I ABNORMAL GENITAL BLEEDING ^461 ^593
Any bleeding other than what is expected in a normal ovulatory cycle is considered abnormal genital bleeding. Abnormal genital bleeding is one of the most common reasons for a woman to seek gynecologic care.
The source of abnormal genital bleeding may be difficult to assess; it may be the rectum, the urinary tract, or the vulva, vagina, cervix, or uterus. The uterus is the source of most abnormal genital bleeding in adult women. Abnormal uterine bleeding (AUB) is a generic term that is a subclassification of genital bleeding. Physical examination readily distinguishes between the two, and each have a separate set of etiologies and treatments (see also “Abnormal Uterine Bleeding” later in this section).A wide variety of conditions can cause the bleeding, including trauma, infection, endocrine or medical abnormalities, lesions, tumors, or neoplasm. It is also possible for contraception or pregnancy to be an etiologic factor. If genital bleeding is secondary to trauma, the differential diagnosis should include rape and abuse. Research into abnormal genital bleeding has been limited by a lack of widely accepted, high-quality and validated outcome measures that are objective and take into account patient quality of life measures. Nevertheless, there are a number of useful diagnostic tools and effective therapeutic options for the woman with abnormal genital bleeding.
Evaluation, Diagnosis, and Management
The following is an ordering of the differential diagnosis for abnormal genital bleeding, based on the age of the patient when symptoms occur:
• In children, the source of abnormal genital bleeding can include foreign bodies, vaginitis, urethral prolapse, neoplasm, trauma, and precocious puberty (see also the “Pediatric Gynecology” section in Part 3).
• In adolescents, abnormal genital bleeding most often occurs as a result of persistent anovulation, including anovulation caused by polycystic ovary syndrome (PCOS) and contraception.
Pregnancy, pelvic infections, and coagulopathies (in as many as 19% of adolescents who require hospitalization) also are common in adolescents. Tumors also should be considered.• Women in the second through fourth decades of life most often develop abnormal genital bleeding from pregnancy, structural lesions (eg, leiomyomas and polyps), anovulation (eg, PCOS), and hormonal contraception. Endometrial hyperplasia (or atrophy) and endometrial cancer also should be considered.
• Menopausal women most often develop bleeding from hormone therapy, endometrial atrophy, leiomyomas, endometrial hyperplasia, and malignancy.
Less common causes of abnormal genital bleeding include the following:
• Vascular anomalies of the uterus
• Infection
• Cirrhosis
• Drug therapy (ie, other than hormonal treatment)
• Thyroid dysfunction
An accurate diagnosis for the cause of bleeding should be established. Medical history should include a structured menstrual history that includes questions about heaviness of bleeding, duration, interval, regularity, and pain; family history of bleeding problems; and the use of medications or herbal supplements. A general physical examination, speculum examination, and bimanual examination should be completed. Proper evaluation of abnormal genital bleeding also may include the following:
• Evaluation for pregnancy
• Complete blood count and measurement of thyroid-stimulating hormone level
• Examination for lower genital tract lesions
• Cervical cytology
• Evaluation for infection or sexually transmitted infections
• Evaluation for endocrine dysfunction, such as PCOS
• Evaluation for bleeding disorder
• Evaluation for trauma or sexual assault (Clinicians should be familiar with any state reporting requirements regarding evidence of abuse or intimate partner violence and sexually transmitted infections; see also the “Sexually Transmitted Infections” section and the “Abuse” section in Part 3.)
• Endometrial biopsy
• Ultrasonography (transvaginal or transabdominal, depending on the patient’s age and the indication)
• Sonohysterography
• Hysteroscopy
The management of abnormal genital bleeding varies greatly, depending on the underlying disorder.
Medication, an office procedure, or surgery may be required, depending on the etiology, the patient’s age, and the patient’s reproductive status. A discussion of the evaluation and management of AUB follows.Abnormal Uterine Bleeding ^573
Abnormal uterine bleeding is any bleeding from the uterus that is abnormal in volume, duration, frequency, or regularity. It is a symptom with many different etiologies.
Classification and Etiology of Abnormal Uterine Bleeding
Descriptive terms that traditionally have been used to characterize abnormal menstrual bleeding patterns include menorrhagia, metrorrhagia, polymenorrhea, and oligomenorrhea. Menorrhagia, or heavy menstrual bleeding, is defined as menstrual blood loss greater than 80 mL. (However, this definition is used for research purposes and, in practice, excessive blood loss should be based on the patient’s perception.) Metrorrhagia is defined as bleeding between periods. Polymenorrhea is defined as bleeding that occurs more often than every 21 days, and oligomenorrhea is defined as bleeding that occurs less frequently than every 35 days.
