Chronic Burn Management
Whether undergoing ambulatory or inpatient management, rehabilitation is critical in achieving improved outcomes. Gait and mobility training with gait aids may be necessary. Other equipment and adaptive aids may help children and adolescents achieve increased independence in self-care skills.
Range-of- motion and stretching exercises of areas affected by burns must begin in the acute care phase in order to help prevent contracture formation. Positioning to promote functional range of motion and prevent contractures is also important. Splints and other custom-molded orthotics are occasionally necessary to further advance this goal (146,147). Pillows, pads, and other bed-based apparatus may be helpful as well. Optimal positioning based on area burned is summarized (Table 14.2).Children with severe burns may develop low bone density and an increased risk of long bone fracture due to prolonged immobilization, nutritional deficit,s and an alteration of the hormonal milieu (148). Intervention to improve bone density includes mobilization and improved nutritional intake of calcium and vitamin D (149). Treatment with growth hormone for the year following hospitalization in severely burned children has been observed to improve lean body mass, height, weight, strength, cardiac function, and bone mineral content. It is hypothesized that this may lead to a higher daily activity level and result in decreased contracture formation (150).
Positioning of the Pediatric Burn Patient
| AREA INVOLVED | CONTRACTURE PREDISPOSITION | CONTRACTURE PREVENTING POSITION |
| Anterior neck | Flexion | Extension, no pillows |
| Anterior axilla | Shoulder adduction | 90° abduction, neutral Rotation |
| Posterior axilla | Shoulder extension | Shoulder flexion |
| Elbow/ forearm | Flexion/pronation | Elbows extended, forearm supination |
| Wrists | Flexion | 15-20° extension |
| Hands MCPs Ips Palmar burn | Hyperextension Flexion Finger flexion, thumb opposition | 70-90° flexion Full extension All joints full extension, thumb radially abducted |
| Chest | Lateral/anterior Flexion | Straight, no lateral or anterior flexion |
| Hips | Flexion, adduction, external rotation | Extension, 10° abduction, neutral rotation |
| Knees | Flexion | Extension |
| Ankles | Plantarflexion | 90° dorsiflexion |
| MCPs, metacarpophalangeals; IPs, interphalangeals. | ||
14.2
Strength and endurance exercises are important and are facilitated by a physical or occupational therapist.
Studies reveal that children with burns who participated in a resistance exercise program over 12 weeks had improved muscle strength, power, lean body mass (151), and pulmonary function (152) compared to those who participated in a standard rehabilitation program without exercise. There was also a decreased need for surgical release of burn contractures (153).Mustoe and colleagues published clinical guidelines regarding scar management based on systematic literature review and expert consensus (154). The importance of prevention of hypertrophic scarring and keloids was emphasized. When a symptomatic scar has developed, the recommended treatment depends on scar classification (Table 14.3, Fig. 14.9).
Pressure garments have been the mainstay of scar treatment for decades. Proposed mechanisms of action include decreasing collagen synthesis by decreasing blood flow and realigning collagen bundles already present. A decrease in hypertrophic scar
14.3
Burn Scar Classification
Mature scar: A light-colored, flat scar
Immature scar: A red, sometimes itchy or painful, and slightly elevated scar in the process of remodeling. Many of these will mature normally over time and become flat, and assume a pigmentation that is similar to the surrounding skin, although they can be paler or slightly darker.
Linear hypertrophic (e.g., surgical/traumatic) scar: A red, raised, sometimes itchy scar confined to the border of the original surgical incision. This usually occurs within weeks after surgery. These scars may increase in size rapidly for 3-6 months and then, after a static phase, begin to regress. They generally mature to have an elevated, slightly rope-like appearance with increased width, which is variable. The full maturation process may take up to 2 years.
Widespread hypertrophic (e.g., burn) scar: A widespread red, raised, sometimes itchy scar that remains within the borders of the burn injury.
Minor keloid: A focally raised, itchy scar extending over normal tissue.
This may Develop up to 1 year after injury and does not regress on its own. Simple Surgical excision is often followed by recurrence. There may be a genetic Abnormality involved in keloid scarring. Typical sites include earlobes.Major keloid: A large, raised (>0.5 cm) scar, possibly painful or pruritic and extending over normal tissue. This often results from minor trauma and can continue to spread over years.
formation reduces the incidence of contractures as well as pain and itchiness (155). Pressure over scars may be achieved through traditional off-the-shelf or custom pressure garments. Care should be taken to avoid wound irritation from seams or zippers. Pressure is usually initiated after wound closure, and garments are worn 23 hours per day for 6-24 months (144), or until scar maturation. Garments should be replaced every 6-12 weeks in order to maintain compression. Over time, garment alterations may be necessary due to limb size fluctuation and growth of the child. The pressure required for effective treatment has not been scientifically established (155). Some have suggested 24-35 mmHg (154), while others have described improvement with pressures as low as 15 mmHg (156). Complications such as discomfort and skin breakdown occasionally result from the use of pressure dressings. High pressures may cause harm such as obstructive sleep apnea (157) or skeletal and dental deformity in children (158).
It is important to note that although pressure dressings are routinely used to prevent and treat burn scars, little scientific evidence exists to support their use (139,154,159). In fact, one prospective, randomized trial of the efficacy of pressure garment therapy showed no significant differences in burn outcome parameters using the Vancouver Burn Scar Assessment between one group that used pressure garments and another that did not (160).
There is some evidence to support the use of silicone dressings to prevent hypertrophic scars in those at risk as well as to improve scar elasticity in already existing symptomatic scars (139,161).
