaned with a mild soap and water. Ice or very hot or cold water should be avoided. Loose skin should be gently debrided. Controversy exists regarding whether blisters should be unroofed, though there is general agreement that needle aspiration should not be performed (134). Tetanus immunization is provided as needed. Intravenous antibiotics are reserved for those with wound infection and sepsis.
Current burn care practice utilizes topical creams, ointments, and/or semiocclusive dressings in order to promote moist healing and rapid epithelialization. Scar symptoms such as pain, itching, and tightening may be reduced with the use of these products, although the effect on ultimate scar appearance is unclear (139). Superficial burns require moisturizer only because intact dermis will protect against infection (134). There is no evidence to support the use of vitamin E cream or topical onion extract ointment in improving scar appearance (139,140).
Partial-thickness burns usually require once- or twice-daily topical antibiotic ointment such as bacitracin and polymyxin in addition to a nonadhesive dressing such as petroleum or bismuth-impregnated gauze. Full-thickness burns, in which infection is a more significant concern, are covered with an antimicrobial cream such as silver sulfadiazine 1% cream, silver nitrate 0.5% solution, or mafenide acetate 0.5% cream (134). Each has advantages and disadvantages. Larger, deeper wounds generally require dressing changes twice per day because of their increased risk of infection (134).
An alternative acute wound management strategy uses synthetic occlusive dressings, human allograft, or pigskin for smaller, partial-thickness burns. They adhere to the wound until epithelization occurs and are trimmed back daily. One author reported successful use of a single application of xenogenic (porcine) acellular dermal matrix for two weeks at a time after initial debridement (141). Other products, such as Acticoat, a silver ion-impregnated gauze in which ions are released over three to four days, allow for only twice-weekly dressing changes. Improved ability to manage pediatric burns on an outpatient basis using this product compared to silver sulfadiazine has been demonstrated (142).
Burns have increasingly been managed in outpatient settings with frequent wound checks or dressing
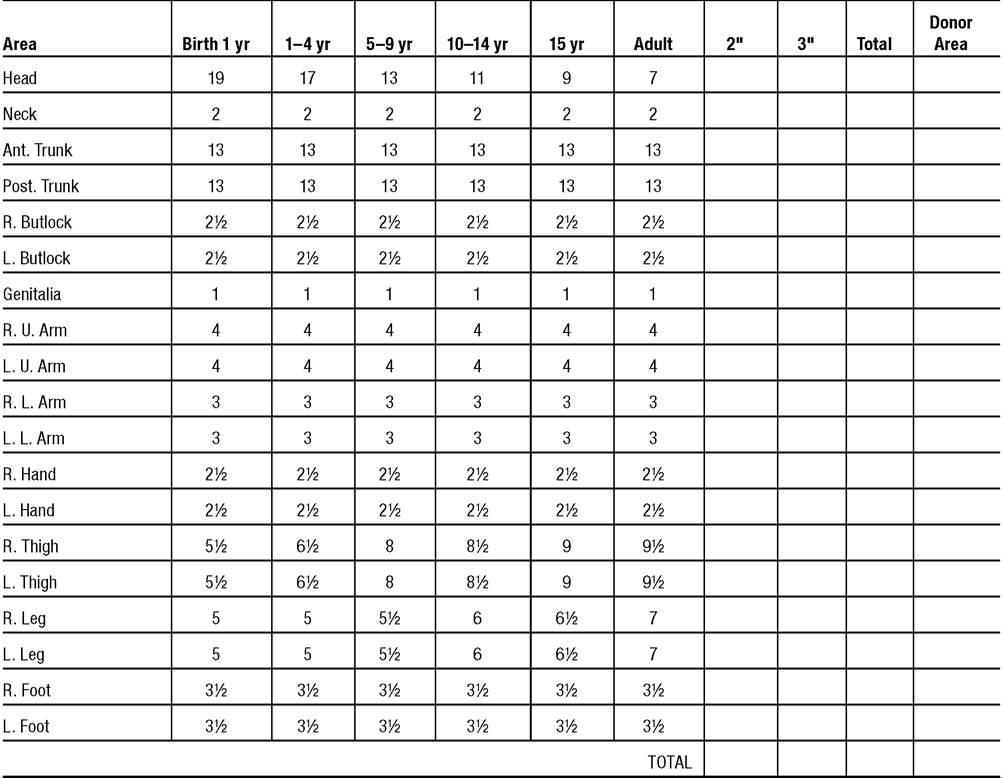
AGE vs. AREA
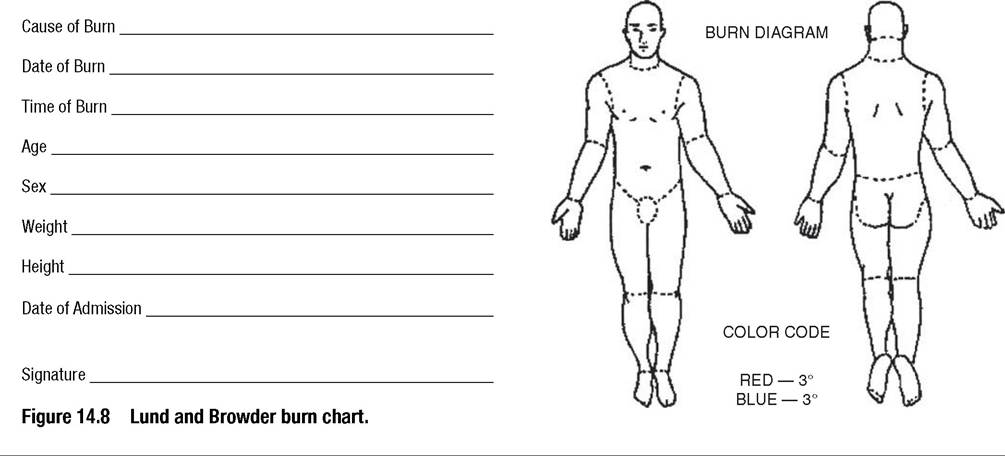
Initial Evaluation UMC.519a, Rev 3.99
changes (130,143). However, partial-thickness burns of greater than 10 % TBSA, full-thickness burns of greater than 2%, and any circumferential burns or burns of the hands, feet, face, or genitals require inpatient treatment (144). Transfer to a burn center is recommended for anyone with burns greater than 20% TBSA or in children under the age of 10 years with greater than 10% TBSA. In addition, individuals with burns complicated by other trauma, child abuse, or medical comorbidities, or burns caused by chemical or electrical exposure should also be transferred to a burn hospital (134,144). An estimated 125 hospitals have specialized burn centers in the United States (124).
About 10% of burn admissions in children are related to child abuse, and about 10% of all abuse cases include burn injuries (145). Features that should raise suspicion for child abuse include symmetric “dip” injuries of the limbs or buttocks, round cigarette or “dropped ash” burns, and prior history of repeated trauma, report of the child or sibling causing the burn, and accompaniment of the child by someone other than the parent (144). An investigator’s checklist is available for use in suspected cases of deliberate burn injuries of children (145).
More on the topic Acute Burn Management:
- Acute Burn Management
- Chronic Burn Management
- TECHNICAL FACTORS OF NEEDLE ELECTROMYOGRAPHY
- Benzodiazepines
- BURNS AND SCALDS
- Pediatric ICU Considerations
- The New Management Incentives
- First aid for burns
- MANAGEMENT OF DOG BITE
- Management