In 2011, to remedy the confusion surrounding nomenclature for AUB, the International Federation of Gynecology and Obstetrics (FIGO) introduced a new classification system, the adoption of which is supported by the American College of Obstetricians and Gynecologists. With this system, AUB is classified by pattern and etiology (Fig. 4-1). The term dysfunctional uterine bleeding, formerly used to describe AUB without a systematic or structural cause, should no longer be used.
A major cause of AUB (after pregnancy is ruled out) is uterine leiomyomas (commonly known as fibroids). These are the most common solid tumors in women and are the leading indication for hysterectomy, most often for AUB and pelvic pressure. An example of the PALM-COEIN
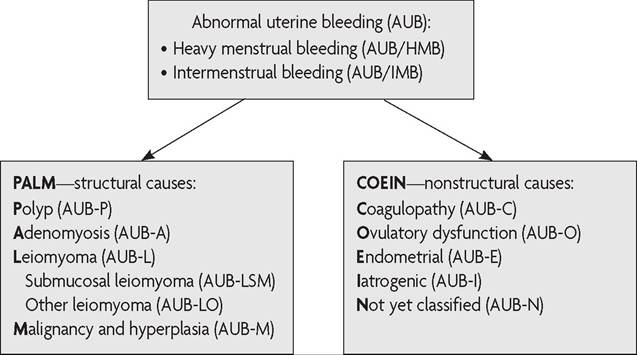
Fig. 4-1. Basic PALM-COEIN classification system for the causes of abnormal uterine bleeding in nonpregnant reproductive-aged women.
This system, approved by the International Federation of Gynecology and Obstetrics, uses the term “abnormal uterine bleeding” paired with terms that describe associated bleeding patterns (“heavy menstrual bleeding” or “intermenstrual bleeding”), a qualifying letter (or letters) to indicate its etiology (or etiologies), or both. (Modified from Munro MG, Critchley HO, Broder MS, Fraser IS. FIGO classification system [PALM-COEIN] for causes of abnormal uterine bleeding in nongravid women of reproductive age. FIGO Working Group on Menstrual Disorders. Int J Gynaecol Obstet 2011;113:3-13.)terminology used for symptomatic uterine leiomyomas is AUB-L (abnormal uterine bleeding-leiomyoma). Another very common, nonstructural cause of AUB is ovulatory dysfunction, which often is the result of an endo- crinopathy, such as PCOS. The new terminology for this etiology is AUB-O (abnormal uterine bleeding-ovulatory dysfunction).
Women with undiagnosed coagulopathies may present initially with AUB. These disorders include defects in primary hemostasis, platelet deficiency (leukemia or idiopathic thrombocytopenia), platelet dysfunction (von Willebrand disease), and abnormalities of secondary hemostasis (congenital factor deficiencies). Von Willebrand disease is the most common inherited bleeding disorder among American women, with a prevalence of 0.6-1.3%. The overall prevalence is even greater among women with chronic heavy menstrual bleeding, and ranges from 5% to 24%. A diagnosis of von Willebrand disease will have significant implications for the woman’s future gynecologic and obstetric care. Given the prevalence and the consequences of such a diagnosis, hematologic disorders should be considered in all patients presenting with AUB or heavy menstrual bleeding, especially adolescents with a sudden onset of AUB or heavy menstrual bleeding at menarche.
Evaluation and Diagnosis of Abnormal Uterine Bleeding
The initial evaluation of patients with AUB is similar to that for patients with abnormal genital bleeding and includes a thorough medical history and physical examination, appropriate laboratory and imaging tests, and consideration of age-related factors (see also “Evaluation, Diagnosis, and Management” of abnormal genital bleeding earlier in this section).
An initial screening for an underlying disorder of hemostasis should be performed. In all adolescents with heavy menstrual bleeding and adult patients with a positive screening history for a bleeding disorder, laboratory testing is indicated. Initial tests should include a complete blood count with platelets, prothrombin time, and partial thromboplastin time (fibrinogen or thrombin time are optional); bleeding time is neither sensitive nor specific, and is not indicated. Depending on the results of the initial tests, or if a patient’s medical history is suggestive of an underlying bleeding condition, specific tests for von Willebrand disease or other coagulopathies may be indicated.
Any patient with an abnormal physical examination, such as an enlarged or globular uterus on bimanual examination, should undergo transvaginal ultrasonography to evaluate for myomas and adenomyosis. When symptoms persist despite treatment in the setting of a normal pelvic examination, further evaluation is indicated with transvaginal ultrasonography, biopsy, or both if not already performed. When there is clinical suspicion for endometrial polyps or submucosal leiomyomas, sonohysterography or hysteroscopy will enable better detection of lesions.