Vigorous scar massage may help to keep scars supple. Massage techniques are performed by a skilled therapist and are taught to the patient or family. Exercise and scar modification techniques should continue over the 12-24 months necessary for scar maturation (144).Additional management options for keloids and recalcitrant hypertrophic scars include the injection of triamcinolone (154). Topical steroids and vitamin E creams have not been successfully used for scar treatment (162). Radiotherapy, laser therapy, and cryotherapy have been used with mixed results (154).
In the acute period, a surgical referral should be made if the burn wound has not healed within a week. Skin grafting may be considered, with the goal of preventing later scar complications (144). Mature scars require surgical intervention when functional loss or cosmesis can be restored or improved. Later, when a hypertrophic scar, keloid, or contracture has developed, surgical interventions include scar excision, skin grafts, reorientation of scars using flaps, W- or Z-plasties, contracture release, and use of skin substitutes or tissue expansion. Surgical excision of hypertrophic scars and keloids without additional treatment results in a high rate of recurrence. Similarly, surgical correction of equinus contractures using the Ilizarov method resulted in recurrence rates of approximately 70% in younger children (163). However, surgical excision in combination with the use of adhesive microporous hypoallergenic paper tape, silicone gel sheeting, steroid injection, or even radiation therapy may decrease the likelihood of recurrence (154).
Outcome
The most common complication for burn survivors is abnormal or hypertrophic scarring, though the actual prevalence is unknown (164). Abnormal scarring may cause contractures and impaired function. Scar contraction may lead to growth restriction in a child, with resultant distortion of anatomical features and disfigurement. Based on a Medline review of 50 studies related to functional outcomes after burn injury, limited range of motion was reported in 0% to 5% of children with minor burns (mean TBSA 6%) and 47% with massive burns (>80% TBSA).
One-third of the children with massive burns were dependent on others for assistance for activities of daily living years after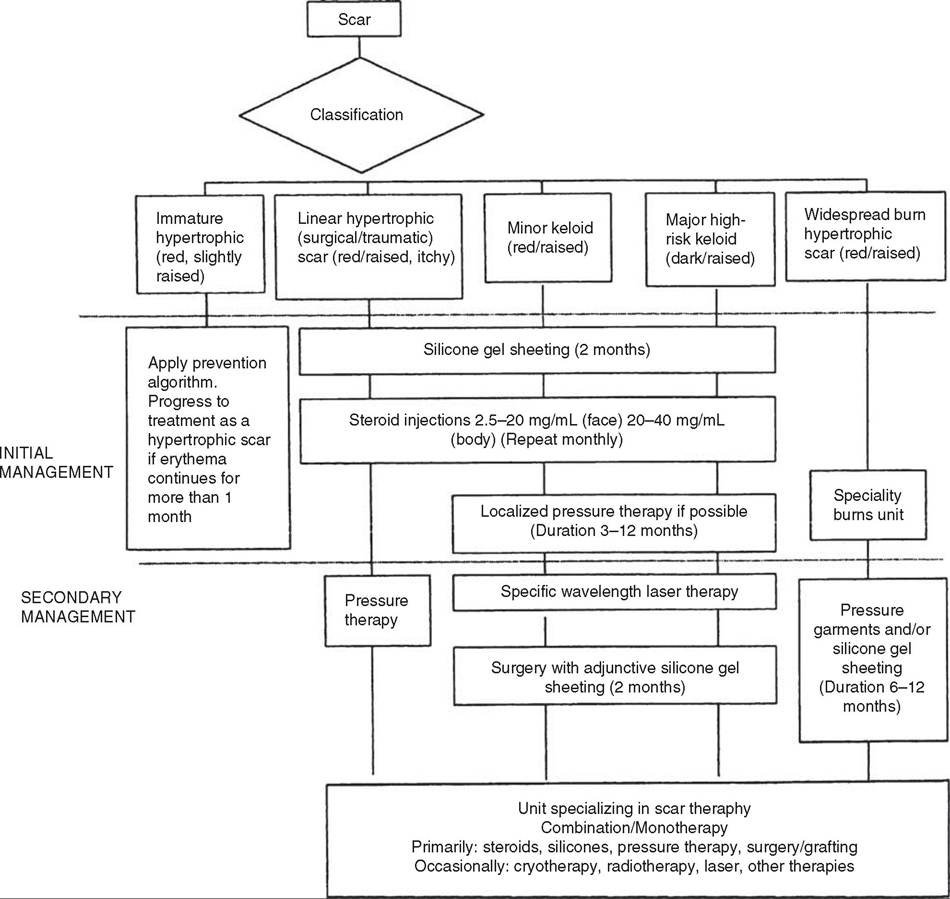
Figure 14.9 Complete burn management algorithm.
injury. It was felt that insufficient data exist to fully describe the burden of burn injuries (165). In a study of adult survivors of massive burns, quality of life was comparable to the general population. The strongest independent predictors of physical quality of life were size of full-thickness injury and hand function. Mental quality of life was best predicted by age at the time of injury (with younger age predicting a better quality of life) and perceived social support (166).
Following a burn injury, children have an increased incidence of psychological disturbance (167) and difficulty with behavior (165). Significantly higher levels of anxiety, phobias, and enuresis have been noted in this population, and 30% met criteria for post- traumatic stress disorder (PTSD) within six months of their burn (168). Pain, separation anxiety, and acute dissociation have been found to contribute to the development of PTSD (169). Feelings of depression and misery were reported by 79% of children with burns in another study (167). Self-esteem and confidence may decline. Fourteen percent to forty-three percent of individuals report dissatisfaction with appearance after a burn (165). Social reintegration may be difficult and social isolation prevalent, with a third having symptoms of antisocial disorder (167). One-fourth to one-third of children with burns experienced interference in playing with other children or seeing friends (165). Return to school and community activities may be eased by education provided to the child's peers and teachers prior to their return.