Endometrial tissue sampling should be performed in patients with AUB who are older than 45 years as a first-line test. Endometrial sampling also should be performed in patients younger than 45 years with a history of unopposed estrogen exposure (such as seen in obesity or PCOS), failed medical management, and persistent AUB. An office endometrial biopsy is the first-line procedure for tissue sampling in the evaluation of patients with AUB. Other evaluation methods, such as transvaginal ultrasonography, sonohysterography, or office hysteroscopy also may be necessary when the endometrial biopsy is insufficient, nondiagnostic, or cannot be performed.
Transvaginal ultrasonography in postmenopausal women with bleeding has an extremely high negative predictive value for endometrial cancer when 4 mm is used as a cut-off.
An endometrial thickness of greater than 4 mm or inability to visualize thickness, however, should be evaluated with another method, such as endometrial biopsy, sonohysterography, or office hysteroscopy. Ultrasonographic measurement of endometrial thickness is of limited value in detecting benign abnormalities in the premenopausal woman as compared with its ability to exclude malignancy in the postmenopausal woman. Thus, measurement of endometrial thickness in premenopausal women is not helpful in the evaluation of AUB.Sonohysterography is a procedure that can be performed in an office setting by a qualified individual. It has the ability to delineate abnormalities in the uterine cavity that may be missed with routine transvaginal ultrasonography and does so without radiation exposure or significant discomfort to the patient. It is important to ensure that the patient is not pregnant, so scheduling during the follicular phase or after a course of progestin should be considered.
Hysteroscopy may be performed in an office setting or in the operating room. Hysteroscopy allows direct visualization of endometrial cavity abnormalities and the ability to take directed biopsies. Hysteroscopy is highly accurate in diagnosing endometrial cancer but less useful for detecting hyperplasia.
Routine use of magnetic resonance imaging in the evaluation of AUB is not recommended. However, magnetic resonance imaging may be useful to guide the treatment of leiomyomas, particularly when the uterus is enlarged, contains multiple leiomyomas, or precise leiomyoma mapping is of clinical importance.
Management of Abnormal Uterine Bleeding
The primary goal of management is to treat the underlying disorder. A universal single approach in the management of all patients with AUB is not feasible or appropriate. In general, treatment options depend on the following:
• Suspected etiology—an underlying coagulopathy should be considered in all patients (particularly adolescents) when AUB is not otherwise explained, does not respond to medical therapy, or both
• Frequency and quantity of bleeding
• Patient age
• Health status
• Reproductive plans
Many causes of AUB are amenable to medical management. Decisions should be based on the patient’s medical history and contraindications to therapies. The treatment of choice for AUB-O if carcinoma is not a concern or has been ruled out is medical therapy. Medical treatment options for AUB-O include progestin therapy and combined hormonal contraception. Medical management should be the initial treatment for most patients with acute AUB, if clinically appropriate. Options include intravenous conjugated equine estrogen, multidose regimens of oral contraceptives or oral progestins, and tranexamic acid. Antifibrinolytic drugs, such as tranexamic acid, work by preventing fibrin degradation and are effective treatments for patients with chronic AUB.
The need for surgical treatment is based on the clinical stability of the patient, the severity of bleeding, contraindications to medical management, the patient’s lack of response to medical management, and the underlying medical condition of the patient. Surgical options include dilation and curettage (D&C), endometrial ablation, uterine artery embolization, and hysterectomy. The choice of surgical modality (eg, D&C versus hysterectomy) is based on the aforementioned factors plus the patient’s desire for future fertility. Specific treatments, such as hysteroscopy with D&C, polypectomy, or myomectomy, may be required if structural abnormalities are suspected as the cause of acute AUB (see also the “Leiomyomas” section later in Part 4). Dilation and curettage alone (without hysteroscopy) is an inadequate tool for evaluation of uterine disorders and may provide only a temporary reduction in bleeding (cycles after the D&C will not be improved). Dilation and curettage with concomitant hysteroscopy may be of value for those patients in whom intrauterine pathology is suspected or a tissue sample is desired. Case reports of uterine artery embolization and endometrial ablation show that these procedures successfully control acute AUB. Endometrial ablation, although readily available in most centers, should be considered only if other treatments have been ineffective or are contraindicated, and it should be performed only when a woman does not have plans for future childbearing and when the possibility of endometrial or uterine cancer has been reliably ruled out as the cause of the acute AUB. Hysterectomy, the definitive treatment for controlling heavy bleeding, may be necessary for patients who do not respond to medical therapy.
Bibliography
American College of Obstetricians and Gynecologists. General management of pediatric gynecology patients. Guidelines for adolescent health care [CD-ROM]. 2nd ed. ed. Washington, DC: American College of Obstetricians and Gynecologists; 2011. p. 172-92.
Diagnosis of abnormal uterine bleeding in reproductive-aged women. Practice Bulletin No. 128. American College of Obstetricians and Gynecologists. Obstet Gynecol 2012;120:197-206. [PubMed] [Obstetrics & Gynecology]
Endometrial ablation. ACOG Practice Bulletin No. 81. American College of Obstetricians and Gynecologists. Obstet Gynecol 2007;109:1233-48. [PubMed] [Obstetrics & Gynecology]
Fraser IS, Critchley HO, Munro MG, Broder M. A process designed to lead to international agreement on terminologies and definitions used to describe abnormalities of menstrual bleeding. Writing Group for this Menstrual Agreement Process. Fertil Steril 2007;87:466-76. [PubMed] [Full Text]
James AH. Obstetric management of adolescents with bleeding disorders. J Pediatr Adolesc Gynecol 2010;23:S31-7. [PubMed] [Full Text]
James AH. Von Willebrand disease. Obstet Gynecol Surv 2006;61:136-45. [PubMed] Kadir RA, Economides DL, Sabin CA, Owens D, Lee CA. Frequency of inherited bleeding disorders in women with menorrhagia. Lancet 1998;351:485-9. [PubMed] [Full Text]
Long-acting reversible contraception: implants and intrauterine devices. Practice bulletin No. 121. American College of Obstetricians and Gynecologists. Obstet Gynecol 2011;118:184-96. [PubMed] [Obstetrics & Gynecology]
Management of abnormal uterine bleeding associated with ovulatory dysfunction. Practice Bulletin No. 136. American College of Obstetricians and Gynecologists. Obstet Gynecol 2013;122:176-85. [PubMed] [Obstetrics & Gynecology]
Management of acute abnormal uterine bleeding in nonpregnant reproductive- aged women. Committee Opinion No. 557. American College of Obstetricians and Gynecologists; Obstet Gynecol 2013;121:891-6. [PubMed] [Obstetrics & Gynecology] Matteson KA, Boardman LA, Munro MG, Clark MA. Abnormal uterine bleeding: a review of patient-based outcome measures. Fertil Steril 2009;92:205-16. [PubMed] [Full Text]
Menstruation in girls and adolescents: using the menstrual cycle as a vital sign. ACOG Committee Opinion No. 349. American College of Obstetricians and Gynecologists. Obstet Gynecol 2006;108:1323-8. [PubMed] [Obstetrics & Gynecology]
Munro MG, Critchley HO, Broder MS, Fraser IS. FIGO classification system (PALM- COEIN) for causes of abnormal uterine bleeding in nongravid women of reproductive age. FIGO Working Group on Menstrual Disorders. Int J Gynaecol Obstet 2011;113:3-13. [PubMed] [Full Text]
Noncontraceptive uses of hormonal contraceptives. Practice Bulletin No. 110. American College of Obstetricians and Gynecologists. Obstet Gynecol 2010; 115:206-18. [PubMed] [Obstetrics & Gynecology]
Shankar M, Lee CA, Sabin CA, Economides DL, Kadir RA. von Willebrand disease in women with menorrhagia: a systematic review. BJOG 2004;111:734-40. [PubMed] [Full Text]
Sharp HT. Assessment of new technology in the treatment of idiopathic menorrhagia and uterine leiomyomata. Obstet Gynecol 2006;108:990-1003. [PubMed] [Obstetrics & Gynecology]
Sonohysterography. Technology Assessment in Obstetrics and Gynecology No. 8. American College of Obstetricians and Gynecologists. Obstet Gynecol 2012;119: 1325-8. [Obstetrics & Gynecology]
The role of transvaginal ultrasonography in the evaluation of postmenopausal bleeding. ACOG Committee Opinion No. 440. American College of Obstetricians and Gynecologists. Obstet Gynecol 2009;114:409-11. [Obstetrics & Gynecology]
Von Willebrand disease in women. Committee Opinion No. 580. American College of Obstetricians and Gynecologists. Obstet Gynecol 2013;122:1368-73. [PubMed] [Obstetrics & Gynecology]
Resources
American College of Obstetricians and Gynecologists. Abnormal uterine bleeding. Patient Education Pamphlet AP095. Washington, DC: American College of Obstetricians and Gynecologists; 2012.
American College of Obstetricians and Gynecologists. Endometrial ablation. Patient Education Pamphlet AP134. Washington, DC: American College of Obstetricians and Gynecologists; 2009.
American College of Obstetricians and Gynecologists. Perimenopausal bleeding and bleeding after menopause. Patient Education Pamphlet AP162. Washington, DC: American College of Obstetricians and Gynecologists; 2010.
Learman LA, Nakagawa S, Gregorich SE, Jackson RA, Jacoby A, Kuppermann M. Success of uterus-preserving treatments for abnormal uterine bleeding, chronic pelvic pain, and symptomatic fibroids: age and bridges to menopause. Am J Obstet Gynecol 2011;204:272.e1-7. [PubMed] [Full Text]